
Table of Contents
Introduction
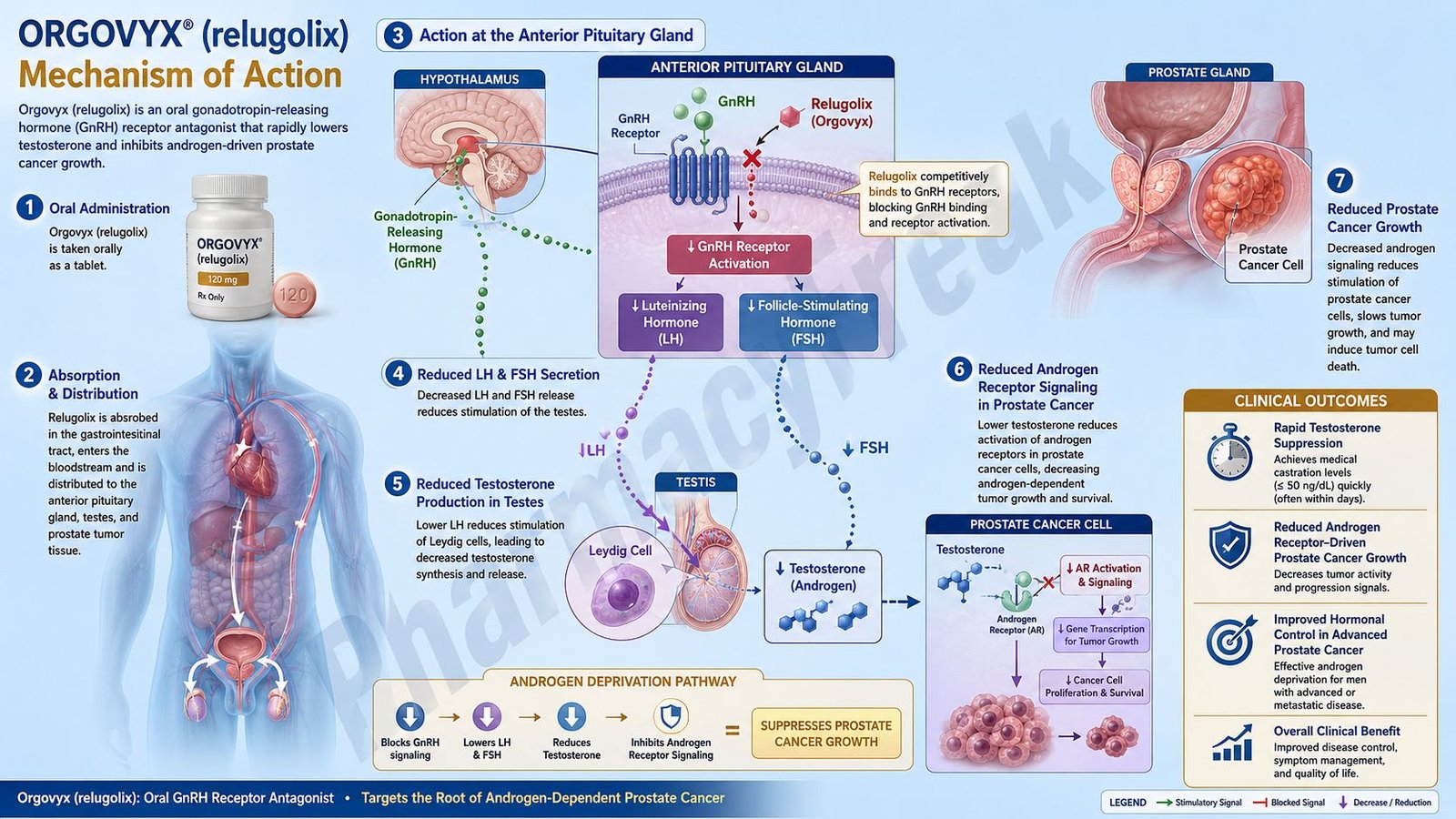
Orgovyx is the brand name of relugolix, an oral hormonal anticancer drug used in adult patients with advanced prostate cancer. Pharmacologically, Orgovyx is a gonadotropin-releasing hormone receptor antagonist, also called a GnRH receptor antagonist or LHRH receptor antagonist.
Prostate cancer growth is commonly driven by androgen signaling, especially testosterone and dihydrotestosterone. Testosterone is mainly produced by the testes under the control of the hypothalamic-pituitary-gonadal axis. In advanced prostate cancer, reducing testosterone to castrate levels is an important therapeutic strategy because it deprives androgen-sensitive cancer cells of a major growth stimulus.
