
Table of Contents
Introduction
Vyvgart is the brand name of efgartigimod alfa-fcab, an immunomodulatory biologic drug used for generalized myasthenia gravis, commonly abbreviated as gMG. Pharmacologically, Vyvgart is a neonatal Fc receptor blocker, also called an FcRn blocker. A related subcutaneous product, Vyvgart Hytrulo, contains efgartigimod alfa with hyaluronidase-qvfc and is used in adults with generalized myasthenia gravis and chronic inflammatory demyelinating polyneuropathy, or CIDP.
Generalized myasthenia gravis is an autoimmune neuromuscular disorder in which pathogenic immunoglobulin G antibodies interfere with normal neuromuscular transmission. In many patients, these antibodies target the acetylcholine receptor at the neuromuscular junction. Some patients may have antibodies against muscle-specific tyrosine kinase, called MuSK, or other neuromuscular junction proteins. The final result is fluctuating skeletal muscle weakness, commonly affecting ocular, bulbar, limb, and respiratory muscles.
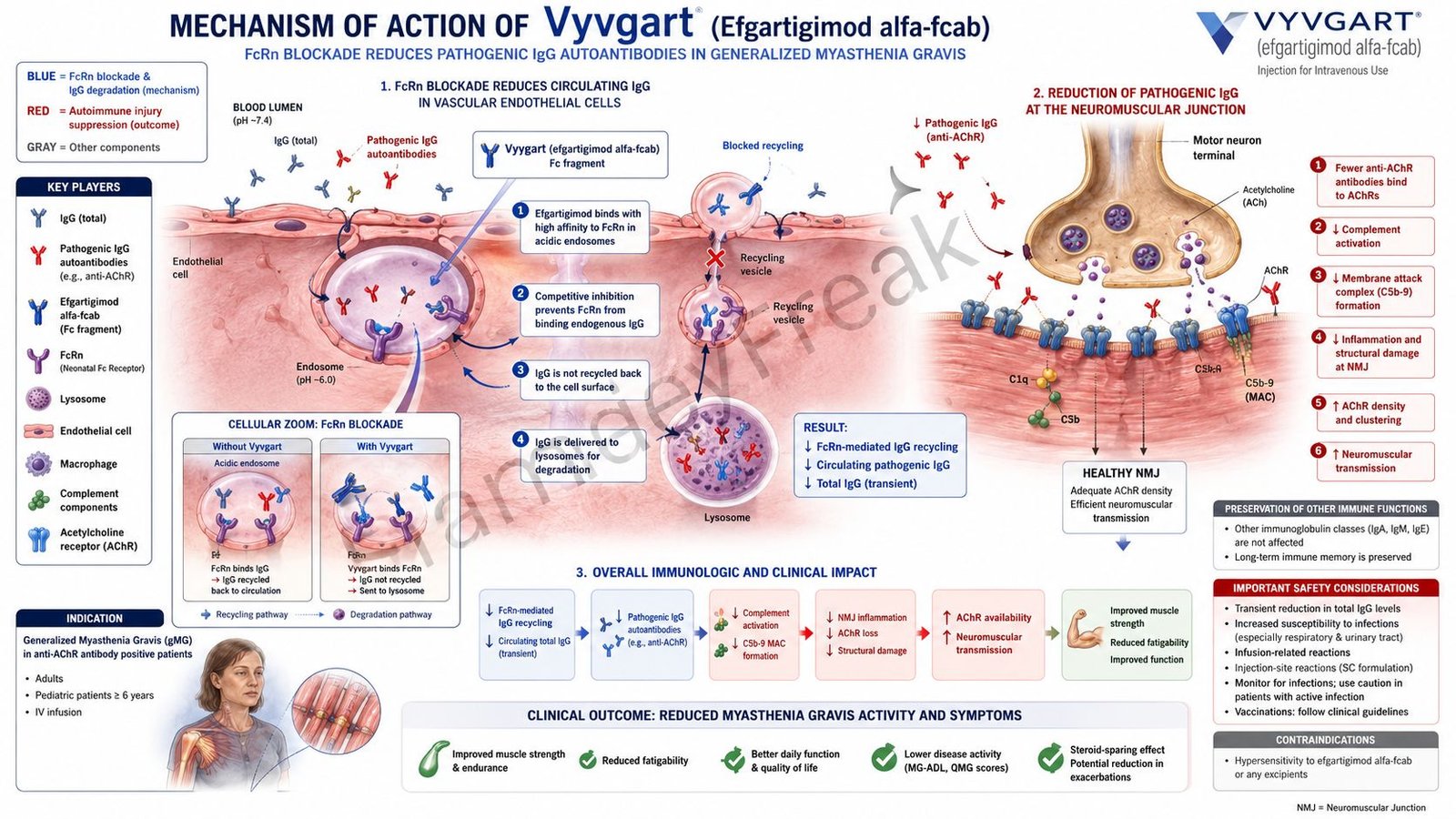
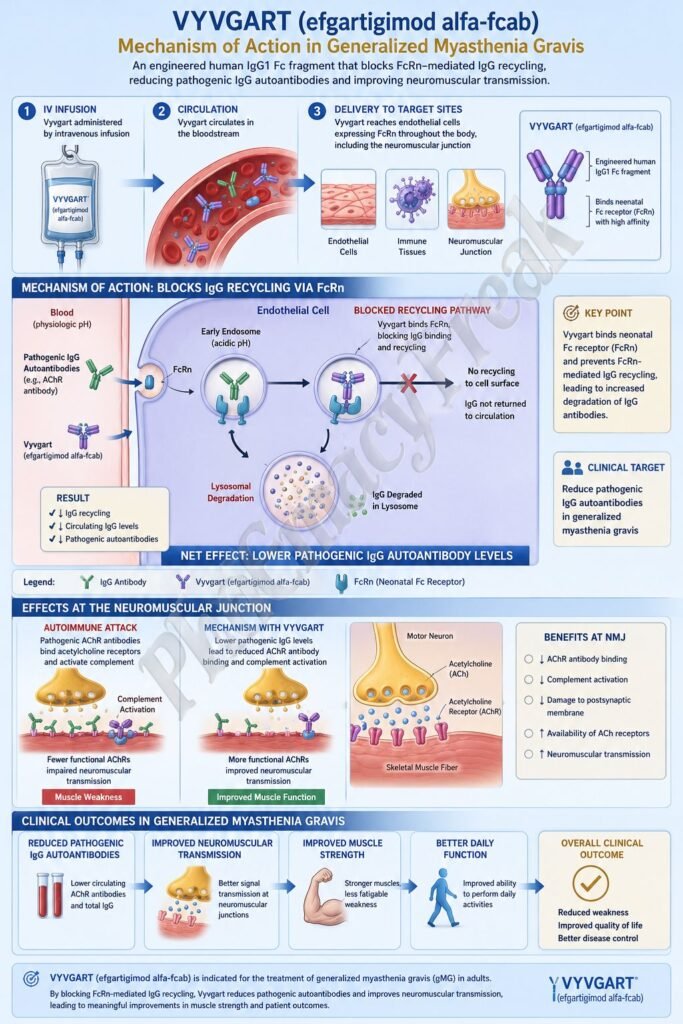
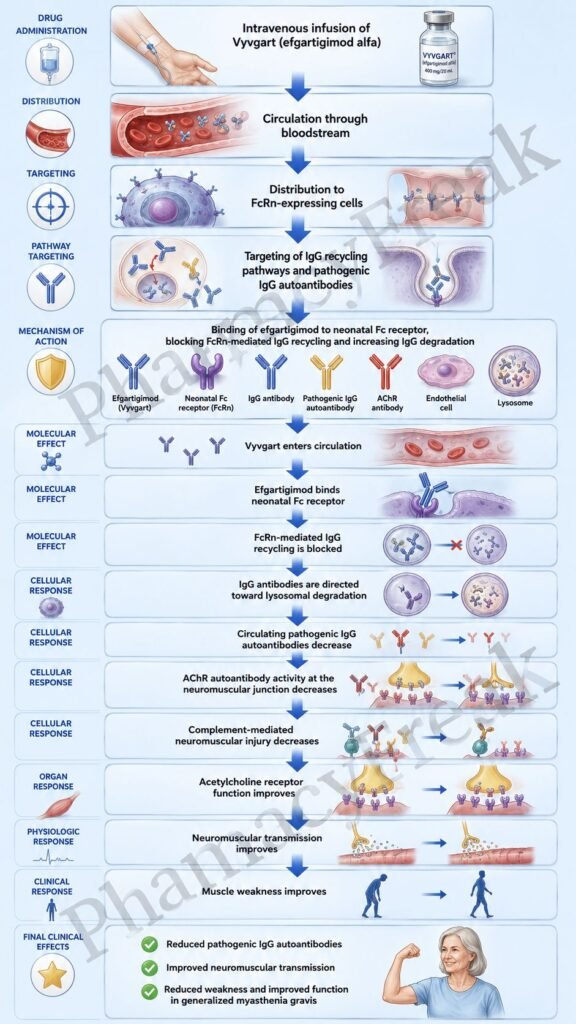
