
Table of Contents
Introduction
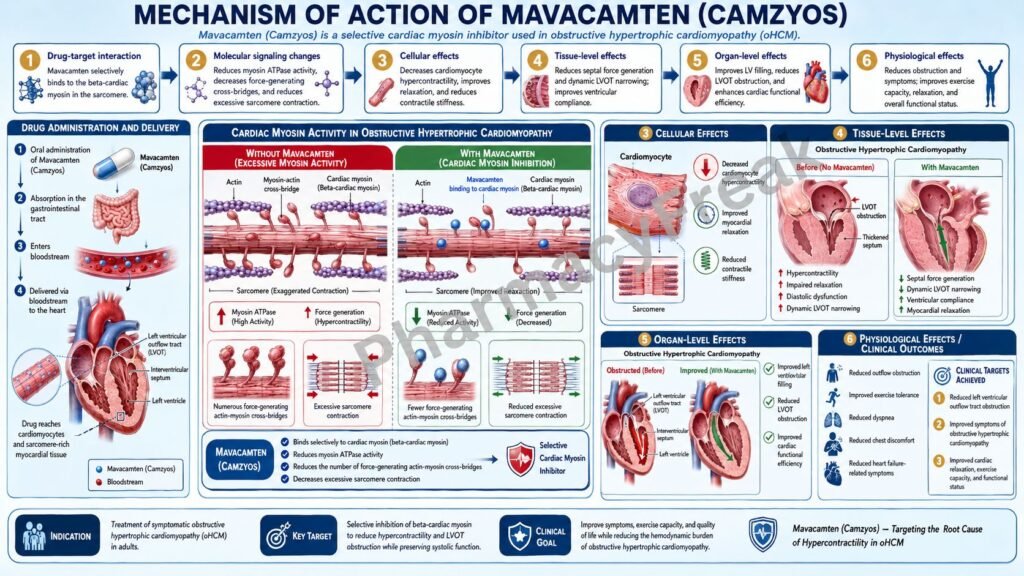
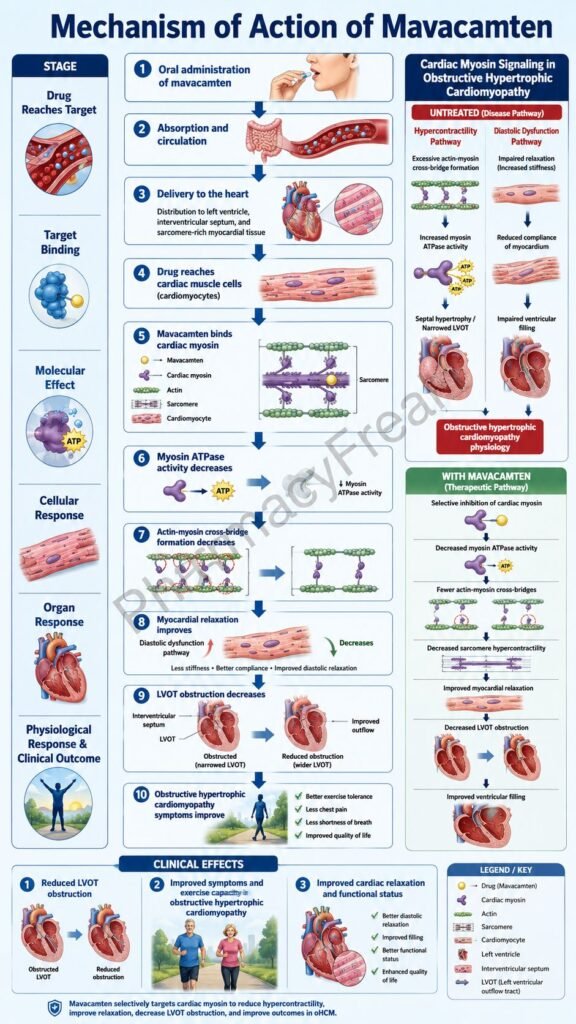
Mavacamten is an oral cardiac myosin inhibitor marketed under the brand name Camzyos. It is used for the treatment of adults with symptomatic New York Heart Association class II–III obstructive hypertrophic cardiomyopathy, also called obstructive HCM or oHCM, to improve functional capacity and symptoms. Current prescribing information describes Camzyos as a cardiac myosin inhibitor and lists its approved indication specifically for symptomatic obstructive HCM in adults.
