
Table of Contents
Introduction
Cosentyx is the brand name of secukinumab, a fully human monoclonal antibody used in immune-mediated inflammatory diseases. It belongs to the class of interleukin-17A inhibitors, also called IL-17A antagonists.
Cosentyx is important in pharmacology because it targets a specific inflammatory cytokine rather than producing broad immunosuppression like corticosteroids. It is used in conditions where the IL-17 pathway plays a major role, such as plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondyloarthritis, enthesitis-related arthritis, and hidradenitis suppurativa. Current prescribing information lists Cosentyx as indicated for moderate to severe plaque psoriasis in adults and pediatric patients 6 years and older, active psoriatic arthritis in adults and pediatric patients 2 years and older, active ankylosing spondylitis in adults and pediatric patients 12 years and older, active non-radiographic axial spondyloarthritis in adults, active enthesitis-related arthritis in pediatric patients 4 years and older, and moderate to severe hidradenitis suppurativa in adults and pediatric patients 12 years and older.
For pharmacy, medical, nursing, and competitive exam students, Cosentyx is an important biologic drug because its mechanism is highly specific: it binds interleukin-17A and prevents IL-17A from interacting with the IL-17 receptor. This reduces downstream inflammation, keratinocyte activation, neutrophil recruitment, joint inflammation, and tissue damage.
Cosentyx is not a painkiller, steroid, antibiotic, or conventional disease-modifying antirheumatic drug. It is a targeted biologic immunomodulator used for long-term control of selected inflammatory disorders.
Mechanism of Action (Step-wise)
- Primary target: Interleukin-17A
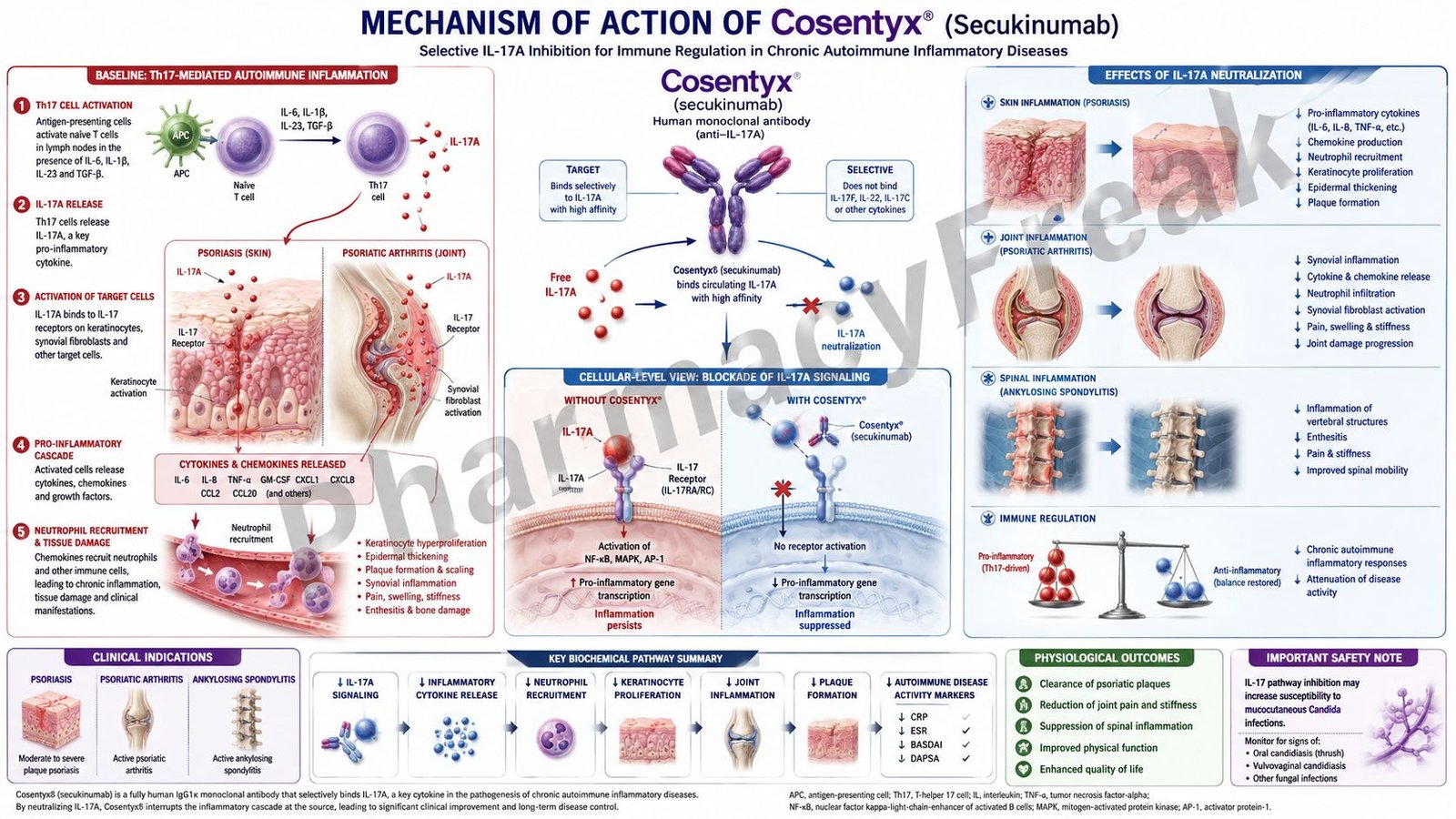
Cosentyx contains secukinumab, a human IgG1 monoclonal antibody that selectively binds to interleukin-17A. IL-17A is a naturally occurring cytokine involved in inflammatory and immune responses.