Vyvgart works by binding to the neonatal Fc receptor. FcRn normally protects IgG antibodies from lysosomal degradation and recycles them back into circulation. By blocking FcRn, efgartigimod increases IgG breakdown and lowers total circulating IgG levels, including pathogenic autoantibodies involved in autoimmune neuromuscular disease. The official label describes efgartigimod alfa-fcab as a human IgG1 antibody fragment that binds FcRn and reduces circulating IgG.
For exam purposes, Vyvgart should be remembered as an FcRn blocker that reduces pathogenic IgG autoantibody levels without broadly depleting B cells or directly blocking acetylcholinesterase. Its important adverse effects include infections, hypersensitivity reactions, infusion-related reactions with intravenous Vyvgart, and injection-site reactions with subcutaneous Vyvgart Hytrulo.
Mechanism of Action (Step-wise)
Step 1: Autoimmune IgG antibodies contribute to gMG
In generalized myasthenia gravis, pathogenic IgG autoantibodies interfere with neuromuscular transmission. Anti-acetylcholine receptor antibodies may block receptor function, promote receptor internalization, and activate complement-mediated injury at the postsynaptic membrane. Anti-MuSK antibodies can disrupt clustering and maintenance of acetylcholine receptors at the neuromuscular junction.
Step 2: Neuromuscular transmission becomes inefficient
Normally, acetylcholine released from the motor nerve terminal binds nicotinic acetylcholine receptors on skeletal muscle. This generates an end-plate potential and triggers muscle contraction. In gMG, autoantibody-mediated damage reduces the safety margin of neuromuscular transmission, leading to fatigable weakness.
Step 3: IgG antibodies are normally protected by FcRn
The neonatal Fc receptor is expressed in many cell types, including endothelial and hematopoietic cells. FcRn binds IgG inside acidic endosomes and rescues it from lysosomal degradation. The IgG is then recycled back to the cell surface and released into circulation.
Step 4: FcRn recycling prolongs IgG half-life
Because of FcRn-mediated recycling, IgG has a long half-life compared with many other plasma proteins. This is useful for normal immunity but problematic in IgG-mediated autoimmune diseases because pathogenic IgG autoantibodies can persist for a long time.
Step 5: Vyvgart binds to FcRn
Efgartigimod alfa-fcab is an engineered human IgG1 Fc fragment designed to bind FcRn. By binding FcRn, it competes with endogenous IgG antibodies for receptor interaction. This is the central molecular action of Vyvgart.