Hypertrophic cardiomyopathy is a genetic or familial heart muscle disorder characterized by abnormal thickening of the myocardium, especially the interventricular septum. In obstructive HCM, this thickened septum and abnormal mitral valve motion can narrow the left ventricular outflow tract. This leads to increased left ventricular outflow tract gradient, shortness of breath, chest pain, fatigue, palpitations, syncope, and exercise limitation.
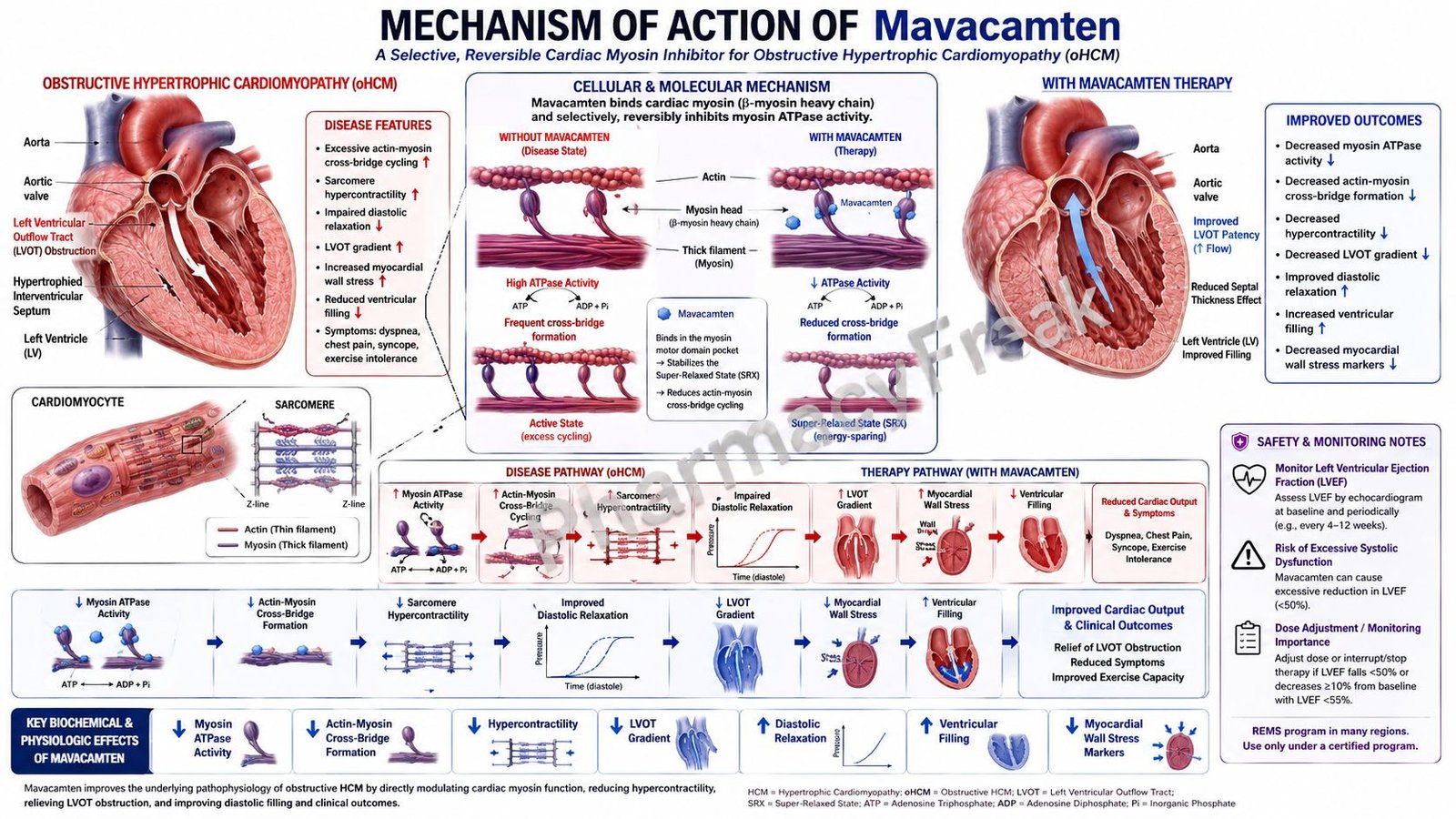
Mavacamten is pharmacologically important because it treats obstructive HCM at the level of the sarcomere, the basic contractile unit of cardiac muscle. Unlike beta-blockers or calcium channel blockers, which mainly reduce heart rate and contractility indirectly, mavacamten directly modulates cardiac myosin activity. It reduces excessive actin-myosin cross-bridge formation and shifts myosin toward an energy-sparing super-relaxed state.
