
Table of Contents
Introduction
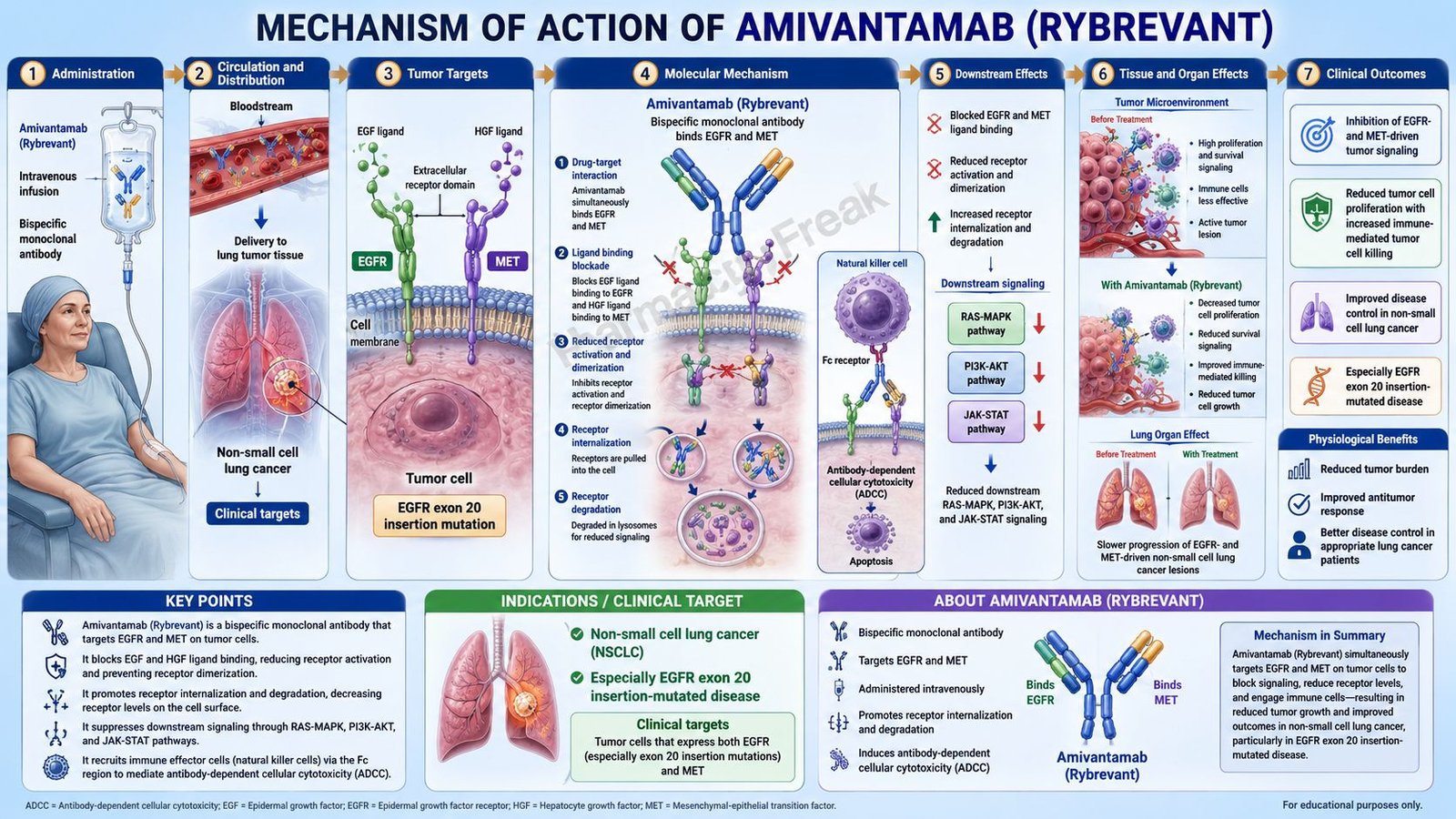
Amivantamab is a targeted anticancer monoclonal antibody used in selected patients with non-small cell lung cancer, commonly abbreviated as NSCLC. It is marketed under the brand name Rybrevant as intravenous amivantamab-vmjw. A subcutaneous formulation, Rybrevant Faspro, contains amivantamab with hyaluronidase-lpuj, but the key anticancer antibody component is amivantamab.