Step 6: IgG recycling is reduced
When FcRn is blocked, endogenous IgG antibodies are not efficiently rescued from intracellular degradation. Instead of being recycled back into blood, more IgG is directed toward lysosomal breakdown.
Step 7: Total circulating IgG levels decrease
As IgG recycling decreases, circulating IgG levels fall. Clinical pharmacodynamic studies show reduction in total IgG levels during treatment. In anti-AChR antibody-positive patients, anti-AChR autoantibody levels decrease in a similar pattern. In anti-AChR antibody-negative patients, total IgG falls, and in anti-MuSK-positive patients, anti-MuSK antibody levels decrease similarly to total IgG.
Step 8: Pathogenic autoantibody burden decreases
Lower pathogenic IgG autoantibody levels reduce autoimmune attack at the neuromuscular junction. This improves the functional availability of acetylcholine receptors or related neuromuscular junction structures.
Step 9: Neuromuscular transmission improves
When autoantibody-mediated interference decreases, acetylcholine signaling becomes more effective. Muscle fibers are more likely to reach threshold and contract properly after nerve stimulation.
Step 10: Muscle weakness improves
The final therapeutic effect in gMG is improvement in fatigable muscle weakness. Patients may experience improvement in activities such as speaking, chewing, swallowing, breathing, eye opening, arm movement, and walking, depending on disease severity and affected muscles.
Step 11: In CIDP, IgG-mediated nerve injury is reduced
CIDP is an immune-mediated peripheral neuropathy involving inflammation, demyelination, weakness, sensory symptoms, and impaired nerve conduction. In some patients, pathogenic IgG antibodies contribute to peripheral nerve injury. Vyvgart Hytrulo reduces circulating IgG and helps reduce immune-mediated nerve damage in adults with CIDP. Vyvgart Hytrulo is indicated for adult patients with CIDP.
Step 12: Vyvgart does not directly inhibit acetylcholinesterase
Vyvgart is different from pyridostigmine. Pyridostigmine improves neuromuscular transmission by inhibiting acetylcholinesterase and increasing acetylcholine availability. Vyvgart acts upstream on IgG recycling and reduces pathogenic autoantibody levels.
Step 13: Vyvgart does not broadly deplete B cells
Vyvgart is also different from anti-CD20 therapies such as rituximab. It does not primarily destroy B cells. Instead, it reduces circulating IgG antibodies by blocking FcRn-mediated recycling.
Step 14: Final therapeutic outcome
The final outcome is reduction of pathogenic IgG-mediated autoimmune activity. In gMG, this improves neuromuscular transmission and reduces muscle weakness. In CIDP, the related subcutaneous product helps reduce IgG-driven peripheral nerve inflammation and disability.
Pharmacokinetics
Vyvgart is administered by intravenous infusion. The recommended dosage of intravenous Vyvgart is 10 mg/kg once weekly for 4 weeks. In patients weighing 120 kg or more, the recommended dose is 1,200 mg per infusion. Subsequent treatment cycles are given based on clinical evaluation.
Vyvgart Hytrulo is administered subcutaneously and contains efgartigimod alfa with hyaluronidase-qvfc. Hyaluronidase increases permeability of subcutaneous tissue by depolymerizing hyaluronan, allowing a larger subcutaneous dose to disperse and absorb more easily. This tissue-permeability effect is transient and usually restored within 24 to 48 hours.
Efgartigimod alfa-fcab is a human IgG1-derived Fc fragment. It is a homodimer made of two identical peptide chains and has affinity for FcRn. Its molecular weight is approximately 54 kDa.
After intravenous administration, efgartigimod shows linear pharmacokinetics over studied dose ranges. Its volume of distribution is approximately 15 to 20 L, suggesting distribution mainly in vascular and extracellular fluid spaces.
Efgartigimod is expected to be degraded by proteolytic enzymes into small peptides and amino acids. It is not metabolized by cytochrome P450 enzymes, so classic CYP inhibitor or inducer interactions are unlikely. Less than 0.1% of a single intravenous dose was recovered in urine, indicating minimal unchanged renal excretion.