For pharmacy, medical, nursing, and competitive exam students, mavacamten is important because it represents a disease-specific targeted therapy for obstructive hypertrophic cardiomyopathy. Its key mechanism is reversible allosteric inhibition of cardiac myosin, leading to reduced hypercontractility, reduced left ventricular outflow tract obstruction, improved cardiac filling pressures, and improved symptoms in suitable patients.
Mechanism of Action (Step-wise)
- Primary target: Cardiac myosin
Mavacamten selectively targets cardiac myosin. Cardiac myosin is the motor protein in heart muscle that interacts with actin to produce contraction.
In normal cardiac muscle, myosin heads bind actin, hydrolyze ATP, and generate force through cross-bridge cycling. In hypertrophic cardiomyopathy, excessive myosin-actin interaction contributes to hypercontractility, inefficient energy use, impaired relaxation, and obstruction of blood flow out of the left ventricle.
- Allosteric and reversible inhibition
Mavacamten is an allosteric and reversible inhibitor of cardiac myosin. Allosteric inhibition means the drug binds to a regulatory site and changes myosin behavior rather than simply blocking the active site like a competitive enzyme inhibitor.
Reversible inhibition means its effects can lessen after drug discontinuation as drug levels fall. This reversibility is clinically important because excessive myosin inhibition can reduce systolic function.
- Reduction in available myosin heads
Mavacamten modulates the number of myosin heads that can enter the “on actin” force-generating state. Fewer myosin heads become available for strong actin binding and power generation.
This reduces excessive systolic force generation, which is a central abnormality in obstructive HCM.
- Reduced actin-myosin cross-bridge formation
In cardiac muscle contraction, myosin heads bind to actin filaments and form cross-bridges. These cross-bridges generate force during systole.
In obstructive HCM, excessive myosin-actin cross-bridge formation contributes to hyperdynamic contraction and left ventricular outflow tract obstruction. Mavacamten reduces both force-producing systolic cross-bridge formation and residual diastolic cross-bridge formation.
- Shift toward the super-relaxed state
Mavacamten shifts more myosin heads into an energy-sparing, recruitable, super-relaxed state. This means fewer myosin heads are actively consuming ATP and generating force at any given time.
This improves the abnormal energetic burden seen in hypertrophic cardiomyopathy and reduces excessive contraction.
- Reduced left ventricular hypercontractility
By decreasing excessive myosin activity, mavacamten reduces left ventricular hypercontractility. This is useful because obstructive HCM is often associated with excessive contractile force and dynamic obstruction.
The goal is not to stop contraction. The goal is to bring excessive sarcomere activity closer to normal.
- Reduced left ventricular outflow tract obstruction
In obstructive HCM, strong contraction can worsen systolic anterior motion of the mitral valve and increase left ventricular outflow tract obstruction. By reducing hypercontractility, mavacamten reduces the dynamic LVOT gradient.
Clinical pharmacodynamic data show reductions in resting and provoked LVOT gradients during treatment. In the EXPLORER-HCM trial, mean resting and Valsalva LVOT gradients decreased by week 4 and were sustained through 30 weeks.
- Improved cardiac filling pressures
Excessive residual cross-bridge formation during diastole can impair relaxation and filling. By reducing residual diastolic cross-bridge formation, mavacamten may improve diastolic function and filling pressures.
This contributes to improved exercise capacity and reduction in symptoms such as dyspnea and fatigue.
- Reduction in cardiac wall stress biomarkers
Mavacamten therapy is associated with reductions in biomarkers of cardiac wall stress, including NT-proBNP. In clinical trial data, reductions in NT-proBNP were observed by week 4 and sustained through treatment.