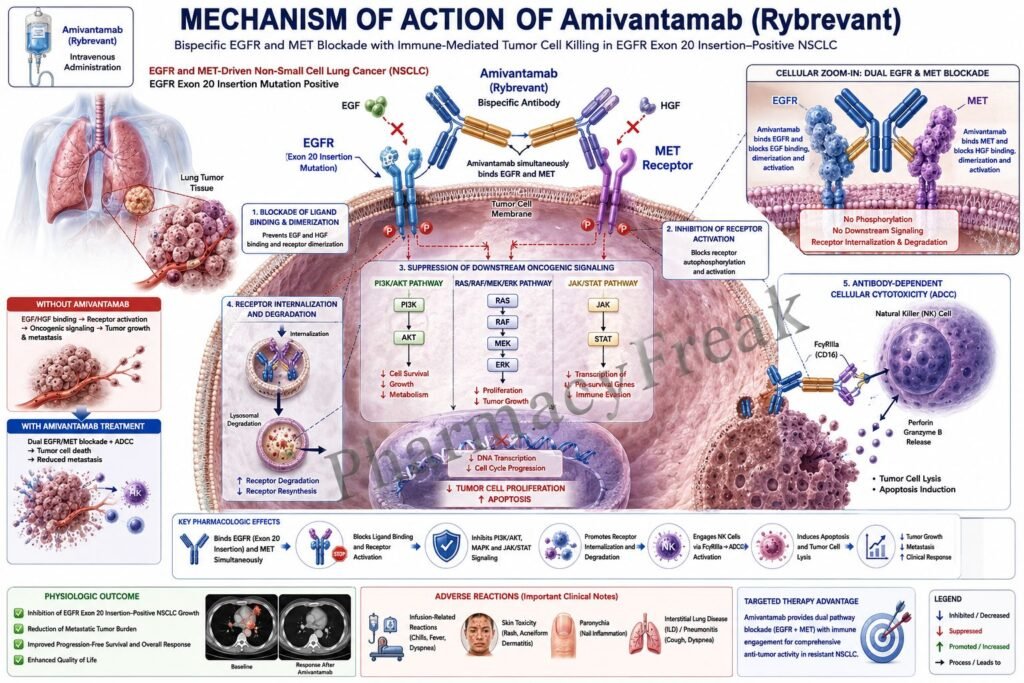
Pharmacologically, amivantamab is a bispecific antibody directed against two important receptor tyrosine kinases: epidermal growth factor receptor, or EGFR, and mesenchymal-epithelial transition factor receptor, or MET. These receptors are important drivers of tumor growth, survival, invasion, and treatment resistance in several types of lung cancer.
EGFR mutations are among the most important targetable alterations in NSCLC. Common activating EGFR mutations include exon 19 deletions and exon 21 L858R substitutions. Another clinically important group is EGFR exon 20 insertion mutations, which are often less responsive to older EGFR tyrosine kinase inhibitors. MET signaling may also contribute to tumor progression and resistance to EGFR-targeted therapy.
Amivantamab works by binding to the extracellular domains of EGFR and MET. This disrupts receptor signaling, promotes receptor degradation, and helps recruit immune effector cells to destroy tumor cells through antibody-dependent cellular cytotoxicity and trogocytosis. Current labeling includes use in adults with locally advanced or metastatic NSCLC with EGFR exon 19 deletions, exon 21 L858R substitution mutations, or EGFR exon 20 insertion mutations in specific first-line or previously treated settings, depending on combination regimen and prior therapy.
For exam purposes, amivantamab should be remembered as a bispecific EGFR-MET monoclonal antibody used in EGFR-mutated NSCLC, with important adverse effects such as infusion-related reactions, dermatologic toxicity, interstitial lung disease or pneumonitis, ocular toxicity, venous thromboembolism when combined with lazertinib, and embryo-fetal toxicity.
Mechanism of Action (Step-wise)
Step 1: EGFR and MET signaling promote tumor growth
EGFR and MET are receptor tyrosine kinases found on the surface of cells. In cancer cells, abnormal activation of these receptors can stimulate growth, survival, migration, invasion, angiogenesis, and resistance pathways.
Step 2: EGFR mutations activate oncogenic signaling
In NSCLC, EGFR mutations such as exon 19 deletions, exon 21 L858R substitutions, and exon 20 insertion mutations can cause abnormal receptor activation. This leads to continuous downstream signaling even when normal growth control signals are absent.
Step 3: EGFR activates downstream signaling pathways
Activated EGFR stimulates pathways such as RAS-RAF-MEK-ERK, PI3K-AKT-mTOR, and JAK-STAT. These pathways promote tumor-cell proliferation, survival, and resistance to apoptosis.