The terminal half-life of intravenous efgartigimod alfa-fcab is approximately 80 to 120 hours, or about 3 to 5 days. No dose adjustment is needed in mild renal impairment, but data are insufficient in moderate or severe renal impairment. Hepatic impairment is not expected to meaningfully affect pharmacokinetics because efgartigimod is not mainly cleared by hepatic CYP metabolism.
A clinically important drug interaction concept is that efgartigimod may decrease concentrations of other compounds that bind human FcRn. This may reduce exposure to some Fc-containing biologics or monoclonal antibodies, so medication review is important.
Clinical Uses
Vyvgart is indicated for the treatment of adult patients with generalized myasthenia gravis. The current U.S. label no longer limits the indication only to anti-acetylcholine receptor antibody-positive adults; the indication section states adult patients with gMG.
Vyvgart helps reduce autoimmune IgG-mediated impairment of neuromuscular transmission. It is especially useful in patients with clinically significant generalized symptoms such as limb weakness, bulbar symptoms, ocular weakness, respiratory involvement, or impaired daily function.
Vyvgart Hytrulo is indicated for adult patients with generalized myasthenia gravis and adult patients with chronic inflammatory demyelinating polyneuropathy.
In gMG, Vyvgart is not a rescue drug for immediate myasthenic crisis management. Severe respiratory or bulbar weakness may require urgent medical care, ventilatory support, plasma exchange, intravenous immunoglobulin, corticosteroids, or other specialist-directed therapies depending on severity.
In CIDP, Vyvgart Hytrulo is used to reduce immune-mediated peripheral nerve dysfunction. CIDP commonly presents with progressive or relapsing weakness, sensory loss, reduced reflexes, and demyelinating changes on nerve testing.
Vyvgart is not an acetylcholinesterase inhibitor, corticosteroid, broad immunosuppressant, or B-cell-depleting drug. It is a targeted FcRn blocker that reduces IgG antibody recycling.
Adverse Effects
The most important adverse effect category is infection. Because Vyvgart reduces circulating IgG levels, immune defense against infections may be affected. Treatment should be delayed in patients with active infection, and patients should be monitored for signs and symptoms of infection during therapy.
Common adverse reactions with intravenous Vyvgart in gMG include respiratory tract infections, headache, and urinary tract infection. Paresthesia and myalgia may also occur.
Hypersensitivity reactions can occur. Reported reactions include anaphylaxis, hypotension leading to syncope, angioedema, dyspnea, and rash. Vyvgart is contraindicated in patients with serious hypersensitivity to efgartigimod alfa products or any excipients.
Infusion-related reactions are important with intravenous Vyvgart. Symptoms may include headache, chills, nausea, vomiting, rash, blood pressure changes, dyspnea, or other infusion symptoms. Severe reactions may require discontinuation of the infusion and appropriate medical treatment.
Subcutaneous Vyvgart Hytrulo can cause injection-site reactions because it is administered under the skin. These may include redness, swelling, itching, pain, bruising, or local irritation. Systemic hypersensitivity reactions can also occur.
Vaccination planning is important. Because Vyvgart causes transient IgG reduction, live vaccines are not recommended during treatment. Age-appropriate vaccines should be reviewed before starting a new treatment cycle whenever possible.
Pregnancy and lactation require careful clinical judgment. There is limited human information about efgartigimod in pregnancy or human milk. Maternal IgG is known to be present in human milk, so breastfeeding decisions should consider maternal need and potential infant risk.
Vyvgart may reduce exposure to other FcRn-binding biologic products. This can be clinically important if a patient is taking monoclonal antibodies or Fc-fusion therapies for other conditions.
Comparative Analysis
Vyvgart is commonly compared with pyridostigmine, corticosteroids, azathioprine, mycophenolate mofetil, rituximab, eculizumab, ravulizumab, zilucoplan, intravenous immunoglobulin, and plasma exchange.
