
Table of Contents
Introduction
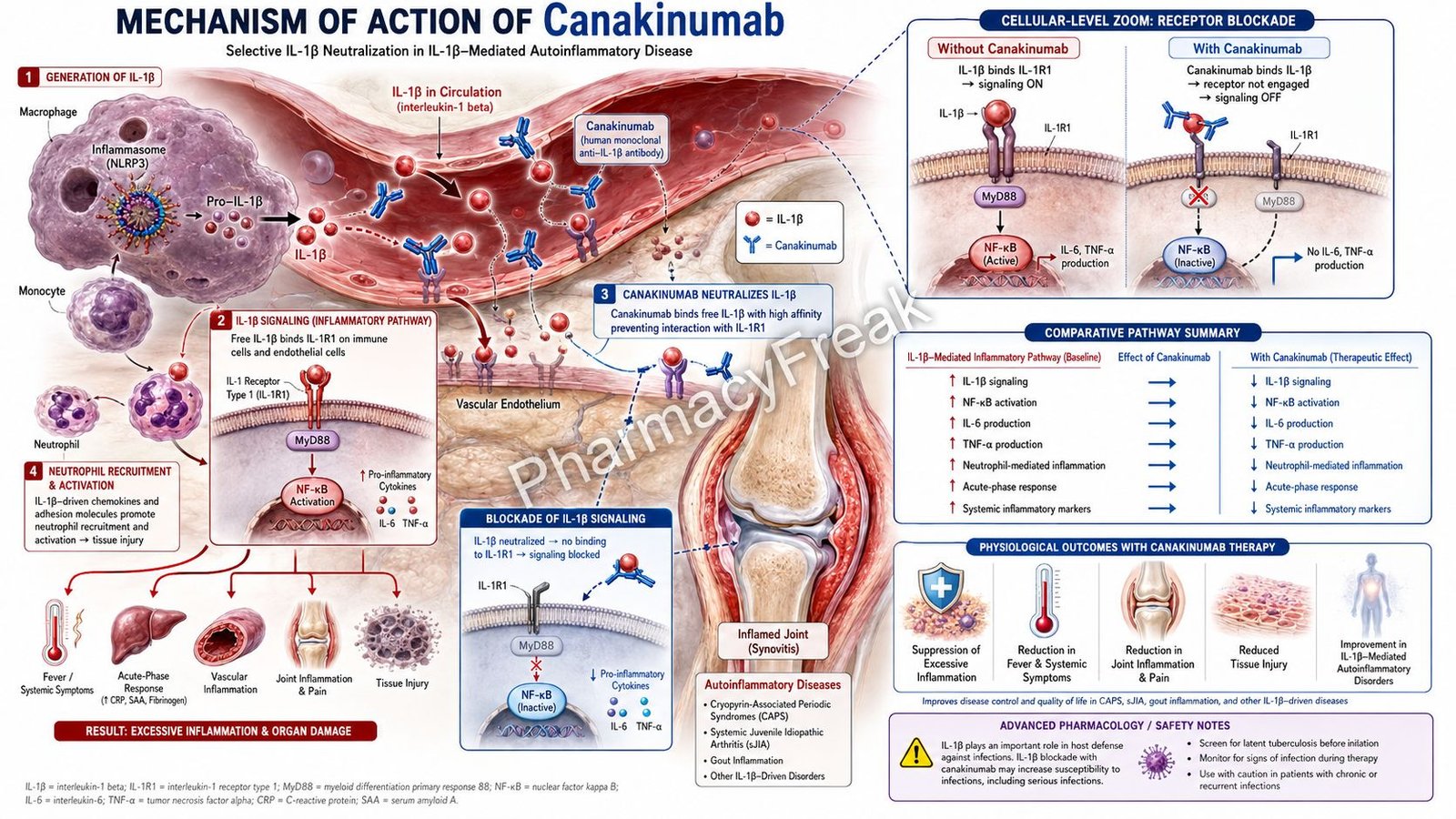
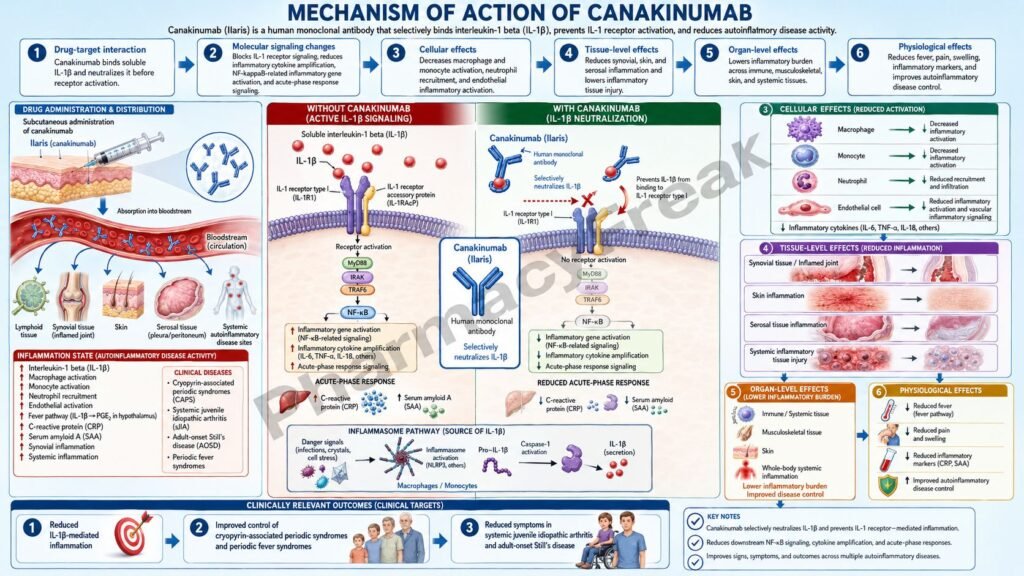
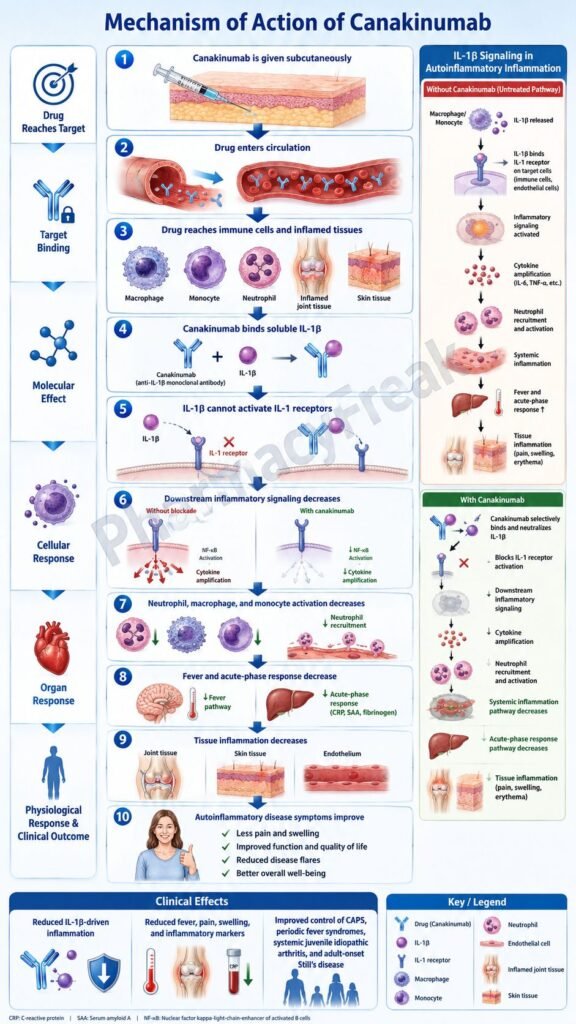
Canakinumab is a recombinant human monoclonal antibody used as a targeted anti-inflammatory biologic. It is marketed under the brand name Ilaris and belongs to the class of interleukin-1 beta inhibitors. Canakinumab specifically blocks interleukin-1 beta, also written as IL-1β, a powerful pro-inflammatory cytokine involved in fever, neutrophil recruitment, acute-phase response, joint inflammation, systemic inflammation, and autoinflammatory disease activity.