Step 4: MET signaling contributes to tumor progression and resistance
MET is activated by hepatocyte growth factor, also called HGF. MET activation can stimulate cell survival, epithelial-to-mesenchymal transition, invasion, and metastasis. MET pathway activation can also contribute to resistance against some EGFR-targeted therapies.
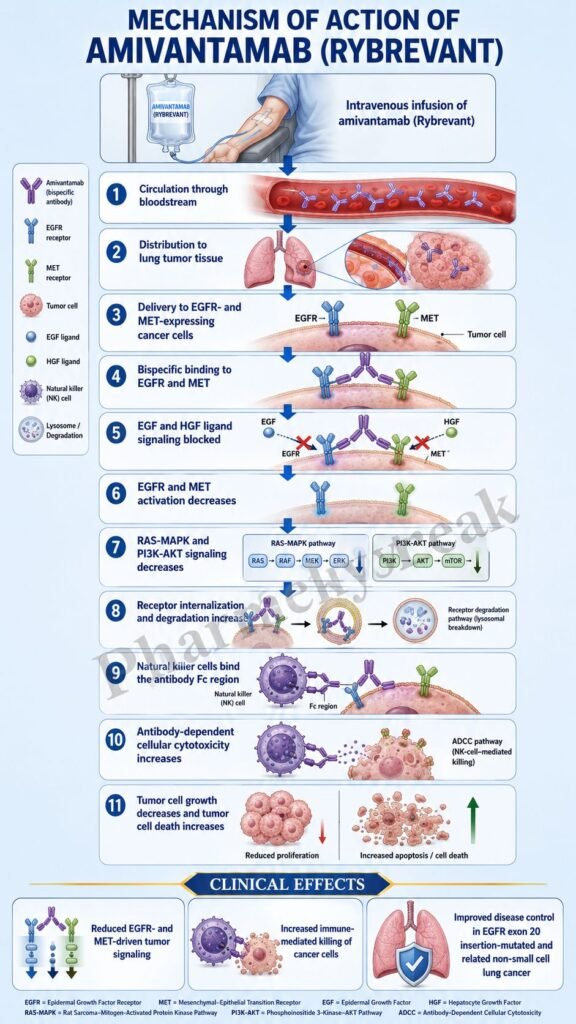
Step 5: Amivantamab binds extracellular EGFR and MET domains
Amivantamab is a bispecific antibody that binds to the extracellular domains of both EGFR and MET. This dual binding allows one antibody drug to target two tumor-driving receptors at the cell surface.
Step 6: Ligand binding and receptor activation are blocked
By occupying extracellular receptor regions, amivantamab can interfere with ligand-dependent receptor activation. This reduces activation of EGFR and MET signaling pathways that normally promote tumor growth and survival.
Step 7: EGFR and MET receptor degradation increases
Amivantamab can promote degradation of EGFR and MET. When receptor levels on the tumor-cell surface decrease, the cancer cell receives less growth and survival signaling through these pathways.
Step 8: Downstream proliferative signaling decreases
As EGFR and MET signaling are disrupted, downstream MAPK, PI3K-AKT, and related pathways become less active. This reduces tumor-cell proliferation and survival signaling.
Step 9: Tumor cells become marked for immune destruction
Because amivantamab is an IgG1-based antibody, its Fc region can interact with immune effector cells. When amivantamab binds EGFR and MET on tumor cells, it can help mark those cells for immune-mediated killing.
Step 10: Antibody-dependent cellular cytotoxicity occurs
Natural killer cells and other immune effector cells can recognize antibody-coated tumor cells and destroy them. This process is called antibody-dependent cellular cytotoxicity, or ADCC. It is one of the important immune mechanisms of amivantamab.
Step 11: Trogocytosis contributes to tumor-cell elimination
Macrophages may remove pieces of antibody-coated tumor-cell membrane through a process called trogocytosis. This can reduce receptor expression and contribute to tumor-cell damage or clearance. The official labeling describes immune effector-cell mechanisms including ADCC and trogocytosis.
Step 12: Combination with lazertinib strengthens EGFR pathway suppression
Lazertinib is an oral EGFR tyrosine kinase inhibitor. When amivantamab is combined with lazertinib, amivantamab targets extracellular EGFR and MET while lazertinib inhibits intracellular EGFR kinase signaling. This provides broader EGFR pathway blockade in appropriate EGFR-mutated NSCLC settings.
