
Table of Contents
Introduction
Enbrel is the brand name of etanercept, a biologic disease-modifying antirheumatic drug used in several chronic inflammatory autoimmune diseases. Pharmacologically, etanercept is a tumor necrosis factor blocker, commonly called a TNF inhibitor or anti-TNF drug.
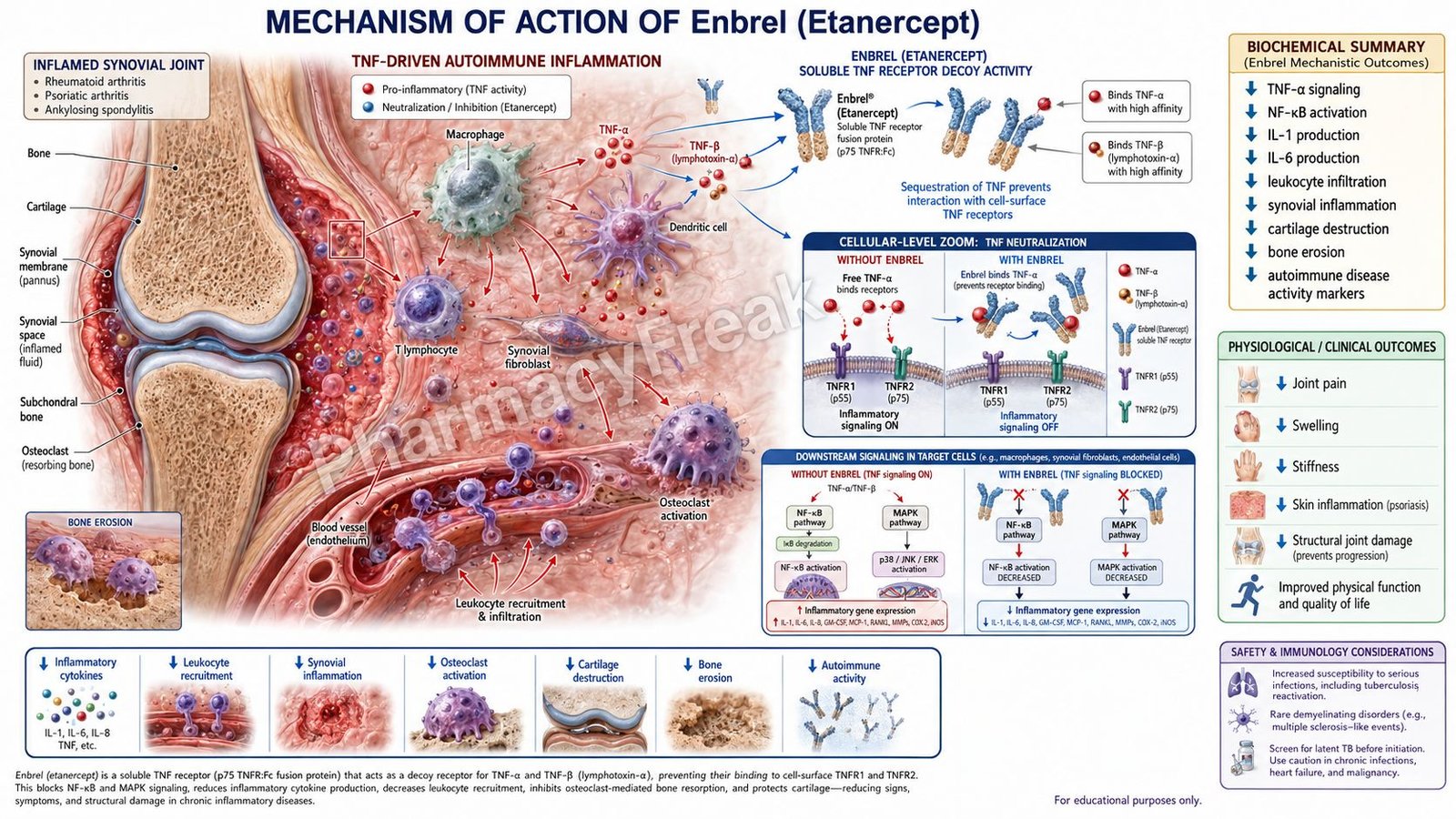
Tumor necrosis factor, especially TNF-alpha, is a major pro-inflammatory cytokine involved in immune activation, leukocyte migration, synovial inflammation, cartilage damage, bone erosion, keratinocyte activation, and systemic inflammatory symptoms. Excessive TNF activity plays an important role in rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, plaque psoriasis, polyarticular juvenile idiopathic arthritis, and juvenile psoriatic arthritis.