- Role of IL-17A in inflammation
IL-17A is mainly produced by Th17 cells and other immune cells such as innate lymphoid cells, gamma-delta T cells, and neutrophils. It plays an important role in chronic inflammatory diseases by stimulating keratinocytes, synovial cells, fibroblasts, endothelial cells, and other tissue cells.
- Blocking IL-17A interaction with IL-17 receptor
Normally, IL-17A binds to IL-17 receptors expressed on several cell types. This receptor activation triggers inflammatory signaling and increases the release of cytokines, chemokines, and other inflammatory mediators.
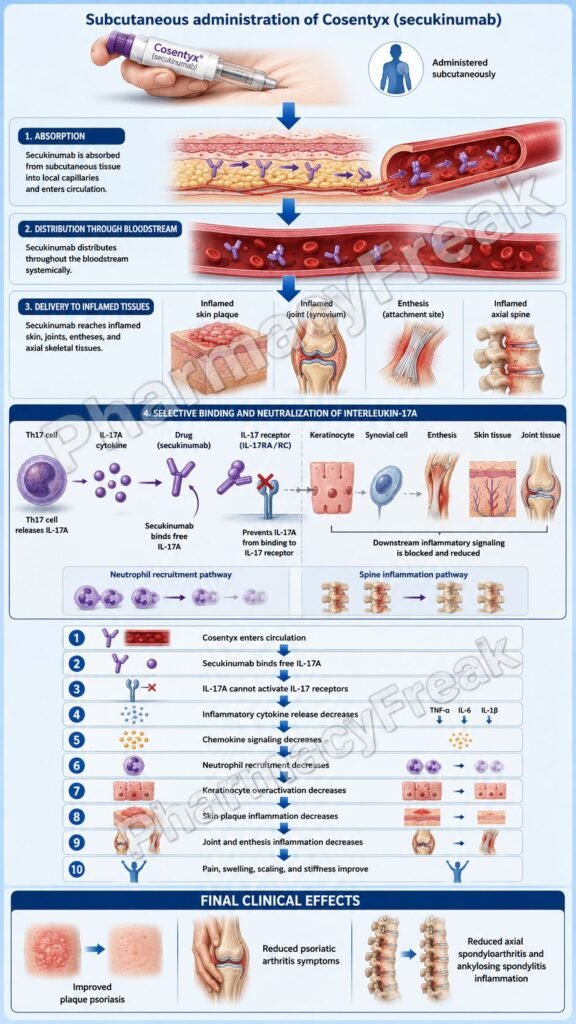
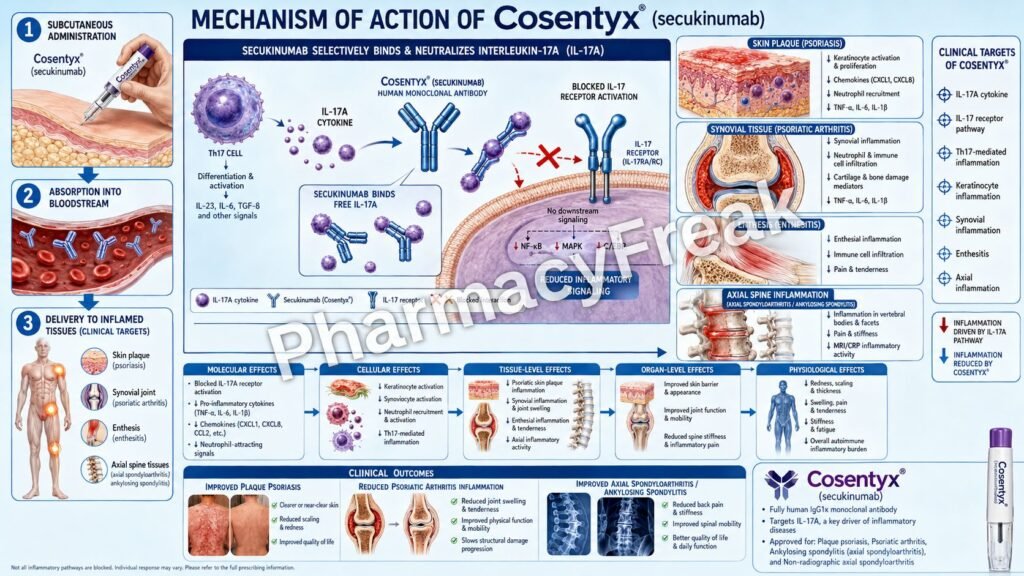
Secukinumab binds IL-17A and prevents it from interacting with the IL-17 receptor. This blocks IL-17A-mediated inflammatory signaling.
- Reduced proinflammatory cytokines and chemokines
By neutralizing IL-17A, Cosentyx decreases the release of proinflammatory cytokines and chemokines. These mediators normally attract inflammatory cells, amplify tissue inflammation, and maintain chronic immune activation.
- Effect in plaque psoriasis
In plaque psoriasis, IL-17A contributes to keratinocyte activation, epidermal hyperproliferation, neutrophil recruitment, scaling, erythema, and plaque formation. Cosentyx reduces IL-17A-mediated inflammation in psoriatic plaques and helps improve skin lesions.
- Effect in psoriatic arthritis and spondyloarthritis
In psoriatic arthritis, ankylosing spondylitis, and non-radiographic axial spondyloarthritis, IL-17A promotes synovial inflammation, enthesitis, bone-related inflammation, pain, stiffness, and joint damage. By inhibiting IL-17A, Cosentyx reduces inflammatory activity in joints, entheses, and axial skeleton.
- Effect in hidradenitis suppurativa
In hidradenitis suppurativa, IL-17A is involved in inflammatory lesions and immune activation in affected skin. Blocking IL-17A helps reduce inflammatory nodules, abscesses, and draining lesions in suitable patients.
