
Table of Contents
Introduction
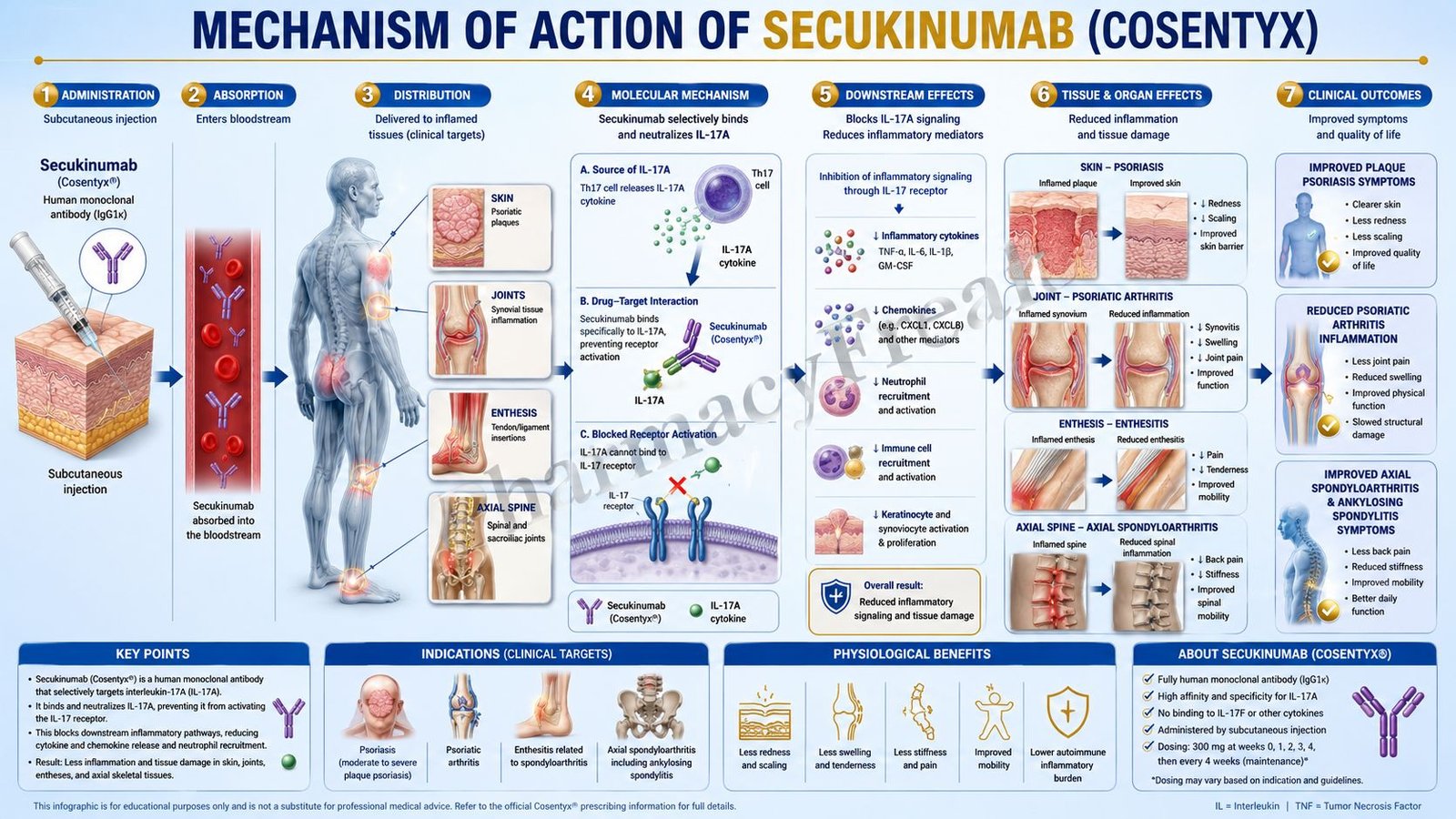
Secukinumab is a biologic immunomodulator marketed under the brand name Cosentyx. Pharmacologically, it is a human interleukin-17A antagonist and a recombinant human IgG1 kappa monoclonal antibody.