Step 13: Final therapeutic outcome
The final therapeutic outcome is inhibition of tumor growth, reduced oncogenic signaling, immune-mediated tumor-cell killing, and improved disease control in selected patients with EGFR-mutated locally advanced or metastatic NSCLC.
Pharmacokinetics
Amivantamab is administered by intravenous infusion when given as Rybrevant. It is not given as an oral tablet because monoclonal antibodies are large protein molecules that would be degraded in the gastrointestinal tract.
Rybrevant dosing is weight-based and depends on the indication and combination regimen. For some regimens, the initial dose is split over Week 1 Day 1 and Day 2 to reduce infusion-related reaction risk. Premedication with an antihistamine, antipyretic, and corticosteroid is used to reduce infusion-related reactions.
Rybrevant Faspro is a subcutaneous formulation of amivantamab with hyaluronidase-lpuj. Hyaluronidase helps increase dispersion and absorption of the injected antibody in subcutaneous tissue. The formulation, dose, route, and administration schedule differ from intravenous Rybrevant.
After intravenous administration, amivantamab exposure increases with dose. Steady-state concentrations are reached by about Week 13 for both 2-week and 3-week dosing regimens, and systemic accumulation is approximately 1.9-fold. The mean volume of distribution is approximately 5 L, reflecting distribution mainly within vascular and extracellular spaces.
Amivantamab has a mean linear clearance of about 0.26 L/day and a mean terminal half-life of approximately 14 days. This relatively long half-life supports intermittent dosing rather than daily administration.
Like other monoclonal antibodies, amivantamab is not mainly metabolized by cytochrome P450 enzymes. It is expected to be degraded into small peptides and amino acids through proteolytic catabolic pathways. Therefore, classic CYP-mediated pharmacokinetic interactions are not a major issue for amivantamab itself.
No clinically meaningful pharmacokinetic differences were observed based on age, body weight range within studied dosing categories, sex, race, ethnicity, mild or moderate renal impairment, or mild hepatic impairment. The effects of severe renal impairment, end-stage renal disease, and moderate to severe hepatic impairment have not been fully studied.
Clinical Uses
Amivantamab is used in adults with locally advanced or metastatic NSCLC with specific EGFR mutations confirmed by an FDA-approved test. Patient selection by mutation testing is essential because amivantamab is not a general lung cancer drug for all NSCLC patients.
Rybrevant in combination with lazertinib is indicated as first-line treatment for adult patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations.
Rybrevant in combination with carboplatin and pemetrexed is indicated for adults with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations whose disease has progressed on or after treatment with an EGFR tyrosine kinase inhibitor.
Rybrevant in combination with carboplatin and pemetrexed is also indicated for first-line treatment of adult patients with locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations.
Rybrevant as a single agent is indicated for adult patients with locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations whose disease has progressed on or after platinum-based chemotherapy.
Amivantamab is not used for small-cell lung cancer, non-EGFR-mutated NSCLC without a relevant indication, or cancers where EGFR/MET targeting is not clinically justified. It is also not a conventional chemotherapy drug; it is a targeted biologic therapy.
Adverse Effects
Infusion-related reactions are among the most important adverse effects of intravenous amivantamab. They commonly occur during the first infusion and may include fever, chills, flushing, nausea, chest discomfort, shortness of breath, wheezing, hypotension, vomiting, or allergic-type symptoms. Premedication and split first dosing are used to reduce this risk.
Dermatologic adverse reactions are very common because EGFR signaling is important in normal skin and hair follicle biology. Rash, acneiform dermatitis, dry skin, pruritus, paronychia, nail toxicity, and severe skin reactions can occur. Prophylactic skin care and early treatment are important. Severe rash, including toxic epidermal necrolysis, has been reported in labeling warnings.
Interstitial lung disease and pneumonitis are serious warnings. New or worsening cough, dyspnea, fever, or hypoxia should prompt evaluation. If ILD or pneumonitis is confirmed, treatment may need to be permanently discontinued depending on severity.
Venous thromboembolic events are especially important when amivantamab is used with lazertinib. Deep vein thrombosis and pulmonary embolism may occur. Current labeling recommends prophylactic anticoagulation for the first four months when Rybrevant is given with lazertinib, with monitoring and management based on severity.
Ocular toxicity may occur, including keratitis, dry eye symptoms, eye redness, blurred vision, or other eye complaints. Patients with worsening eye symptoms should be referred promptly to an ophthalmologist. Contact lens use may need to be interrupted until symptoms are evaluated.