- Final therapeutic effect
The final therapeutic effect of Cosentyx is reduced IL-17A-driven inflammation, improvement in psoriatic skin plaques, reduced joint inflammation, decreased pain and stiffness, improvement in axial inflammatory symptoms, and better control of hidradenitis suppurativa lesions.
Pharmacokinetics
Cosentyx is available mainly as a subcutaneous injection, and intravenous formulation may be used in selected adult rheumatologic indications under healthcare supervision.
Absorption:
After subcutaneous administration, secukinumab is absorbed slowly. Following a single subcutaneous dose in plaque psoriasis subjects, peak serum concentration occurs at approximately 6 days. The subcutaneous bioavailability of secukinumab ranges from about 55% to 77%.
Distribution:
Secukinumab distributes mainly in vascular and interstitial compartments, which is typical for monoclonal antibodies. The mean volume of distribution during the terminal phase after intravenous administration ranges from about 7.10 to 8.60 L in plaque psoriasis subjects.
Metabolism:
The exact metabolic pathway of secukinumab has not been fully characterized. Since it is a human IgG1 monoclonal antibody, it is expected to be degraded into small peptides and amino acids by normal catabolic pathways, similar to endogenous IgG.
Excretion:
Secukinumab is not primarily eliminated unchanged through the kidney like small-molecule drugs. It is mainly cleared through protein catabolism.
Half-life and duration:
The mean half-life of secukinumab ranges from approximately 22 to 31 days in plaque psoriasis subjects. This long half-life supports monthly maintenance dosing in many indications after the initial loading schedule.
Special pharmacokinetic point:
Steady-state concentrations are generally achieved by around Week 24 with every-4-week subcutaneous dosing. Body weight can influence secukinumab clearance and volume of distribution.