Canakinumab is clinically important because many autoinflammatory diseases are driven by excessive IL-1β activity. Unlike corticosteroids or broad immunosuppressants, canakinumab targets a specific cytokine pathway. It binds IL-1β and prevents it from activating IL-1 receptors on immune and tissue cells. The official labeling describes canakinumab as a human monoclonal anti-human IL-1β antibody that neutralizes IL-1β by blocking its interaction with IL-1 receptors; it does not bind IL-1α or IL-1 receptor antagonist.
Canakinumab is indicated for several IL-1β-driven diseases, including cryopyrin-associated periodic syndromes, tumor necrosis factor receptor-associated periodic syndrome, hyperimmunoglobulin D syndrome/mevalonate kinase deficiency, familial Mediterranean fever, active Still’s disease including adult-onset Still’s disease and systemic juvenile idiopathic arthritis, and selected adult gout flares when NSAIDs and colchicine are unsuitable or inadequate and repeated corticosteroid courses are not appropriate.
For pharmacy, medical, nursing, and competitive exam students, canakinumab is important because it connects immunology, inflammation, rheumatology, rare autoinflammatory syndromes, and biologic pharmacology. Its key mechanism is selective neutralization of IL-1β, leading to reduced inflammasome-driven inflammation and decreased acute-phase markers such as C-reactive protein and serum amyloid A.
Mechanism of Action (Step-wise)
- Primary target: Interleukin-1 beta
Canakinumab specifically targets interleukin-1 beta. IL-1β is a pro-inflammatory cytokine produced mainly by activated macrophages, monocytes, and other innate immune cells. It is generated after activation of inflammatory pathways such as the inflammasome, especially the NLRP3 inflammasome.
IL-1β promotes fever, leukocyte activation, endothelial activation, pain, tissue inflammation, and production of acute-phase proteins.
- Binding to soluble IL-1β
After subcutaneous administration and systemic absorption, canakinumab circulates in the blood and binds human IL-1β with high specificity. This prevents free IL-1β from interacting with its receptor on target cells.
This is the central pharmacological action of canakinumab: selective neutralization of IL-1β.
- Prevention of IL-1 receptor activation
Normally, IL-1β binds to interleukin-1 receptor type I on immune cells, endothelial cells, synovial cells, skin cells, and other tissues. This receptor then recruits the IL-1 receptor accessory protein, allowing intracellular inflammatory signaling to proceed.
Canakinumab blocks this first step by binding IL-1β before it can activate the IL-1 receptor complex.
- Inhibition of downstream inflammatory signaling
When IL-1β activates its receptor, downstream signaling pathways such as MyD88-dependent signaling, IRAK activation, TRAF6 activation, NF-κB activation, and MAP kinase signaling are stimulated.
These pathways increase transcription of inflammatory genes. By neutralizing IL-1β, canakinumab reduces activation of these downstream pathways.
- Reduced production of inflammatory mediators
IL-1β signaling increases production of inflammatory mediators such as IL-6, TNF-alpha, prostaglandins, chemokines, adhesion molecules, and acute-phase proteins.
By blocking IL-1β activity, canakinumab reduces the inflammatory cascade. This leads to decreased fever, rash, joint pain, tissue inflammation, neutrophil recruitment, and systemic inflammatory symptoms.
- Effect on inflammasome-driven diseases
In cryopyrin-associated periodic syndromes, mutations in the NLRP3 gene cause overactivation of the inflammasome. This leads to excessive IL-1β release and recurrent inflammatory symptoms. The label notes that CAPS disorders are generally caused by NLRP3 mutations, resulting in an overactive inflammasome and excessive activated IL-1β release.
Canakinumab blocks the downstream cytokine product of this inflammasome activation, reducing inflammatory episodes.
- Effect in Still’s disease
Still’s disease, including systemic juvenile idiopathic arthritis and adult-onset Still’s disease, is an autoinflammatory disease driven by innate immune activation and pro-inflammatory cytokines such as IL-1β.