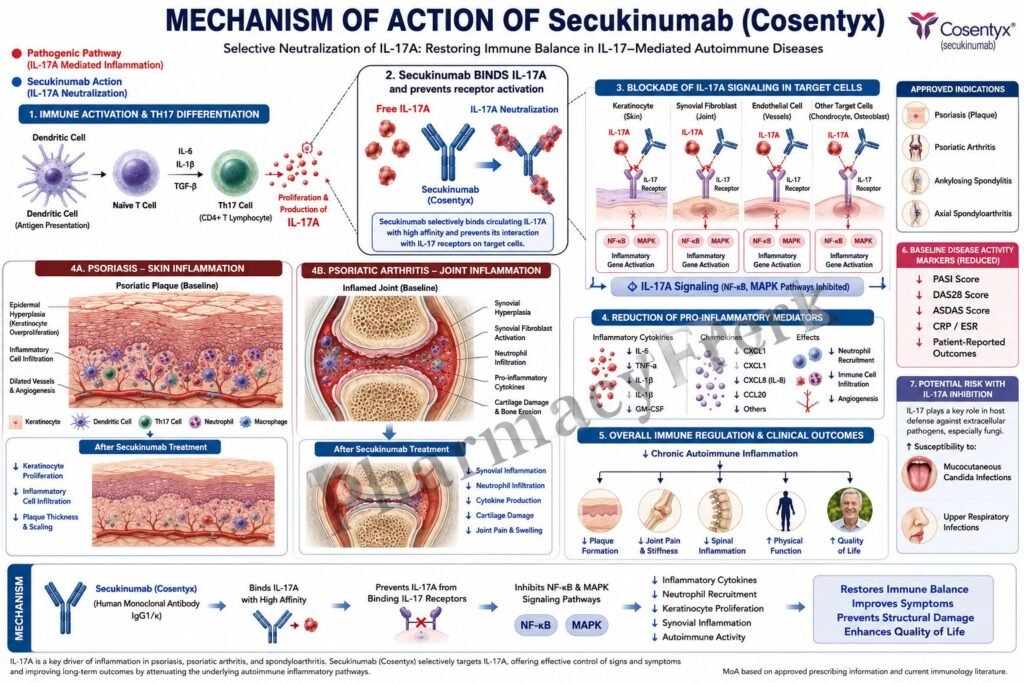
Interleukin-17A, commonly called IL-17A, is a pro-inflammatory cytokine involved in immune defense and chronic inflammatory disease. It is produced mainly by Th17 cells, but other immune cells such as gamma-delta T cells, innate lymphoid cells, neutrophils, and natural killer cells may also contribute to IL-17A production. IL-17A acts on keratinocytes, synoviocytes, endothelial cells, fibroblasts, and epithelial cells to promote inflammatory cytokines, chemokines, antimicrobial peptides, and neutrophil recruitment.
Secukinumab works by selectively binding to IL-17A and preventing it from interacting with the IL-17 receptor. This reduces downstream inflammatory signaling in skin, joints, entheses, axial skeleton, and hair follicle-associated inflammatory lesions.
Current approved uses of Cosentyx include moderate-to-severe plaque psoriasis in adults and pediatric patients 6 years and older; active psoriatic arthritis in adults and pediatric patients 2 years and older; active ankylosing spondylitis in adults and pediatric patients 12 years and older; active non-radiographic axial spondyloarthritis in adults with objective signs of inflammation; active enthesitis-related arthritis in pediatric patients 4 years and older; and moderate-to-severe hidradenitis suppurativa in adults and pediatric patients 12 years and older.
For exam purposes, secukinumab should be remembered as an anti-IL-17A monoclonal antibody that blocks IL-17A-mediated inflammation. It is especially important in psoriasis, psoriatic arthritis, axial spondyloarthritis, and hidradenitis suppurativa.