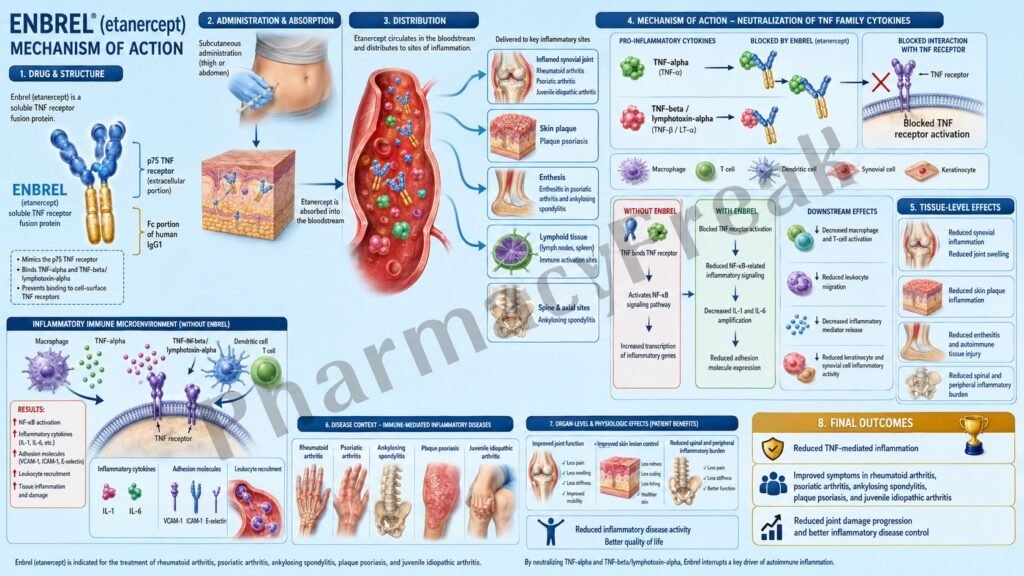
Etanercept is not a conventional small-molecule drug. It is a recombinant dimeric fusion protein made from the extracellular ligand-binding portion of the human p75 TNF receptor linked to the Fc portion of human IgG1. This structure allows it to act like a soluble decoy receptor for TNF. Instead of allowing TNF to bind cell-surface TNF receptors, etanercept binds TNF in circulation and tissues, making TNF biologically inactive. The U.S. label describes Enbrel as a TNF blocker administered by subcutaneous injection, with approved adult indications including rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, and plaque psoriasis, and pediatric indications including polyarticular juvenile idiopathic arthritis, juvenile psoriatic arthritis, and plaque psoriasis in specified age groups.
For exam purposes, Enbrel should be remembered as a soluble TNF receptor-Fc fusion protein that binds TNF-alpha and TNF-beta, prevents TNF receptor activation, and reduces inflammatory cytokine signaling. Its most important safety warnings are serious infections and malignancies.
Mechanism of Action (Step-wise)
Step 1: TNF is produced during inflammation
TNF-alpha is produced mainly by activated macrophages, T cells, natural killer cells, and other immune cells. It is released during immune activation and plays a central role in inflammatory diseases affecting joints, skin, spine, and entheses.
Step 2: TNF binds to cell-surface TNF receptors
TNF normally acts by binding to TNF receptors on target cells. Two major TNF receptors are TNFR1, also called p55, and TNFR2, also called p75. Binding of TNF to these receptors triggers inflammatory signaling inside the cell.
Step 3: TNF receptor activation increases inflammatory signaling
Once TNF binds to its receptors, intracellular pathways such as NF-kB, MAPK, and other inflammatory signaling cascades are activated. These pathways increase transcription of inflammatory genes.
Step 4: Pro-inflammatory mediators increase
TNF signaling increases cytokines, chemokines, adhesion molecules, prostaglandin-related mediators, and matrix metalloproteinases. These substances recruit inflammatory cells, increase vascular permeability, and promote tissue damage.
Step 5: TNF contributes to joint inflammation and destruction
In rheumatoid arthritis and psoriatic arthritis, TNF promotes synovitis, pannus formation, cartilage degradation, bone erosion, pain, swelling, stiffness, and progressive joint damage. It also increases expression of adhesion molecules that help leukocytes migrate into inflamed synovium.