Relugolix works by competitively blocking GnRH receptors in the anterior pituitary gland. This prevents natural GnRH from stimulating release of luteinizing hormone and follicle-stimulating hormone. Reduced LH secretion leads to rapid suppression of testicular testosterone production. Lower testosterone levels reduce androgen receptor activation in prostate cancer cells and help slow tumor growth.
Orgovyx is indicated for the treatment of adult patients with advanced prostate cancer. The recommended dosing starts with a 360 mg loading dose on Day 1, followed by 120 mg orally once daily.
For exam purposes, Orgovyx should be remembered as an oral GnRH receptor antagonist that rapidly lowers LH, FSH, and testosterone without the initial testosterone flare seen with GnRH agonists such as leuprolide.
Mechanism of Action (Step-wise)
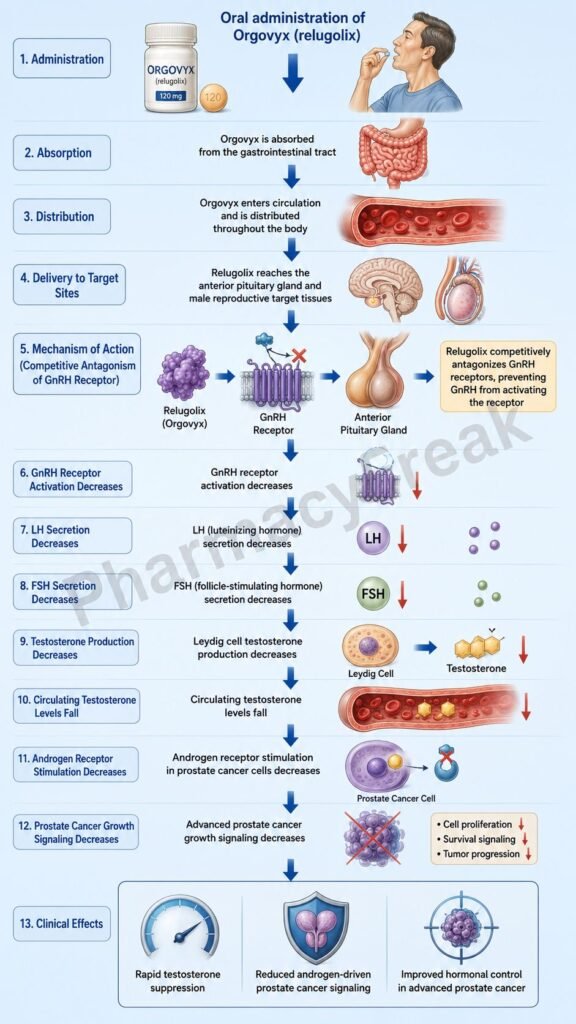
Step 1: The hypothalamus releases GnRH
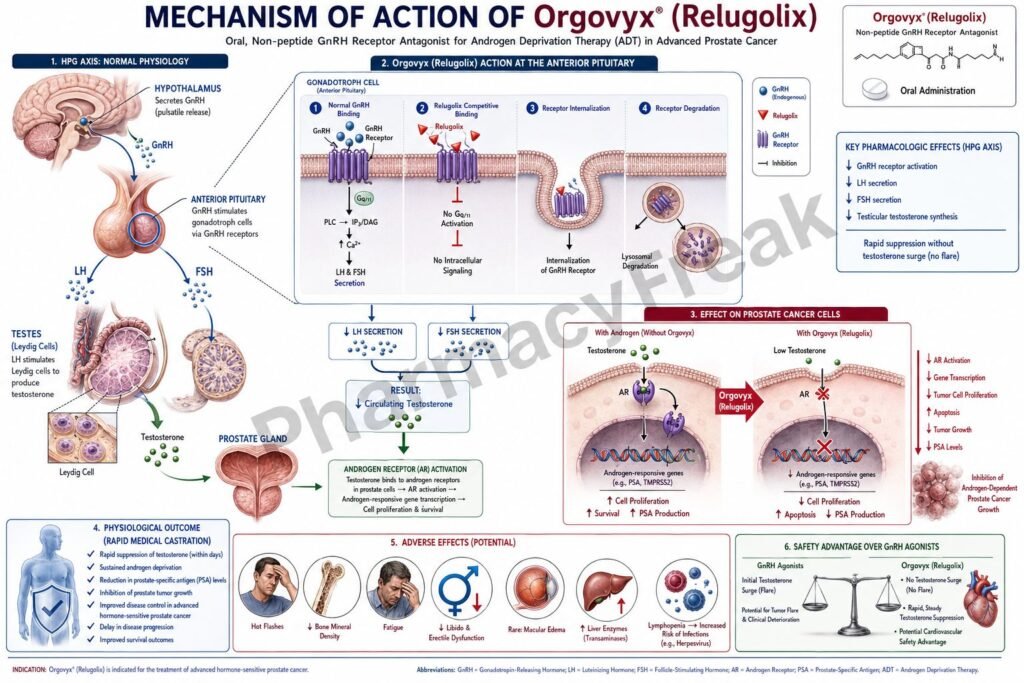
In normal male reproductive physiology, the hypothalamus releases gonadotropin-releasing hormone in pulses. GnRH travels to the anterior pituitary gland through the hypophyseal portal circulation.