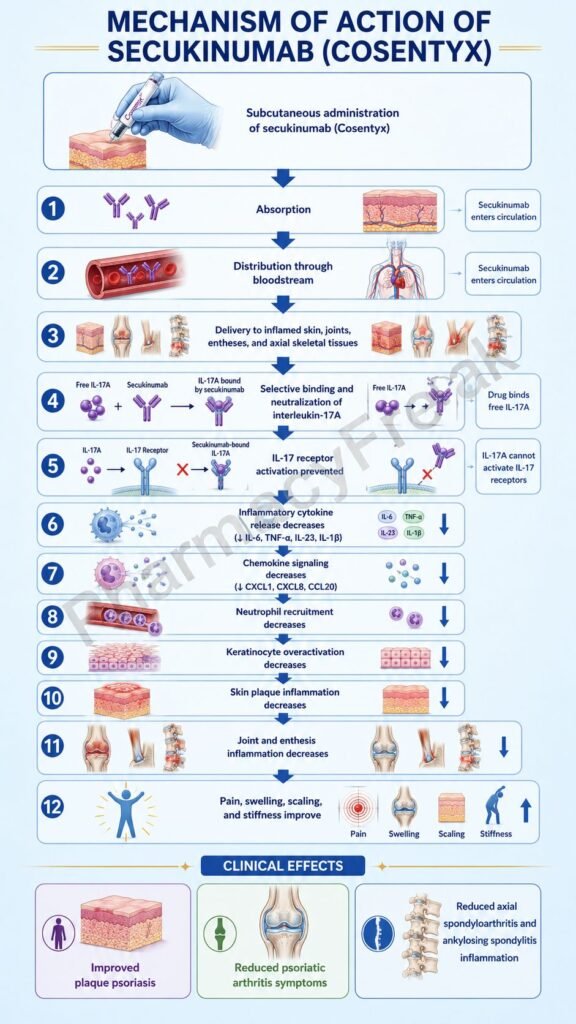
Mechanism of Action (Step-wise)
Step 1: IL-17A is produced by inflammatory immune cells
IL-17A is mainly associated with Th17 immune responses. It can also be produced by innate immune cells and other lymphocyte populations during inflammation. In chronic immune-mediated diseases, IL-17A becomes an important driver of tissue inflammation.
Step 2: IL-17A binds to IL-17 receptors on target cells
IL-17A normally binds to IL-17 receptor complexes on cells such as keratinocytes, synovial fibroblasts, epithelial cells, endothelial cells, and stromal cells. This receptor activation starts intracellular inflammatory signaling.
Step 3: IL-17 receptor signaling activates inflammatory pathways
After IL-17A binds its receptor, downstream signaling pathways such as NF-kB, MAPK, and C/EBP-related inflammatory transcription pathways become activated. These pathways increase production of pro-inflammatory mediators.
Step 4: Inflammatory cytokines and chemokines increase
IL-17A stimulation increases cytokines and chemokines such as IL-6, granulocyte colony-stimulating factor, CXCL1, CXCL8, CCL20, and other mediators. These signals recruit and activate neutrophils and other inflammatory cells.
Step 5: IL-17A drives keratinocyte activation in psoriasis
In plaque psoriasis, IL-17A stimulates keratinocytes to proliferate and produce inflammatory mediators. This contributes to thick, erythematous, scaly plaques. IL-17A also promotes antimicrobial peptide expression and maintains the inflammatory loop between immune cells and keratinocytes.
Step 6: IL-17A contributes to joint and enthesis inflammation
In psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondyloarthritis, and enthesitis-related arthritis, IL-17A contributes to synovitis, enthesitis, bone marrow inflammation, pain, stiffness, swelling, and tissue remodeling.
Step 7: IL-17A contributes to hidradenitis suppurativa inflammation
In hidradenitis suppurativa, inflammatory pathways involving IL-17A contribute to painful nodules, abscesses, draining tunnels, and chronic inflammatory lesions in intertriginous areas such as axillae, groin, buttocks, and inframammary regions.
Step 8: Secukinumab binds selectively to IL-17A
Secukinumab binds to IL-17A and neutralizes it. By binding IL-17A, secukinumab prevents IL-17A from interacting with the IL-17 receptor. This is the central molecular action of the drug.
Step 9: IL-17 receptor activation decreases
When IL-17A is neutralized, IL-17 receptor signaling is reduced. This lowers downstream activation of NF-kB, MAPK, and related inflammatory transcription pathways.
Step 10: Cytokine and chemokine production decreases
Reduced IL-17 receptor signaling decreases production of inflammatory cytokines, chemokines, and neutrophil-recruiting signals. This reduces inflammatory cell migration into skin, joints, entheses, and other affected tissues.
Step 11: Tissue inflammation improves
In plaque psoriasis, reduced IL-17A activity improves keratinocyte hyperproliferation and plaque inflammation. In psoriatic arthritis and axial spondyloarthritis, it reduces inflammatory pain, stiffness, swelling, and enthesitis. In hidradenitis suppurativa, it helps reduce inflammatory lesion activity.
Step 12: Secukinumab does not broadly block all IL-17 family cytokines
Secukinumab selectively targets IL-17A. It does not directly block TNF-alpha, IL-12, IL-23, JAK enzymes, or the IL-17 receptor itself. This selective cytokine targeting helps distinguish it from TNF inhibitors, IL-23 inhibitors, JAK inhibitors, and IL-17 receptor blockers.