Step 6: TNF contributes to skin and axial inflammation
In plaque psoriasis, TNF contributes to keratinocyte activation, inflammatory cell recruitment, plaque formation, erythema, scaling, and chronic skin inflammation. In ankylosing spondylitis and other spondyloarthropathies, TNF contributes to spinal inflammation, enthesitis, pain, stiffness, and reduced mobility.
Step 7: Enbrel acts as a soluble decoy TNF receptor
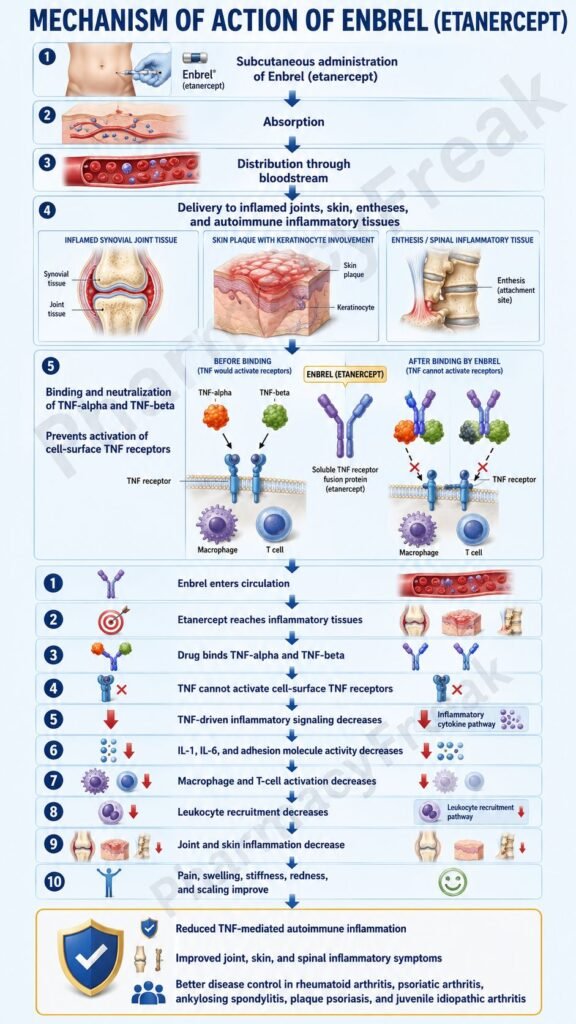
Etanercept is a dimeric soluble form of the p75 TNF receptor fused to human IgG1 Fc. It binds TNF molecules before they can bind natural cell-surface TNF receptors. This decoy receptor mechanism is the central pharmacological action of Enbrel.
Step 8: Enbrel binds TNF-alpha and TNF-beta
Etanercept binds both TNF-alpha and TNF-beta, also called lymphotoxin-alpha. By binding these TNF molecules, etanercept prevents them from activating cell-surface TNF receptors. The official label states that etanercept inhibits binding of TNF-alpha and TNF-beta to cell-surface TNF receptors, rendering TNF biologically inactive.
Step 9: TNF receptor activation decreases
Because TNF is trapped by etanercept, less TNF reaches TNFR1 and TNFR2 on inflammatory target cells. This reduces TNF-driven receptor signaling.
Step 10: Inflammatory cytokine production decreases
Reduced TNF receptor signaling decreases production of inflammatory mediators such as IL-1, IL-6, GM-CSF, chemokines, adhesion molecules, and matrix metalloproteinases. This helps reduce inflammatory cell recruitment and tissue destruction.
Step 11: Leukocyte migration and tissue inflammation decrease
TNF normally increases adhesion molecules such as E-selectin and ICAM-1, which help leukocytes enter inflamed tissues. Etanercept reduces TNF-regulated adhesion molecule expression and lowers inflammatory cell movement into joints, skin, and other tissues.
Step 12: Joint damage and skin inflammation improve
In inflammatory arthritis, decreased TNF signaling reduces pain, swelling, morning stiffness, synovitis, and structural damage progression. In plaque psoriasis, it reduces inflammatory plaque formation and improves scaling and erythema.
Step 13: Enbrel does not primarily lyse TNF-expressing cells
A key exam distinction is that etanercept mainly acts as a soluble receptor that neutralizes TNF. It is not primarily designed to kill TNF-expressing cells. The label notes that cells expressing transmembrane TNF that binds Enbrel are not lysed in vitro in the presence or absence of complement.