Canakinumab reduces IL-1β-mediated fever, systemic inflammation, rash, arthritis, pain, and elevated inflammatory markers.
- Effect in gout flares
In gout flares, monosodium urate crystals activate macrophages and the NLRP3 inflammasome, causing overproduction of IL-1β. IL-1β then drives acute joint inflammation with pain, redness, swelling, warmth, and neutrophil infiltration. The label specifically describes gout flares as involving resident macrophages, infiltrating neutrophils, and IL-1β overproduction triggered by uric acid crystals through NLRP3 inflammasome activation.
Canakinumab reduces this IL-1β-driven inflammatory response.
- Reduction of acute-phase response
IL-1β stimulates systemic acute-phase inflammation. This increases markers such as C-reactive protein and serum amyloid A. Canakinumab treatment reduces these inflammatory markers, and labeling notes that CRP and SAA normalize within 8 days in CAPS patients after ILARIS treatment.
- Final therapeutic effect
The final therapeutic effect of canakinumab is selective IL-1β blockade, reduced IL-1 receptor signaling, decreased inflammasome-driven inflammation, suppression of fever and systemic inflammatory symptoms, reduced joint and tissue inflammation, and improvement in IL-1β-mediated autoinflammatory diseases.
Pharmacokinetics
Canakinumab is administered by subcutaneous injection. It is not given orally because monoclonal antibodies would be degraded in the gastrointestinal tract.
Absorption:
After subcutaneous administration, canakinumab is slowly absorbed into systemic circulation. In adult CAPS patients receiving a single 150 mg subcutaneous dose, peak serum concentration occurred approximately 7 days after dosing. The estimated absolute bioavailability after subcutaneous administration is approximately 66%.
Distribution:
Canakinumab is an IgG1/kappa monoclonal antibody, so its distribution is mainly within vascular and extracellular fluid spaces. The apparent volume of distribution varies with body weight. In a typical 70 kg CAPS patient, the estimated steady-state volume of distribution is approximately 6.01 L.
Metabolism:
Canakinumab is not metabolized by cytochrome P450 enzymes. Like other therapeutic monoclonal antibodies, it is degraded by proteolytic catabolism into small peptides and amino acids.
Excretion:
Canakinumab is not primarily eliminated unchanged by the kidneys. Its clearance occurs mainly through normal protein catabolic pathways and is influenced by body weight.
Half-life and duration:
Canakinumab has a long mean terminal half-life of about 26 days after subcutaneous dosing. This long half-life supports extended dosing intervals, such as every 4 weeks, every 8 weeks, or at least 12 weeks between retreatment doses in gout flares depending on the indication.
Special pharmacokinetic point:
Inflammatory cytokines such as IL-1 can suppress CYP450 enzyme formation. By blocking IL-1β and reducing inflammation, canakinumab may normalize CYP450 activity. This can be clinically important for narrow therapeutic index drugs such as warfarin, where monitoring may be needed when canakinumab is started.
Clinical Uses
- Cryopyrin-associated periodic syndromes:
Canakinumab is used in adults and pediatric patients 4 years and older with CAPS, including familial cold autoinflammatory syndrome and Muckle-Wells syndrome. - Tumor necrosis factor receptor-associated periodic syndrome:
It is used in adult and pediatric patients with TRAPS, an autoinflammatory periodic fever syndrome. - Hyperimmunoglobulin D syndrome/mevalonate kinase deficiency:
Canakinumab is used in adult and pediatric patients with HIDS/MKD, conditions associated with recurrent inflammatory episodes. - Familial Mediterranean fever:
It is used in adult and pediatric patients with FMF, especially when IL-1β-driven inflammation contributes to recurrent fever and serositis. - Active Still’s disease:
Canakinumab is used in patients 2 years of age and older with active Still’s disease, including adult-onset Still’s disease and systemic juvenile idiopathic arthritis. - Gout flares in selected adults:
Canakinumab is used for symptomatic treatment of adult gout flares when NSAIDs and colchicine are contraindicated, not tolerated, or inadequate, and when repeated corticosteroid courses are not appropriate. - Inflammasome-driven inflammation:
Its mechanism is especially useful in diseases where excessive IL-1β release drives fever, rash, arthritis, serosal inflammation, and systemic inflammatory symptoms.