Compared with pyridostigmine, Vyvgart has a disease-modifying immunological mechanism. Pyridostigmine inhibits acetylcholinesterase and increases acetylcholine at the neuromuscular junction. Vyvgart reduces pathogenic IgG autoantibodies by blocking FcRn.
Compared with corticosteroids, Vyvgart is more targeted. Corticosteroids broadly suppress inflammation and immune activation, while Vyvgart specifically reduces IgG recycling. Steroids can be effective but are associated with weight gain, diabetes, osteoporosis, infection risk, cataracts, mood effects, and adrenal suppression.
Compared with azathioprine or mycophenolate mofetil, Vyvgart has a different onset and mechanism. Azathioprine and mycophenolate reduce lymphocyte proliferation and immune activity over time. Vyvgart reduces circulating IgG through FcRn blockade.
Compared with rituximab, Vyvgart does not directly deplete B cells. Rituximab targets CD20-positive B lymphocytes, reducing future antibody-producing immune activity. Vyvgart reduces existing circulating IgG by preventing FcRn recycling.
Compared with eculizumab and ravulizumab, Vyvgart acts upstream at the antibody level rather than at the complement level. Eculizumab and ravulizumab inhibit complement C5 and are especially relevant in anti-AChR antibody-positive gMG where complement-mediated postsynaptic injury is important.
Compared with zilucoplan, Vyvgart has a different target. Zilucoplan is a complement C5 inhibitor, while Vyvgart is an FcRn blocker. Both may improve gMG but act at different points in autoimmune pathology.
Compared with intravenous immunoglobulin, Vyvgart is more specific to FcRn blockade. IVIG has multiple immunomodulatory mechanisms, including Fc receptor modulation, complement effects, and autoantibody neutralization. Vyvgart directly blocks FcRn to increase IgG degradation.
Compared with plasma exchange, Vyvgart does not physically remove antibodies from plasma immediately. Plasma exchange rapidly removes circulating antibodies and is often used in severe exacerbations or crisis. Vyvgart gradually reduces IgG through altered recycling and catabolism.
MCQs
- Vyvgart contains which active drug?
a) Ravulizumab
b) Efgartigimod alfa-fcab
c) Rituximab
d) Pyridostigmine
Answer: b) Efgartigimod alfa-fcab
- Vyvgart belongs to which pharmacological class?
a) Acetylcholinesterase inhibitor
b) Complement C5 inhibitor
c) Neonatal Fc receptor blocker
d) CD20 monoclonal antibody
Answer: c) Neonatal Fc receptor blocker
- The main molecular target of Vyvgart is:
a) Neonatal Fc receptor
b) Acetylcholine receptor
c) Complement C5
d) Muscarinic M3 receptor
Answer: a) Neonatal Fc receptor
- FcRn normally functions to:
a) Destroy all IgG antibodies immediately
b) Recycle IgG and protect it from lysosomal degradation
c) Break down acetylcholine in the synaptic cleft
d) Activate complement C5 directly
Answer: b) Recycle IgG and protect it from lysosomal degradation
- Blocking FcRn with Vyvgart leads to:
a) Increased circulating IgG
b) Reduced circulating IgG
c) Increased acetylcholine release
d) Direct B-cell destruction
Answer: b) Reduced circulating IgG
- In generalized myasthenia gravis, Vyvgart reduces:
a) Pathogenic IgG autoantibodies
b) Serum glucose only
c) Dopamine levels
d) Platelet aggregation
Answer: a) Pathogenic IgG autoantibodies
- Which autoantibody is commonly involved in generalized myasthenia gravis?
a) Anti-acetylcholine receptor antibody
b) Anti-insulin antibody only
c) Anti-thyroglobulin antibody only
d) Anti-mitochondrial antibody only
Answer: a) Anti-acetylcholine receptor antibody
- Vyvgart is administered by which route?