This supports the idea that mavacamten reduces hemodynamic stress in obstructive HCM.
- Final therapeutic effect
The final therapeutic effect of mavacamten is reversible inhibition of cardiac myosin, reduced excessive actin-myosin cross-bridge formation, decreased hypercontractility, reduced LVOT obstruction, improved filling pressures, improved exercise capacity, and symptomatic improvement in adults with NYHA class II–III obstructive hypertrophic cardiomyopathy.
Pharmacokinetics
Mavacamten is administered orally as Camzyos capsules. Available capsule strengths include 2.5 mg, 5 mg, 10 mg, and 15 mg. The recommended starting dose is 5 mg once daily, with individualized titration based on clinical status and echocardiographic response. The maximum recommended dose is 15 mg once daily.
Absorption:
Mavacamten has an estimated oral bioavailability of at least 85%. Median time to maximum plasma concentration is approximately 1 to 2 hours. A high-fat meal does not produce a clinically significant change in mavacamten exposure, so it may be taken without regard to food.
Distribution:
Mavacamten is highly protein-bound. Plasma protein binding is approximately 97% to 98%. Because it is an oral small molecule, it distributes systemically and reaches cardiac tissue to modulate sarcomere function.
Metabolism:
Mavacamten is extensively metabolized, mainly by CYP2C19, with additional contribution from CYP3A4 and CYP2C9. Labeling estimates metabolism through CYP2C19 at about 74%, CYP3A4 at about 18%, and CYP2C9 at about 8%.
Excretion:
After a radiolabeled dose, about 85% of the dose was recovered in urine and about 7% in feces. Only a small fraction was recovered as unchanged drug, showing that metabolism is the major elimination pathway.
Half-life and duration:
The terminal half-life depends strongly on CYP2C19 metabolizer status. In CYP2C19 normal metabolizers, the terminal half-life is about 6 to 9 days. In CYP2C19 poor metabolizers, the half-life is prolonged to about 23 days.
Special pharmacokinetic point:
Genetic variation in CYP2C19 can greatly affect mavacamten exposure. CYP2C19 poor metabolizers have higher exposure and longer half-life, increasing the need for careful dose titration and monitoring. Drug interactions with CYP2C19 and CYP3A4 inhibitors or inducers are clinically important because excessive exposure can increase heart failure risk, while reduced exposure can decrease effectiveness.
Clinical Uses
- Symptomatic obstructive hypertrophic cardiomyopathy:
Mavacamten is used in adults with symptomatic NYHA class II–III obstructive HCM to improve functional capacity and symptoms. - Reduction of LVOT obstruction:
It is used when dynamic left ventricular outflow tract obstruction contributes to symptoms such as dyspnea, chest discomfort, fatigue, presyncope, or exercise intolerance. - Sarcomere-targeted therapy:
Mavacamten is useful because it directly targets the excessive cardiac myosin activity that contributes to hypercontractility and obstruction in HCM. - Functional capacity improvement:
By reducing obstruction and cardiac wall stress, mavacamten can improve exercise capacity in selected patients. - Symptom improvement:
Patients with obstructive HCM may experience improvement in shortness of breath, fatigue, chest discomfort, and activity limitation when therapy is appropriately monitored. - Alternative or add-on approach in oHCM management:
Mavacamten is not simply a heart-rate-lowering drug. It offers a targeted approach focused on abnormal sarcomere mechanics, although it requires strict echocardiographic monitoring because excessive reduction in contractility can be dangerous.
Adverse Effects
Common adverse effects of mavacamten include:
- Dizziness
- Syncope
- Fatigue
- Dyspnea
- Palpitations
- Chest discomfort
- Reduced left ventricular ejection fraction
- Possible worsening heart failure symptoms
The most common adverse reactions reported in the label were dizziness and syncope, occurring more commonly with Camzyos than placebo in clinical trials.