Step 13: Final therapeutic outcome
The final therapeutic outcome is reduction of IL-17A-mediated inflammation. This improves skin lesions in plaque psoriasis, reduces musculoskeletal inflammation in psoriatic arthritis and spondyloarthritis, and helps control inflammatory lesion burden in hidradenitis suppurativa.
Pharmacokinetics
Secukinumab is administered by injection, not by oral tablet. Because it is a monoclonal antibody protein, it would be degraded in the gastrointestinal tract if taken orally.
Cosentyx is available for subcutaneous use through injection devices and prefilled syringes. It also has an intravenous formulation for some adult rheumatologic indications, including adult psoriatic arthritis, ankylosing spondylitis, and non-radiographic axial spondyloarthritis. The intravenous formulation must be diluted and administered by a healthcare professional as an infusion.
After subcutaneous administration, secukinumab is absorbed slowly. In plaque psoriasis subjects, peak serum concentrations after a single subcutaneous dose occurred at about 6 days. Bioavailability after subcutaneous administration ranged from approximately 55% to 77%.
Secukinumab distributes into serum and tissues. In plaque psoriasis, concentrations in lesional and non-lesional skin were measured at a fraction of serum concentrations, showing that the drug reaches skin tissue relevant to disease activity.
Secukinumab is not mainly metabolized by hepatic cytochrome P450 enzymes. Like endogenous IgG antibodies, it is expected to be degraded into small peptides and amino acids through catabolic pathways. Therefore, classic CYP-based drug interactions are not a major pharmacokinetic issue.
The mean half-life of secukinumab ranges from about 22 to 31 days in plaque psoriasis subjects, and population pharmacokinetic analysis estimated a mean half-life of about 23 days in hidradenitis suppurativa subjects. This long half-life supports dosing at extended intervals rather than daily use.
No formal trial has fully evaluated the effect of renal or hepatic impairment on secukinumab pharmacokinetics. Because it is a monoclonal antibody, renal filtration and CYP metabolism are not expected to be the main clearance mechanisms, but clinical judgment is still needed in patients with significant comorbidities.
Before treatment, patients should be evaluated for tuberculosis and should complete age-appropriate vaccinations according to current immunization guidance. Live vaccines should generally be avoided during therapy.
Clinical Uses
Secukinumab is used in moderate-to-severe plaque psoriasis in adults and pediatric patients 6 years and older who are candidates for systemic therapy or phototherapy. In psoriasis, blocking IL-17A reduces keratinocyte activation and inflammatory plaque formation.
Secukinumab is used in active psoriatic arthritis in adults and pediatric patients 2 years and older. It can improve joint pain, swelling, stiffness, enthesitis, dactylitis, and skin symptoms in appropriate patients.
It is also used in active ankylosing spondylitis in adults and pediatric patients 12 years and older. Ankylosing spondylitis is an inflammatory disease of the axial skeleton that commonly causes inflammatory back pain, morning stiffness, sacroiliitis, and reduced spinal mobility.
Secukinumab is used in active non-radiographic axial spondyloarthritis in adults with objective signs of inflammation. These patients have axial inflammatory symptoms but may not yet show definite radiographic sacroiliitis.
It is used in active enthesitis-related arthritis in pediatric patients 4 years and older. Enthesitis-related arthritis is a juvenile idiopathic arthritis category involving inflammation where tendons, ligaments, or joint capsules attach to bone.
Secukinumab is also used in moderate-to-severe hidradenitis suppurativa in adults and pediatric patients 12 years and older. This indication is important because IL-17A is involved in inflammatory lesions, nodules, abscesses, and draining tunnels in HS.
Secukinumab is not an antibiotic, steroid, NSAID, or immediate painkiller. It is a disease-modifying biologic therapy used for long-term control of selected immune-mediated inflammatory diseases.
Adverse Effects
The most important adverse effects of secukinumab are related to immune modulation. Because IL-17A participates in mucocutaneous immune defense, especially against fungal organisms, secukinumab can increase the risk of infections.
Common adverse effects include nasopharyngitis, upper respiratory tract infection, diarrhea, rhinitis, oral herpes, and injection-site reactions. Candida infections are exam-relevant because IL-17 signaling is important in defense against Candida species.