Clinical Uses
- Moderate to severe plaque psoriasis:
Cosentyx is used in adults and pediatric patients 6 years and older who are candidates for systemic therapy or phototherapy. - Psoriatic arthritis:
It is used in adults and pediatric patients 2 years and older with active psoriatic arthritis. It may be used with or without methotrexate. - Ankylosing spondylitis:
Cosentyx is used in adults and pediatric patients 12 years and older with active ankylosing spondylitis. - Non-radiographic axial spondyloarthritis:
It is used in adults with active non-radiographic axial spondyloarthritis with objective signs of inflammation. - Enthesitis-related arthritis:
It is used in pediatric patients 4 years and older with active enthesitis-related arthritis. - Hidradenitis suppurativa:
Cosentyx is used in adults and pediatric patients 12 years and older with moderate to severe hidradenitis suppurativa.
These indications reflect the role of IL-17A in inflammatory skin, joint, and axial skeletal diseases.
Adverse Effects
Common adverse effects of Cosentyx include:
- Nasopharyngitis
- Upper respiratory tract infection
- Rhinitis
- Diarrhea
- Headache
- Injection site reactions
- Nausea
- Fatigue
- Herpes infections
- Fungal infections, especially Candida infections
Important serious or clinically significant adverse effects include:
- Serious infections
- Tuberculosis reactivation risk
- Mucocutaneous candidiasis
- Inflammatory bowel disease worsening or new onset
- Hypersensitivity reactions
- Anaphylaxis
- Angioedema
- Eczematous eruptions
- Opportunistic infections
Cosentyx can increase the risk of infections because IL-17A contributes to host defense, especially at mucosal surfaces. Tuberculosis evaluation is recommended before starting therapy, and active TB should be treated before Cosentyx is initiated. Age-appropriate vaccinations should also be completed before treatment where possible.
Inflammatory bowel disease is an important exam point. IL-17 inhibitors may worsen Crohn’s disease or ulcerative colitis in some patients, so caution is needed in patients with a history of inflammatory bowel disease.
Live vaccines are generally avoided during therapy with biologic immunomodulators such as Cosentyx.
Comparative Analysis
| Feature | Cosentyx | Ixekizumab | Brodalumab | Adalimumab |
|---|---|---|---|---|
| Generic name | Secukinumab | Ixekizumab | Brodalumab | Adalimumab |
| Drug class | IL-17A inhibitor | IL-17A inhibitor | IL-17 receptor blocker | TNF-alpha inhibitor |
| Main target | IL-17A cytokine | IL-17A cytokine | IL-17 receptor A | TNF-alpha |
| Type of drug | Monoclonal antibody | Monoclonal antibody | Monoclonal antibody | Monoclonal antibody |
| Major use | Psoriasis, PsA, AS, nr-axSpA, HS | Psoriasis, PsA, axial spondyloarthritis | Plaque psoriasis | Psoriasis, PsA, RA, IBD, AS |
| Key pathway | IL-17 pathway | IL-17 pathway | IL-17 receptor pathway | TNF-alpha pathway |
| Infection risk | Yes | Yes | Yes | Yes |
| IBD caution | Important | Important | Important | Can treat some IBD cases |
| Route | Subcutaneous; IV in selected adult indications | Subcutaneous | Subcutaneous | Subcutaneous |
Cosentyx and ixekizumab both directly target IL-17A, while brodalumab blocks the IL-17 receptor. Adalimumab is different because it targets TNF-alpha rather than IL-17A. A clinically important distinction is inflammatory bowel disease: TNF-alpha inhibitors may be useful in some IBD patients, whereas IL-17 pathway inhibitors may worsen or trigger IBD in susceptible patients.
MCQs
- Cosentyx contains which active drug?
a) Adalimumab
b) Secukinumab
c) Ustekinumab
d) Infliximab
Answer: b) Secukinumab
- Cosentyx primarily targets which cytokine?
a) IL-6
b) TNF-alpha
c) IL-17A
d) IL-1 beta
Answer: c) IL-17A
- Secukinumab belongs to which drug class?
a) Calcineurin inhibitor
b) IL-17A inhibitor
c) Antimetabolite
d) JAK inhibitor
Answer: b) IL-17A inhibitor
- Cosentyx prevents IL-17A from binding to:
a) Dopamine receptor
b) IL-17 receptor
c) Beta-2 receptor
d) Insulin receptor
Answer: b) IL-17 receptor
- Which disease is commonly treated with Cosentyx?