Other common adverse effects include musculoskeletal pain, stomatitis, edema, fatigue, diarrhea, constipation, nausea, vomiting, decreased appetite, cough, dyspnea, paresthesia, hemorrhage, and laboratory abnormalities such as decreased albumin, decreased sodium, decreased potassium, decreased hemoglobin, increased ALT, increased AST, and decreased blood cell counts depending on regimen.
Embryo-fetal toxicity is an important warning. EGFR and MET signaling are important in embryonic development, and amivantamab can cause fetal harm based on its mechanism. Females of reproductive potential should use effective contraception during treatment and for 3 months after the last dose.
Breastfeeding is not recommended during treatment and for 3 months after the last dose because of the potential for serious adverse reactions in the breastfed child.
Comparative Analysis
Amivantamab is commonly compared with EGFR tyrosine kinase inhibitors such as osimertinib, lazertinib, erlotinib, gefitinib, afatinib, dacomitinib, and mobocertinib.
Compared with osimertinib, amivantamab is a monoclonal antibody that binds extracellular EGFR and MET, while osimertinib is an oral small-molecule EGFR tyrosine kinase inhibitor that blocks intracellular EGFR kinase activity. Osimertinib is widely used in EGFR exon 19 deletion and exon 21 L858R mutation NSCLC, while amivantamab has roles in combination regimens and EGFR exon 20 insertion disease.
Compared with lazertinib, amivantamab has a different route and target structure. Lazertinib is an oral EGFR TKI, while amivantamab is an antibody targeting EGFR and MET outside the cell. Their combination provides dual extracellular and intracellular pathway targeting.
Compared with older EGFR TKIs such as erlotinib and gefitinib, amivantamab is not limited to ATP-binding site inhibition. Its antibody-based mechanism includes receptor degradation and immune effector-cell recruitment.
Compared with MET inhibitors such as capmatinib and tepotinib, amivantamab targets both EGFR and MET. MET inhibitors mainly target MET exon 14 skipping or MET-driven disease, while amivantamab is used in EGFR-mutated NSCLC where dual EGFR-MET targeting is clinically useful.
Compared with platinum chemotherapy such as carboplatin plus pemetrexed, amivantamab is targeted therapy. Platinum chemotherapy causes DNA damage and broadly affects dividing cells. Amivantamab targets EGFR and MET receptor-driven cancer biology and may be combined with chemotherapy in approved NSCLC settings.
Compared with immune checkpoint inhibitors such as pembrolizumab or nivolumab, amivantamab does not primarily release T-cell immune checkpoints. Instead, it directly binds tumor-cell surface receptors and can recruit innate immune effector mechanisms such as ADCC and trogocytosis.
Compared with cetuximab, which targets EGFR alone, amivantamab is bispecific and targets both EGFR and MET. This dual targeting is a key pharmacological distinction.
MCQs
- Amivantamab belongs to which pharmacological class?
a) Bispecific EGFR-MET monoclonal antibody
b) PARP inhibitor
c) CDK4/6 inhibitor
d) Proteasome inhibitor
Answer: a) Bispecific EGFR-MET monoclonal antibody
- The main brand name of intravenous amivantamab is:
a) Rybrevant
b) Tagrisso
c) Tarceva
d) Keytruda
Answer: a) Rybrevant
- Amivantamab targets which receptors?
a) EGFR and MET
b) HER2 and VEGF only
c) CD20 and CD19
d) PD-1 and CTLA-4
Answer: a) EGFR and MET
- Amivantamab binds mainly to which part of EGFR and MET?
a) Extracellular domains
b) Nuclear DNA-binding domains
c) Mitochondrial membrane only
d) Ribosomal subunits
Answer: a) Extracellular domains
- Which cancer type is the main approved clinical area for amivantamab?
a) EGFR-mutated non-small cell lung cancer
b) Acute bacterial pneumonia
c) Chronic myeloid leukemia
d) Type 1 diabetes mellitus
Answer: a) EGFR-mutated non-small cell lung cancer
- Which EGFR mutation group is an important indication for single-agent amivantamab after platinum chemotherapy?
a) EGFR exon 20 insertion mutations
b) BRCA1 mutation
c) BCR-ABL T315I mutation
d) JAK2 V617F mutation
Answer: a) EGFR exon 20 insertion mutations
- Which mechanism contributes to amivantamab’s immune-mediated tumor-cell killing?