Step 14: Final therapeutic outcome
The final therapeutic effect is reduced TNF-mediated inflammation. This improves signs and symptoms of autoimmune inflammatory disease, reduces progression of structural joint damage in selected arthritis indications, and improves physical function and quality of life in appropriate patients.
Pharmacokinetics
Enbrel is administered by subcutaneous injection. It is not given orally because etanercept is a large protein biologic that would be degraded in the gastrointestinal tract.
In adults with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis, a common recommended dose is 50 mg once weekly. In adult plaque psoriasis, an induction regimen of 50 mg twice weekly for 3 months may be used, followed by 50 mg once weekly. In pediatric indications, dosing is weight-based, commonly 0.8 mg/kg once weekly up to a maximum of 50 mg per week.
After subcutaneous administration, etanercept is absorbed slowly. In rheumatoid arthritis patients receiving a single 25 mg subcutaneous dose, the label reports a mean half-life of about 102 hours and time to maximum concentration of about 69 hours. This long half-life supports weekly or twice-weekly dosing schedules depending on indication.
Etanercept is a biologic fusion protein and is not primarily metabolized by hepatic cytochrome P450 enzymes. Like endogenous proteins, it is expected to be degraded into smaller peptides and amino acids through proteolytic catabolic pathways. Therefore, classic CYP-mediated drug interactions are not the main concern.
Because Enbrel suppresses TNF-mediated immunity, the most important pharmacological monitoring relates to infection risk rather than routine drug-level monitoring. Patients should be screened for latent tuberculosis before starting therapy and monitored for infection during treatment.
Live vaccines should generally be avoided during Enbrel therapy. Combination with certain biologic immunomodulators such as anakinra or abatacept is not recommended because of increased infection risk and lack of added clinical benefit.
Clinical Uses
Enbrel is used in moderately to severely active rheumatoid arthritis. It reduces signs and symptoms, improves physical function, induces major clinical response, and inhibits progression of structural joint damage. It can be used alone or with methotrexate.
Enbrel is used in polyarticular juvenile idiopathic arthritis in patients 2 years of age and older. It helps reduce signs and symptoms of moderately to severely active disease.
Enbrel is used in adult psoriatic arthritis. It reduces signs and symptoms, improves physical function, and inhibits progression of structural damage. It can be used with or without methotrexate.
Enbrel is used in active ankylosing spondylitis. It reduces inflammatory spinal symptoms such as pain and stiffness and improves function in appropriate patients.
Enbrel is used in chronic moderate-to-severe plaque psoriasis in patients 4 years of age and older who are candidates for systemic therapy or phototherapy. It reduces TNF-mediated skin inflammation and plaque activity.
Enbrel is also indicated for juvenile psoriatic arthritis in patients 2 years of age and older, reflecting its role in pediatric inflammatory arthritis with psoriatic features. The 2024 U.S. prescribing information lists juvenile psoriatic arthritis as a recent major update to indications and pediatric dosing sections.
Enbrel is not a steroid, NSAID, painkiller, antibiotic, or immediate rescue medicine. It is a disease-modifying biologic therapy used for long-term control of selected immune-mediated inflammatory diseases.
Adverse Effects
The most important safety warning with Enbrel is serious infection. TNF is important for host defense against intracellular organisms, granuloma maintenance, and immune control of certain bacterial, fungal, viral, and opportunistic infections. Blocking TNF can increase the risk of infections that may require hospitalization or may be fatal. The boxed warning lists serious infections including tuberculosis, bacterial sepsis, invasive fungal infections such as histoplasmosis, and other opportunistic infections.
Tuberculosis is a major exam-relevant warning. Patients should be tested for latent TB before starting Enbrel. If latent TB is present, treatment should be started before Enbrel. Patients should also be monitored for active TB during therapy, even if the initial latent TB test was negative.
Malignancy is another boxed warning. Lymphoma and other malignancies, some fatal, have been reported in children and adolescent patients treated with TNF blockers, including Enbrel. The risk must be interpreted carefully because underlying inflammatory diseases may also affect malignancy risk, but the warning remains clinically important.
The most common adverse effects are infections and injection-site reactions. Injection-site reactions may include redness, itching, pain, swelling, bruising, or irritation at the injection site.
Neurologic reactions may occur, including new onset or worsening demyelinating disease. Enbrel should be used cautiously in patients with a history of multiple sclerosis, optic neuritis, transverse myelitis, or other demyelinating disorders.