a) Intravenous infusion
b) Oral tablet
c) Intranasal spray
d) Inhalation
Answer: a) Intravenous infusion
- Vyvgart Hytrulo contains efgartigimod alfa with:
a) Hyaluronidase
b) Dopamine
c) Insulin
d) Methotrexate
Answer: a) Hyaluronidase
- Hyaluronidase in Vyvgart Hytrulo mainly helps by:
a) Increasing permeability of subcutaneous tissue
b) Blocking acetylcholinesterase
c) Inhibiting complement C5
d) Stimulating dopamine receptors
Answer: a) Increasing permeability of subcutaneous tissue
- Which adverse effect category is important because Vyvgart reduces IgG?
a) Infection risk
b) Severe hypoglycemia
c) Irreversible hearing loss
d) Gingival hyperplasia
Answer: a) Infection risk
- Which vaccine type is not recommended during Vyvgart treatment?
a) Live vaccines
b) Inactivated influenza vaccine only
c) Recombinant vaccines only
d) Toxoid vaccines only
Answer: a) Live vaccines
- Which reaction can occur with intravenous Vyvgart administration?
a) Infusion-related reaction
b) Permanent tooth discoloration
c) Acute gout in every patient
d) Severe insulin overdose
Answer: a) Infusion-related reaction
- Vyvgart differs from pyridostigmine because Vyvgart:
a) Blocks FcRn and reduces IgG, while pyridostigmine inhibits acetylcholinesterase
b) Directly blocks acetylcholine receptors
c) Is an oral anticholinergic drug
d) Is a beta-blocker
Answer: a) Blocks FcRn and reduces IgG, while pyridostigmine inhibits acetylcholinesterase
- Which statement best describes Vyvgart?
a) It blocks FcRn, increases IgG degradation, and lowers pathogenic IgG autoantibodies
b) It directly stimulates nicotinic receptors at the neuromuscular junction
c) It permanently removes all B cells from the body
d) It inhibits bacterial cell wall synthesis
Answer: a) It blocks FcRn, increases IgG degradation, and lowers pathogenic IgG autoantibodies
FAQs
What is the mechanism of action of Vyvgart?
Vyvgart, or efgartigimod alfa-fcab, binds to the neonatal Fc receptor and blocks IgG recycling. This increases IgG degradation and reduces circulating pathogenic IgG autoantibodies involved in generalized myasthenia gravis.
What is the generic name of Vyvgart?
The generic name of Vyvgart is efgartigimod alfa-fcab.
What is Vyvgart used for?
Vyvgart is used for the treatment of adult patients with generalized myasthenia gravis. Vyvgart Hytrulo is used in adults with generalized myasthenia gravis and adults with chronic inflammatory demyelinating polyneuropathy.
Is Vyvgart an acetylcholinesterase inhibitor?
No. Vyvgart does not inhibit acetylcholinesterase. It reduces pathogenic IgG antibodies by blocking FcRn. Pyridostigmine is an acetylcholinesterase inhibitor used in myasthenia gravis.
Does Vyvgart deplete B cells?
No. Vyvgart does not primarily deplete B cells. It reduces circulating IgG levels by preventing FcRn-mediated IgG recycling.
Why does Vyvgart increase infection risk?
Vyvgart lowers circulating IgG levels. Since IgG antibodies help defend against infections, reducing IgG can increase susceptibility to infections in some patients.
Can live vaccines be given during Vyvgart therapy?
Live vaccines are not recommended during Vyvgart treatment because the drug causes transient reduction in IgG levels and vaccine safety or immune response may be affected.
How is Vyvgart different from Vyvgart Hytrulo?
Vyvgart is an intravenous efgartigimod alfa-fcab infusion. Vyvgart Hytrulo is a subcutaneous formulation containing efgartigimod alfa and hyaluronidase-qvfc. Hyaluronidase helps the drug disperse through subcutaneous tissue.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