Serious infections can occur. Secukinumab should be used carefully in patients with chronic infection, recurrent infection, or risk factors for infection. If a serious infection develops, treatment interruption may be required until the infection is controlled.
Tuberculosis evaluation is required before starting therapy. Secukinumab should not be started in patients with active tuberculosis. Latent tuberculosis should be treated before beginning therapy according to standard recommendations.
Hypersensitivity reactions can occur, including anaphylaxis and urticaria. Secukinumab is contraindicated in patients with a serious hypersensitivity reaction to secukinumab or any excipient. Severe allergic reactions require discontinuation and urgent treatment.
Inflammatory bowel disease is an important warning. New-onset or worsening Crohn’s disease or ulcerative colitis has been reported with IL-17 inhibitors, including secukinumab. Patients with abdominal pain, chronic diarrhea, blood in stool, weight loss, or worsening intestinal symptoms require evaluation.
Eczematous eruptions have been reported, including atopic dermatitis-like eruptions and other eczematous skin reactions. Clinicians may need to evaluate severity and decide whether treatment should continue.
Live vaccines should generally be avoided during secukinumab therapy. Age-appropriate vaccines should be completed before starting treatment whenever possible.
Some device components may contain natural rubber latex, which is relevant for latex-sensitive individuals. Patients with latex sensitivity should review the specific product presentation and administration device with a healthcare professional.
Pregnancy and lactation data are limited. As an IgG antibody, secukinumab may cross the placenta, especially during the second and third trimesters. Use during pregnancy requires individualized risk-benefit assessment.
Comparative Analysis
Secukinumab is commonly compared with other biologic and targeted drugs used in psoriasis, psoriatic arthritis, axial spondyloarthritis, and hidradenitis suppurativa.
Compared with ixekizumab, secukinumab has a similar target because both are IL-17A inhibitors. Both reduce IL-17A-mediated inflammation, but they differ in dosing schedules, approved indications, formulation options, and clinical trial data.
Compared with brodalumab, secukinumab blocks IL-17A itself, while brodalumab blocks the IL-17 receptor A subunit. Brodalumab therefore inhibits signaling from multiple IL-17 family cytokines that use IL-17RA, whereas secukinumab selectively neutralizes IL-17A.
Compared with bimekizumab, secukinumab blocks IL-17A only, while bimekizumab blocks both IL-17A and IL-17F. This difference may influence efficacy and adverse effect patterns, including Candida infection risk.
Compared with IL-23 inhibitors such as guselkumab, risankizumab, and tildrakizumab, secukinumab acts downstream. IL-23 inhibitors reduce maintenance of Th17 responses, while secukinumab directly neutralizes the IL-17A effector cytokine.
Compared with ustekinumab, secukinumab has a different cytokine target. Ustekinumab blocks the p40 subunit shared by IL-12 and IL-23, while secukinumab blocks IL-17A.
Compared with TNF-alpha inhibitors such as adalimumab, infliximab, etanercept, and certolizumab, secukinumab targets a more specific cytokine pathway. TNF inhibitors are broadly useful across many inflammatory diseases, including inflammatory bowel disease, while IL-17 inhibitors may worsen or unmask inflammatory bowel disease in some patients.
Compared with JAK inhibitors such as tofacitinib and upadacitinib, secukinumab is an injectable biologic that neutralizes an extracellular cytokine. JAK inhibitors are oral small molecules that block intracellular signaling from multiple cytokines and require monitoring for infections, thrombosis, laboratory abnormalities, and lipid changes.
Compared with corticosteroids, secukinumab is not a broad rapid anti-inflammatory rescue drug. Corticosteroids suppress many inflammatory pathways quickly, while secukinumab selectively blocks IL-17A and is used for long-term disease control.
MCQs
- Secukinumab belongs to which pharmacological class?
a) IL-17A antagonist
b) TNF-alpha inhibitor
c) JAK inhibitor
d) IL-23 p19 inhibitor
Answer: a) IL-17A antagonist
- The brand name of secukinumab is:
a) Tremfya
b) Cosentyx
c) Humira
d) Stelara
Answer: b) Cosentyx
- Secukinumab is a:
a) Small-molecule oral kinase inhibitor
b) Human IgG1 kappa monoclonal antibody
c) Corticosteroid
d) Nonsteroidal anti-inflammatory drug
Answer: b) Human IgG1 kappa monoclonal antibody
- The main molecular target of secukinumab is:
a) IL-17A
b) IL-23 p19
c) TNF-alpha
d) JAK1
Answer: a) IL-17A
- IL-17A normally promotes inflammation by acting on:
a) Keratinocytes, synoviocytes, epithelial cells, and stromal cells
b) Red blood cells only
c) Pancreatic beta cells only
d) Platelets only
Answer: a) Keratinocytes, synoviocytes, epithelial cells, and stromal cells
- Secukinumab prevents IL-17A from:
a) Binding to the IL-17 receptor
b) Binding to dopamine receptors
c) Activating beta-2 receptors
d) Inhibiting acetylcholinesterase
Answer: a) Binding to the IL-17 receptor
- Which pathway is reduced after IL-17A blockade?