New onset or worsening congestive heart failure has been reported with TNF blockers. Patients with heart failure should be monitored carefully, and therapy may need reconsideration if symptoms worsen.
Hematologic reactions can occur, including rare pancytopenia and aplastic anemia. Warning symptoms include persistent fever, bruising, bleeding, or pallor.
Hepatitis B reactivation can occur in patients previously infected with hepatitis B virus. Patients at risk should be evaluated and monitored during and after therapy.
Hypersensitivity reactions, including anaphylaxis and serious allergic reactions, may occur. Enbrel should be discontinued if a serious allergic reaction occurs.
Autoimmune reactions such as lupus-like syndrome and autoimmune hepatitis have been reported. If lupus-like syndrome or autoimmune hepatitis develops, Enbrel should be stopped.
Live vaccines should generally be avoided during therapy. Concurrent use with anakinra or abatacept is not recommended because of increased serious infection risk. Cyclophosphamide combination is also not recommended in certain settings.
Comparative Analysis
Enbrel is one of several TNF inhibitors. Other important TNF inhibitors include infliximab, adalimumab, golimumab, and certolizumab pegol.
Compared with infliximab, Enbrel is a soluble TNF receptor-Fc fusion protein, while infliximab is a chimeric monoclonal antibody against TNF-alpha. Infliximab is given by intravenous infusion and is used in diseases such as rheumatoid arthritis, Crohn’s disease, ulcerative colitis, ankylosing spondylitis, psoriatic arthritis, and plaque psoriasis. Enbrel is not used for inflammatory bowel disease and may not be effective for Crohn’s disease or ulcerative colitis.
Compared with adalimumab, Enbrel differs structurally and mechanistically. Adalimumab is a fully human monoclonal antibody against TNF-alpha, while etanercept is a soluble p75 TNF receptor fusion protein that binds TNF-alpha and TNF-beta. Adalimumab has broader approved use in inflammatory bowel disease, while Enbrel is mainly used in arthritis, spondyloarthritis, and psoriasis indications.
Compared with certolizumab pegol, Enbrel has an Fc region, while certolizumab is a pegylated Fab fragment without an Fc region. Certolizumab’s structure influences placental transfer and pharmacological behavior, making it clinically distinct in pregnancy discussions.
Compared with methotrexate, Enbrel is a biologic targeted therapy, while methotrexate is a conventional synthetic DMARD. Methotrexate broadly affects immune cell function and folate-dependent pathways, while Enbrel specifically neutralizes TNF-mediated signaling. In rheumatoid arthritis, the two may be used together when appropriate.
Compared with IL-17 inhibitors such as secukinumab, Enbrel targets TNF rather than IL-17A. IL-17 inhibitors are especially effective in psoriasis and axial spondyloarthritis but may worsen inflammatory bowel disease. TNF inhibitors differ in their effectiveness across arthritis, psoriasis, and bowel disease, depending on the specific agent.
Compared with IL-23 inhibitors such as guselkumab, Enbrel acts earlier and more broadly in TNF-mediated inflammation, while IL-23 inhibitors target the IL-23/Th17 pathway. IL-23 inhibitors are very important in psoriasis and inflammatory bowel disease, but they do not work through TNF neutralization.
Compared with JAK inhibitors such as tofacitinib, upadacitinib, and baricitinib, Enbrel is an injectable biologic that neutralizes an extracellular cytokine. JAK inhibitors are oral small molecules that block intracellular cytokine signaling pathways and have different monitoring and safety concerns.
MCQs
- Enbrel contains which active drug?
a) Adalimumab
b) Etanercept
c) Infliximab
d) Secukinumab
Answer: b) Etanercept
- Enbrel belongs to which pharmacological class?
a) TNF inhibitor
b) IL-17A inhibitor
c) JAK inhibitor
d) CD20 antibody
Answer: a) TNF inhibitor
- Etanercept is structurally best described as:
a) Soluble p75 TNF receptor-Fc fusion protein
b) Small-molecule JAK inhibitor
c) Chimeric anti-TNF monoclonal antibody
d) Anti-CD20 monoclonal antibody
Answer: a) Soluble p75 TNF receptor-Fc fusion protein
- Enbrel mainly works by binding:
a) TNF-alpha and TNF-beta
b) IL-23 only
c) CD20 only
d) VEGF-A only
Answer: a) TNF-alpha and TNF-beta
- The main result of etanercept binding TNF is:
a) Prevention of TNF binding to cell-surface TNF receptors
b) Direct stimulation of TNF receptors
c) Irreversible inhibition of cyclooxygenase
d) Activation of dopamine receptors
Answer: a) Prevention of TNF binding to cell-surface TNF receptors
- Which intracellular pathway is commonly reduced after TNF blockade?