Important serious or clinically significant adverse effects include:
- Heart failure due to systolic dysfunction
- Excessive reduction in left ventricular ejection fraction
- Worsening dyspnea
- Chest pain
- Palpitations
- Leg edema
- Rapid weight gain
- Hypotension in overdose
- Syncope
- Embryo-fetal toxicity
- Drug interaction-related toxicity
The boxed warning is a major exam point. Camzyos reduces left ventricular ejection fraction and can cause heart failure due to systolic dysfunction. Echocardiographic assessment of LVEF is required before and during treatment. Initiation is not recommended when LVEF is below 55%, and treatment should be interrupted if LVEF falls below 50% or if heart failure symptoms or worsening clinical status occur.
Mavacamten is available only through the Camzyos REMS Program because of the risk of heart failure due to systolic dysfunction. The REMS program requires certified prescribers, patient enrollment, ongoing monitoring, and certified pharmacies.
Drug interactions are clinically important. Camzyos is contraindicated with strong CYP2C19 inhibitors and with moderate to strong CYP2C19 inducers or moderate to strong CYP3A4 inducers. Negative inotropes can have additive effects, and labeling advises avoiding certain combinations such as disopyramide, ranolazine, verapamil with a beta-blocker, or diltiazem with a beta-blocker.
Comparative Analysis
| Feature | Mavacamten | Beta-Blockers | Verapamil/Diltiazem | Disopyramide |
|---|---|---|---|---|
| Drug class | Cardiac myosin inhibitor | Beta-adrenergic blockers | Non-dihydropyridine calcium channel blockers | Class IA antiarrhythmic with negative inotropic effect |
| Main target | Cardiac myosin | Beta-1 receptors | L-type calcium channels | Sodium channels and myocardial contractility |
| Main action | Reduces excessive actin-myosin cross-bridging | Reduces heart rate and contractility | Reduces heart rate, contractility, and AV conduction | Reduces contractility and arrhythmias |
| Disease role | Targeted therapy for obstructive HCM | Symptom control in HCM | Symptom control in selected HCM patients | Used in selected obstructive HCM patients |
| Effect on LVOT gradient | Directly reduces hypercontractility and obstruction | Indirect reduction by reducing contractility/heart rate | Indirect reduction | Negative inotropic reduction |
| Route | Oral | Oral or IV depending on drug | Oral or IV depending on drug | Oral |
| Major safety concern | Reduced LVEF, heart failure, REMS monitoring | Bradycardia, hypotension, fatigue | Bradycardia, hypotension, worsening HF | Anticholinergic effects, QT prolongation, proarrhythmia |
| Exam point | First-in-class cardiac myosin inhibitor for oHCM | First-line symptom control in many patients | Avoid in some patients with severe obstruction or HF risk | Negative inotrope with arrhythmia concerns |
Mavacamten differs from beta-blockers and calcium channel blockers because it directly targets cardiac myosin at the sarcomere level. Beta-blockers and non-dihydropyridine calcium channel blockers mainly reduce heart rate and contractility through receptor or calcium-channel effects. Disopyramide also reduces contractility but is an antiarrhythmic with anticholinergic and proarrhythmic concerns. Mavacamten is unique because it reduces excessive cardiac myosin-actin cross-bridge formation, but this same mechanism can also reduce LVEF too much if exposure is excessive.
MCQs
- Mavacamten is marketed under which brand name?
a) Entresto
b) Camzyos
c) Corlanor
d) Jardiance
Answer: b) Camzyos
- Mavacamten belongs to which drug class?
a) Cardiac myosin inhibitor
b) ACE inhibitor
c) Loop diuretic
d) Beta-blocker
Answer: a) Cardiac myosin inhibitor
- Mavacamten is mainly used for:
a) Symptomatic obstructive hypertrophic cardiomyopathy
b) Acute bacterial endocarditis
c) Ventricular fibrillation arrest
d) Hyperthyroidism
Answer: a) Symptomatic obstructive hypertrophic cardiomyopathy
- The primary molecular target of mavacamten is:
a) Cardiac myosin
b) Angiotensin-converting enzyme
c) Sodium-glucose cotransporter 2
d) Beta-2 receptor
Answer: a) Cardiac myosin
- Mavacamten reduces cardiac contraction by decreasing:
a) Actin-myosin cross-bridge formation
b) Hemoglobin synthesis
c) Bacterial protein synthesis
d) Platelet aggregation
Answer: a) Actin-myosin cross-bridge formation
- Mavacamten shifts myosin toward which state?