a) Antibody-dependent cellular cytotoxicity
b) Direct cyclooxygenase inhibition
c) Dopamine receptor blockade
d) Sodium channel opening
Answer: a) Antibody-dependent cellular cytotoxicity
- Trogocytosis with amivantamab mainly involves which immune cells?
a) Macrophages
b) Red blood cells
c) Platelets
d) Pancreatic beta cells
Answer: a) Macrophages
- Which downstream pathways are commonly activated by EGFR signaling?
a) RAS-RAF-MEK-ERK and PI3K-AKT pathways
b) Coagulation cascade only
c) Cholinergic neuromuscular pathway
d) Renin-angiotensin pathway only
Answer: a) RAS-RAF-MEK-ERK and PI3K-AKT pathways
- Which adverse effect is especially common during early intravenous amivantamab treatment?
a) Infusion-related reaction
b) Severe hypoglycemia
c) Ototoxicity in all patients
d) Gingival hyperplasia
Answer: a) Infusion-related reaction
- Which adverse effect is strongly related to EGFR inhibition?
a) Acneiform rash and nail toxicity
b) Severe insulin overdose
c) Irreversible hearing loss in every patient
d) Complete loss of smell in all patients
Answer: a) Acneiform rash and nail toxicity
- Which serious lung toxicity is associated with amivantamab?
a) Interstitial lung disease or pneumonitis
b) Acute asthma cure
c) Mandatory tuberculosis
d) Bronchial smooth muscle hypertrophy only
Answer: a) Interstitial lung disease or pneumonitis
- When amivantamab is combined with lazertinib, which adverse event requires special attention?
a) Venous thromboembolism
b) Severe hypoglycemia
c) Acute gout only
d) Vitamin C deficiency
Answer: a) Venous thromboembolism
- Amivantamab differs from osimertinib because amivantamab is:
a) An extracellular EGFR-MET antibody, while osimertinib is an intracellular EGFR TKI
b) A beta-blocker, while osimertinib is an antibiotic
c) A corticosteroid, while osimertinib is an NSAID
d) A dopamine agonist, while osimertinib is a diuretic
Answer: a) An extracellular EGFR-MET antibody, while osimertinib is an intracellular EGFR TKI
- Which statement best describes amivantamab?
a) It disrupts EGFR and MET signaling and recruits immune effector mechanisms against tumor cells
b) It inhibits bacterial cell wall synthesis
c) It blocks platelet P2Y12 receptors
d) It stimulates soluble guanylate cyclase
Answer: a) It disrupts EGFR and MET signaling and recruits immune effector mechanisms against tumor cells
FAQs
What is the mechanism of action of amivantamab?
Amivantamab is a bispecific monoclonal antibody that binds extracellular EGFR and MET receptors. It disrupts EGFR and MET signaling, promotes receptor degradation, and recruits immune effector cells to kill tumor cells through ADCC and trogocytosis.
What is the brand name of amivantamab?
The main brand name of intravenous amivantamab-vmjw is Rybrevant. Rybrevant Faspro is a subcutaneous formulation that contains amivantamab with hyaluronidase-lpuj.
What is amivantamab used for?
Amivantamab is used in selected adult patients with locally advanced or metastatic EGFR-mutated non-small cell lung cancer, including EGFR exon 19 deletions, exon 21 L858R substitutions, and EGFR exon 20 insertion mutations in specific treatment settings.
Is amivantamab a tyrosine kinase inhibitor?
No. Amivantamab is not a small-molecule tyrosine kinase inhibitor. It is a bispecific monoclonal antibody that binds extracellular EGFR and MET receptors. However, it may be combined with EGFR tyrosine kinase inhibitors such as lazertinib in approved settings.
Why does amivantamab target both EGFR and MET?
EGFR drives many EGFR-mutated lung cancers, while MET signaling can contribute to tumor progression and resistance. Dual EGFR-MET targeting helps block complementary tumor growth and survival pathways.
What are the most important adverse effects of amivantamab?
Important adverse effects include infusion-related reactions, rash, acneiform dermatitis, nail toxicity, paronychia, interstitial lung disease or pneumonitis, ocular toxicity, venous thromboembolism when combined with lazertinib, and embryo-fetal toxicity.
Why does amivantamab cause skin toxicity?
EGFR is important in normal skin and hair follicle biology. Blocking EGFR signaling can cause acneiform rash, dry skin, itching, paronychia, and nail changes.
Can amivantamab be used during pregnancy?
Amivantamab can cause fetal harm based on its mechanism involving EGFR and MET signaling. Females of reproductive potential should use effective contraception during treatment and for 3 months after the last dose.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