a) NF-kB-mediated inflammatory signaling
b) Insulin receptor signaling only
c) GABA receptor signaling
d) Cholinergic neuromuscular signaling
Answer: a) NF-kB-mediated inflammatory signaling
- Which disease is an approved use of Enbrel?
a) Rheumatoid arthritis
b) Acute bacterial pneumonia
c) Type 1 diabetes mellitus
d) Parkinson’s disease
Answer: a) Rheumatoid arthritis
- Enbrel is administered by which route?
a) Subcutaneous injection
b) Oral tablet
c) Inhalation
d) Intrathecal injection
Answer: a) Subcutaneous injection
- Which boxed warning is associated with Enbrel?
a) Serious infections and malignancies
b) Severe hypoglycemia only
c) Irreversible hearing loss
d) Acute opioid withdrawal
Answer: a) Serious infections and malignancies
- Which infection must be screened for before starting Enbrel?
a) Tuberculosis
b) Dermatophyte infection only
c) Common cold only
d) Helicobacter pylori only
Answer: a) Tuberculosis
- Which vaccine type should generally be avoided during Enbrel therapy?
a) Live vaccines
b) Inactivated influenza vaccine only
c) Recombinant vaccines only
d) Toxoid vaccines only
Answer: a) Live vaccines
- Which adverse reaction commonly occurs with Enbrel injections?
a) Injection-site reaction
b) Severe ototoxicity
c) Gingival hyperplasia
d) Hypoglycemic coma
Answer: a) Injection-site reaction
- Which neurologic condition may newly occur or worsen with TNF blockers such as Enbrel?
a) Demyelinating disease
b) Migraine aura only
c) Essential tremor only
d) Peripheral neuropathy from diabetes only
Answer: a) Demyelinating disease
- Enbrel is contraindicated in patients with:
a) Sepsis
b) Mild seasonal allergy
c) Controlled hypertension
d) Mild acne
Answer: a) Sepsis
- Which statement best differentiates Enbrel from infliximab?
a) Enbrel is a soluble TNF receptor-Fc fusion protein, while infliximab is an anti-TNF monoclonal antibody
b) Enbrel is oral, while infliximab is inhaled
c) Enbrel blocks CD20, while infliximab blocks IL-17A
d) Enbrel is an antibiotic, while infliximab is an antifungal
Answer: a) Enbrel is a soluble TNF receptor-Fc fusion protein, while infliximab is an anti-TNF monoclonal antibody
FAQs
What is the mechanism of action of Enbrel?
Enbrel, or etanercept, acts as a soluble decoy receptor for TNF. It binds TNF-alpha and TNF-beta, prevents them from binding cell-surface TNF receptors, and reduces TNF-mediated inflammatory signaling.
What is the generic name of Enbrel?
The generic name of Enbrel is etanercept.
Is Enbrel a monoclonal antibody?
Enbrel is not a conventional monoclonal antibody. It is a recombinant dimeric fusion protein made from the extracellular portion of the human p75 TNF receptor linked to the Fc portion of human IgG1.
What is Enbrel used for?
Enbrel is used for rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, plaque psoriasis, and juvenile psoriatic arthritis in approved adult or pediatric populations.
Why does Enbrel increase infection risk?
TNF is important for immune defense against infections, especially tuberculosis and certain fungal or opportunistic infections. Blocking TNF can reduce immune control of these pathogens and increase serious infection risk.
What is the most important warning for Enbrel?
The most important boxed warnings are serious infections and malignancies. Patients should be screened for tuberculosis before treatment and monitored for infections during therapy.
Can Enbrel be used with live vaccines?
Live vaccines should generally be avoided during Enbrel therapy because TNF blockade can reduce immune defense and increase infection risk from live vaccine organisms.
How is Enbrel different from adalimumab?
Enbrel is a soluble TNF receptor-Fc fusion protein that binds TNF-alpha and TNF-beta. Adalimumab is a fully human monoclonal antibody against TNF-alpha. Their indications, structure, dosing, and disease coverage differ.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