a) NF-kB and inflammatory chemokine signaling
b) Insulin receptor signaling only
c) Coagulation factor activation only
d) Cholinergic neuromuscular transmission
Answer: a) NF-kB and inflammatory chemokine signaling
- Which disease is an approved use of secukinumab?
a) Moderate-to-severe plaque psoriasis
b) Acute bacterial pneumonia
c) Type 1 diabetes mellitus
d) Parkinson’s disease
Answer: a) Moderate-to-severe plaque psoriasis
- Secukinumab is also used in:
a) Active psoriatic arthritis
b) Acute appendicitis
c) Tuberculosis treatment
d) Hyperthyroidism
Answer: a) Active psoriatic arthritis
- Which infection is especially exam-relevant with IL-17 blockade?
a) Candida infection
b) Malaria only
c) Rabies only
d) Tetanus only
Answer: a) Candida infection
- Which screening is recommended before starting secukinumab?
a) Tuberculosis evaluation
b) Audiometry only
c) Blood group testing only
d) Serum uric acid only
Answer: a) Tuberculosis evaluation
- Which vaccine type should generally be avoided during secukinumab therapy?
a) Live vaccines
b) Inactivated influenza vaccine only
c) Recombinant vaccines only
d) Toxoid vaccines only
Answer: a) Live vaccines
- Which condition may newly occur or worsen with secukinumab?
a) Inflammatory bowel disease
b) Hypothyroidism in all patients
c) Severe hypoglycemia
d) Acute glaucoma in every patient
Answer: a) Inflammatory bowel disease
- Secukinumab differs from guselkumab because guselkumab targets:
a) IL-23 p19
b) IL-17A
c) CD20
d) VEGF-A
Answer: a) IL-23 p19
- Which statement best describes secukinumab?
a) It neutralizes IL-17A and reduces inflammatory cytokine and chemokine signaling
b) It inhibits bacterial cell wall synthesis
c) It blocks dopamine D2 receptors
d) It inhibits cyclooxygenase irreversibly
Answer: a) It neutralizes IL-17A and reduces inflammatory cytokine and chemokine signaling
FAQs
What is the mechanism of action of secukinumab?
Secukinumab binds selectively to IL-17A and prevents IL-17A from activating the IL-17 receptor. This reduces downstream inflammatory cytokines, chemokines, neutrophil recruitment, keratinocyte activation, and tissue inflammation.
What is the brand name of secukinumab?
The brand name of secukinumab is Cosentyx.
What is secukinumab used for?
Secukinumab is used for plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondyloarthritis, enthesitis-related arthritis, and hidradenitis suppurativa in approved adult or pediatric populations.
Is secukinumab an IL-23 inhibitor?
No. Secukinumab is an IL-17A inhibitor. IL-23 inhibitors such as guselkumab, risankizumab, and tildrakizumab act upstream by suppressing IL-23-driven Th17 pathway maintenance.
Why can secukinumab increase Candida infections?
IL-17A is important for mucocutaneous defense against Candida. Blocking IL-17A can reduce this defense and increase the risk of oral, genital, or skin Candida infections.
Can secukinumab worsen inflammatory bowel disease?
Yes. New-onset or worsening Crohn’s disease or ulcerative colitis has been reported with IL-17 inhibitors. Patients with symptoms such as chronic diarrhea, abdominal pain, or blood in stool should be evaluated.
Is secukinumab taken orally?
No. Secukinumab is a monoclonal antibody and is given by injection. It is mainly administered subcutaneously, and an intravenous formulation is available for certain adult rheumatologic indications.
How is secukinumab different from adalimumab?
Secukinumab blocks IL-17A, while adalimumab blocks TNF-alpha. Both are biologics used in inflammatory diseases, but they target different cytokines and have different safety considerations.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