Adverse Effects
Common adverse effects of canakinumab include:
- Nasopharyngitis
- Upper respiratory tract infection
- Diarrhea
- Influenza
- Rhinitis
- Nausea
- Headache
- Bronchitis
- Gastroenteritis
- Pharyngitis
- Musculoskeletal pain
- Vertigo
- Injection-site reactions
- Abdominal pain
- Back pain
- Urinary tract infection
- Hypertriglyceridemia
Important serious or clinically significant adverse effects include:
- Serious infections
- Opportunistic infections
- Tuberculosis reactivation risk
- Hypersensitivity reactions
- Drug reaction with eosinophilia and systemic symptoms
- Immunosuppression-related malignancy concern
- Reduced vaccine response
- Risk with live vaccines
- Macrophage activation syndrome in Still’s disease patients
- Injection-site reactions
Canakinumab increases the risk of serious infections because IL-1β is part of normal host defense. The label advises caution in patients with infections or recurrent infection risk, avoidance during active infection requiring medical intervention, and discontinuation if a serious infection develops.
Live vaccines should be avoided during canakinumab therapy. Recommended vaccinations should be updated before starting therapy when feasible, because IL-1 blockade may interfere with immune response to infections and vaccines.
Macrophage activation syndrome is a life-threatening disorder that can occur in rheumatic conditions, especially Still’s disease. Clinicians should monitor for infection or worsening Still’s disease because these may trigger MAS.
Comparative Analysis
| Feature | Canakinumab | Anakinra | Rilonacept | Tocilizumab |
|---|---|---|---|---|
| Drug class | IL-1β monoclonal antibody | IL-1 receptor antagonist | IL-1 trap fusion protein | IL-6 receptor antagonist |
| Main target | IL-1β | IL-1 receptor | IL-1α and IL-1β | IL-6 receptor |
| Selectivity | Selective for IL-1β | Blocks IL-1 receptor signaling | Binds IL-1 cytokines | Blocks IL-6 signaling |
| Route | Subcutaneous | Subcutaneous | Subcutaneous | Intravenous or subcutaneous |
| Dosing style | Long interval | Usually daily | Weekly | Variable by indication |
| Major uses | Periodic fever syndromes, Still’s disease, selected gout flares | RA, autoinflammatory syndromes, selected off-label uses | CAPS, recurrent pericarditis | RA, GCA, CRS, SJIA, others |
| Key adverse concern | Infection, live vaccines, hypersensitivity | Injection reactions, infections | Infections, lipid changes | Infection, liver enzymes, GI perforation |
| Exam point | Selective IL-1β blockade | IL-1 receptor blockade | IL-1 cytokine trap | IL-6 receptor blockade |
Canakinumab differs from anakinra because canakinumab binds IL-1β directly, while anakinra blocks the IL-1 receptor. Rilonacept acts as a soluble decoy receptor that traps IL-1 cytokines. Tocilizumab targets a different cytokine pathway by blocking IL-6 receptor signaling. Canakinumab is especially remembered as a long-acting monoclonal antibody selective for IL-1β.
MCQs
- Canakinumab is marketed under which brand name?
a) Humira
b) Ilaris
c) Actemra
d) Kineret
Answer: b) Ilaris
- Canakinumab primarily targets:
a) TNF-alpha
b) IL-6 receptor
c) IL-1 beta
d) CD20
Answer: c) IL-1 beta
- Canakinumab belongs to which drug class?
a) IL-1β-blocking monoclonal antibody
b) Calcineurin inhibitor
c) JAK inhibitor
d) Antimetabolite
Answer: a) IL-1β-blocking monoclonal antibody
- The main effect of canakinumab is to prevent IL-1β from binding to:
a) IL-1 receptors
b) Beta receptors
c) Dopamine receptors
d) Histamine receptors
Answer: a) IL-1 receptors
- Canakinumab does not bind significantly to:
a) IL-1α or IL-1 receptor antagonist
b) IL-1β
c) Human IL-1β
d) Circulating IL-1β
Answer: a) IL-1α or IL-1 receptor antagonist
- Which inflammasome is strongly associated with CAPS and gout flare IL-1β production?