a) Super-relaxed state
b) Fully activated inflammatory state
c) Irreversible denatured state
d) Glycogen-bound state
Answer: a) Super-relaxed state
- The main hemodynamic effect of mavacamten in obstructive HCM is reduction of:
a) LVOT gradient
b) Blood glucose
c) Pulmonary surfactant
d) Gastric acid secretion
Answer: a) LVOT gradient
- Which monitoring is essential before and during mavacamten therapy?
a) Echocardiographic LVEF monitoring
b) Daily sputum culture
c) Serum amylase only
d) Audiometry only
Answer: a) Echocardiographic LVEF monitoring
- Initiation of mavacamten is not recommended if LVEF is:
a) Below 55%
b) Above 70%
c) Exactly 60%
d) Above 80%
Answer: a) Below 55%
- Mavacamten should be interrupted if LVEF falls below:
a) 50%
b) 80%
c) 75%
d) 65%
Answer: a) 50%
- The major boxed warning of mavacamten involves:
a) Heart failure due to systolic dysfunction
b) Severe ototoxicity
c) Gingival hyperplasia
d) Tendon rupture
Answer: a) Heart failure due to systolic dysfunction
- Mavacamten is primarily metabolized by:
a) CYP2C19
b) Acetylcholinesterase
c) Monoamine oxidase-B
d) Alcohol dehydrogenase only
Answer: a) CYP2C19
- Which CYP phenotype may have prolonged mavacamten half-life?
a) CYP2C19 poor metabolizer
b) CYP2D6 ultra-rapid metabolizer only
c) CYP1A2 rapid metabolizer only
d) CYP2E1 poor metabolizer only
Answer: a) CYP2C19 poor metabolizer
- Which adverse effect was reported more commonly with mavacamten than placebo in trials?
a) Dizziness
b) Severe hypoglycemia
c) Ototoxicity
d) Nephrolithiasis
Answer: a) Dizziness
- Which statement about mavacamten is correct?
a) It reversibly inhibits cardiac myosin and reduces excessive myosin-actin cross-bridge formation
b) It directly blocks aldosterone receptors
c) It inhibits bacterial cell wall synthesis
d) It stimulates beta-1 receptors to increase contractility
Answer: a) It reversibly inhibits cardiac myosin and reduces excessive myosin-actin cross-bridge formation
FAQs
- What is mavacamten used for?
Mavacamten is used for adults with symptomatic NYHA class II–III obstructive hypertrophic cardiomyopathy to improve functional capacity and symptoms.
- What is the mechanism of action of mavacamten?
Mavacamten is a reversible allosteric inhibitor of cardiac myosin. It reduces the number of myosin heads available for actin binding, decreases excessive actin-myosin cross-bridge formation, and shifts myosin toward an energy-sparing super-relaxed state.
- Is mavacamten a beta-blocker?
No. Mavacamten is not a beta-blocker. It directly targets cardiac myosin, whereas beta-blockers reduce heart rate and contractility through beta-adrenergic receptor blockade.
- How does mavacamten help obstructive HCM?
In obstructive HCM, excessive cardiac contraction contributes to left ventricular outflow tract obstruction. Mavacamten reduces hypercontractility and lowers LVOT gradient, improving symptoms and functional capacity.
- Why does mavacamten require echocardiography?
Mavacamten can reduce left ventricular ejection fraction. Echocardiography is required before and during therapy to monitor LVEF and LVOT gradient and to reduce the risk of heart failure.
- What is the most important safety risk of mavacamten?
The most important risk is heart failure due to systolic dysfunction. Treatment should be interrupted if LVEF falls below 50% or if the patient develops heart failure symptoms or worsening clinical status.
- What are common side effects of mavacamten?
Common side effects include dizziness and syncope. Other clinically important symptoms to monitor include shortness of breath, chest pain, fatigue, palpitations, leg swelling, and rapid weight gain.
- Which enzymes metabolize mavacamten?
Mavacamten is mainly metabolized by CYP2C19, with additional metabolism by CYP3A4 and CYP2C9.
- Why is mavacamten available through a REMS program?
Mavacamten can cause heart failure due to excessive reduction in systolic function. The REMS program ensures appropriate prescribing, patient enrollment, pharmacy certification, and required cardiac monitoring.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