a) Plaque psoriasis
b) Acute bacterial pneumonia
c) Type 1 diabetes ketoacidosis
d) Malaria
Answer: a) Plaque psoriasis
- The main pharmacological effect of Cosentyx is:
a) Increased gastric acid secretion
b) Reduced IL-17A-mediated inflammation
c) Direct bacterial killing
d) Increased insulin release
Answer: b) Reduced IL-17A-mediated inflammation
- Which adverse effect is associated with IL-17A inhibition?
a) Mucocutaneous Candida infection
b) Severe hypoglycemia
c) Ototoxicity
d) Hyperkalemia
Answer: a) Mucocutaneous Candida infection
- Which condition requires caution during Cosentyx therapy?
a) Inflammatory bowel disease
b) Mild myopia
c) Iron deficiency anemia only
d) Lactose intolerance
Answer: a) Inflammatory bowel disease
- Cosentyx is best described as a:
a) Steroid
b) Monoclonal antibody
c) NSAID
d) Antibiotic
Answer: b) Monoclonal antibody
- Which statement about IL-17A is correct?
a) It has no role in inflammation
b) It promotes inflammatory cytokine and chemokine release
c) It is a pancreatic hormone
d) It directly lowers blood glucose
Answer: b) It promotes inflammatory cytokine and chemokine release
- Before starting Cosentyx, patients should be evaluated for:
a) Active or latent tuberculosis
b) Blood group only
c) Vitamin C level only
d) Serum amylase only
Answer: a) Active or latent tuberculosis
- Cosentyx differs from adalimumab because adalimumab targets:
a) IL-17A
b) TNF-alpha
c) IL-17 receptor
d) Histamine H1 receptor
Answer: b) TNF-alpha
- Which route is commonly used for Cosentyx administration?
a) Oral
b) Subcutaneous
c) Inhalational
d) Sublingual
Answer: b) Subcutaneous
- The long dosing interval of Cosentyx is mainly due to:
a) Rapid renal excretion
b) Long monoclonal antibody half-life
c) Immediate metabolism by CYP enzymes
d) Poor receptor binding
Answer: b) Long monoclonal antibody half-life
- Which statement about Cosentyx is correct?
a) It blocks IL-17A and reduces inflammatory signaling
b) It is used for acute asthma relief
c) It directly inhibits bacterial cell wall synthesis
d) It is a dopamine receptor antagonist
Answer: a) It blocks IL-17A and reduces inflammatory signaling
FAQs
- What is Cosentyx used for?
Cosentyx is used for several immune-mediated inflammatory diseases, including moderate to severe plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondyloarthritis, enthesitis-related arthritis, and hidradenitis suppurativa.
- What is the mechanism of action of Cosentyx?
Cosentyx contains secukinumab, a monoclonal antibody that selectively binds IL-17A. By blocking IL-17A interaction with the IL-17 receptor, it reduces inflammatory cytokines, chemokines, immune cell recruitment, and tissue inflammation.
- Is Cosentyx a steroid?
No. Cosentyx is not a steroid. It is a biologic monoclonal antibody that specifically targets IL-17A.
- Why is IL-17A important in psoriasis?
IL-17A activates keratinocytes and promotes inflammatory mediator release. This contributes to epidermal hyperproliferation, scaling, erythema, plaque formation, and neutrophil recruitment in psoriasis.
- Can Cosentyx increase infection risk?
Yes. Cosentyx can increase the risk of infections, including upper respiratory infections and fungal infections such as Candida. Serious infections may also occur.
- Why is tuberculosis screening done before Cosentyx?
Because Cosentyx affects immune function, patients should be evaluated for active or latent tuberculosis before treatment. Active TB should be treated before starting therapy.
- Can Cosentyx worsen inflammatory bowel disease?
Yes. IL-17 pathway inhibition may worsen or trigger inflammatory bowel disease in some patients. Caution is needed in patients with Crohn’s disease or ulcerative colitis.
- How is Cosentyx administered?
Cosentyx is commonly administered by subcutaneous injection. Intravenous administration may be used in selected adult indications under healthcare supervision.
- How is Cosentyx different from TNF inhibitors?
Cosentyx targets IL-17A, while TNF inhibitors such as adalimumab target TNF-alpha. Both reduce inflammation, but they act on different cytokine pathways.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