a) NLRP3 inflammasome
b) Proteasome
c) Ribosome
d) Spliceosome
Answer: a) NLRP3 inflammasome
- Cryopyrin-associated periodic syndromes are commonly related to mutations in:
a) NLRP3
b) EGFR
c) HER2
d) BCR-ABL
Answer: a) NLRP3
- Canakinumab reduces which acute-phase markers?
a) CRP and serum amyloid A
b) Troponin and myoglobin only
c) Insulin and glucagon
d) Hemoglobin and albumin only
Answer: a) CRP and serum amyloid A
- Canakinumab is used in active Still’s disease including:
a) AOSD and SJIA
b) COPD and asthma
c) Type 1 and type 2 diabetes
d) Hypertension and angina
Answer: a) AOSD and SJIA
- Canakinumab is administered by which route?
a) Subcutaneous injection
b) Oral tablet
c) Inhalation
d) Sublingual tablet
Answer: a) Subcutaneous injection
- Which adverse effect is clinically important with canakinumab?
a) Serious infection
b) Severe hypoglycemia
c) Ototoxicity
d) Gingival hyperplasia
Answer: a) Serious infection
- Live vaccines during canakinumab therapy should generally be:
a) Avoided
b) Given weekly
c) Used to increase absorption
d) Given with every dose
Answer: a) Avoided
- Which life-threatening syndrome requires monitoring in Still’s disease patients?
a) Macrophage activation syndrome
b) Serotonin syndrome only
c) Acute angle-closure glaucoma
d) Reye syndrome only
Answer: a) Macrophage activation syndrome
- Canakinumab differs from anakinra because anakinra:
a) Blocks the IL-1 receptor
b) Blocks CD20
c) Inhibits JAK1
d) Blocks VEGF
Answer: a) Blocks the IL-1 receptor
- Which statement about canakinumab is correct?
a) It neutralizes IL-1β and reduces IL-1 receptor-mediated inflammation
b) It directly replaces insulin
c) It blocks bacterial cell wall synthesis
d) It is a rescue bronchodilator
Answer: a) It neutralizes IL-1β and reduces IL-1 receptor-mediated inflammation
FAQs
- What is canakinumab used for?
Canakinumab is used for IL-1β-mediated inflammatory diseases, including cryopyrin-associated periodic syndromes, TRAPS, HIDS/MKD, familial Mediterranean fever, active Still’s disease including AOSD and SJIA, and selected adult gout flares.
- What is the mechanism of action of canakinumab?
Canakinumab is a human monoclonal antibody that binds interleukin-1 beta and neutralizes its activity. It prevents IL-1β from binding IL-1 receptors, thereby reducing inflammatory signaling.
- Is canakinumab a steroid?
No. Canakinumab is not a steroid. It is a targeted biologic monoclonal antibody that blocks IL-1β.
- Does canakinumab block IL-1 alpha?
No. Canakinumab selectively binds IL-1β and does not bind IL-1α or IL-1 receptor antagonist.
- Why is canakinumab useful in CAPS?
CAPS is commonly associated with NLRP3 inflammasome overactivation, causing excessive IL-1β release. Canakinumab neutralizes IL-1β and reduces the resulting inflammation.
- How does canakinumab help gout flares?
In gout flares, urate crystals activate macrophages and the NLRP3 inflammasome, leading to IL-1β overproduction. Canakinumab blocks IL-1β and reduces acute inflammatory joint symptoms in selected adult patients.
- What are common side effects of canakinumab?
Common side effects include nasopharyngitis, upper respiratory infections, diarrhea, influenza, nausea, headache, bronchitis, abdominal pain, injection-site reactions, and musculoskeletal pain.
- What is the most important safety risk of canakinumab?
Serious infection is one of the most important risks because IL-1β blockade can impair immune defense against infections.
- Can live vaccines be given with canakinumab?
Live vaccines should generally be avoided during canakinumab therapy. Recommended vaccinations should be updated before treatment when possible.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