Step 2: GnRH stimulates pituitary GnRH receptors
GnRH binds to GnRH receptors on anterior pituitary gonadotroph cells. This receptor activation stimulates secretion of luteinizing hormone and follicle-stimulating hormone.
Step 3: LH stimulates testosterone production
Luteinizing hormone acts on Leydig cells in the testes and stimulates testosterone synthesis. Testosterone then circulates in blood and can be converted to dihydrotestosterone in some tissues.
Step 4: Testosterone activates androgen receptors
Testosterone and dihydrotestosterone bind androgen receptors in prostate cells. In androgen-sensitive prostate cancer, this signaling promotes cancer-cell survival, proliferation, and disease progression.
Step 5: Advanced prostate cancer often depends on androgen signaling
Many prostate cancer cells remain dependent on androgen receptor signaling, especially earlier in advanced disease. Therefore, androgen deprivation therapy aims to reduce testosterone levels and limit androgen receptor stimulation.
Step 6: Orgovyx blocks pituitary GnRH receptors
Relugolix competitively binds to GnRH receptors in the anterior pituitary gland. By occupying these receptors, it prevents endogenous GnRH from activating them. This is the central molecular mechanism of Orgovyx.
Step 7: LH and FSH secretion decrease
When GnRH receptor signaling is blocked, pituitary release of LH and FSH falls. LH suppression is especially important because LH is the main hormonal driver of testicular testosterone production.
Step 8: Testicular testosterone production decreases
Reduced LH stimulation leads to decreased testosterone synthesis by Leydig cells. Relugolix reduces testosterone concentrations after the oral loading dose and continued once-daily dosing.
Step 9: Castrate testosterone levels are achieved
The therapeutic goal of androgen deprivation therapy is to suppress testosterone to castrate levels. Lower testosterone decreases androgen receptor activation in prostate cancer cells.
Step 10: Prostate cancer growth signaling decreases
With less testosterone available, androgen receptor-driven transcription decreases. This reduces expression of genes involved in prostate cancer growth, survival, and progression.
Step 11: No initial testosterone flare occurs
A key advantage of GnRH antagonists is that they directly block GnRH receptors. GnRH agonists initially stimulate receptors before downregulation, causing a temporary testosterone surge or flare. Orgovyx avoids this initial flare because it is an antagonist.
Step 12: Testosterone recovery may occur after discontinuation
After stopping Orgovyx, pituitary GnRH receptor blockade decreases over time, allowing LH and testosterone production to recover. This reversibility is clinically relevant when planning treatment duration, adverse effect management, and follow-up.
Step 13: Final therapeutic outcome
The final therapeutic outcome is rapid androgen deprivation. This helps control advanced prostate cancer by lowering testosterone, reducing androgen receptor stimulation, and slowing growth of androgen-sensitive tumor cells.
Pharmacokinetics
Orgovyx is administered orally as a tablet. This is clinically important because many other androgen deprivation therapies are injectable depot formulations. The standard regimen begins with a 360 mg loading dose on the first day, followed by 120 mg once daily at approximately the same time each day.
Relugolix may be taken with or without food. Tablets should be swallowed whole and should not be crushed or chewed.
Relugolix is absorbed after oral administration and produces pharmacological suppression of LH, FSH, and testosterone. The loading dose helps achieve rapid hormone suppression early in treatment.
Relugolix is a substrate of P-glycoprotein. This is an important drug interaction point. Oral P-glycoprotein inhibitors can increase relugolix exposure. If coadministration cannot be avoided, Orgovyx should be taken first and separated from the P-glycoprotein inhibitor by at least 6 hours according to labeling guidance.
Combined P-glycoprotein and strong CYP3A inducers can reduce relugolix exposure and may decrease effectiveness. If such combination cannot be avoided, the Orgovyx dose may need adjustment according to prescribing guidance.
Because Orgovyx is taken daily, adherence is very important. Missed doses may reduce continuous testosterone suppression. If treatment is interrupted for more than 7 days, restarting with the loading dose may be required according to product guidance.
Clinical Uses
Orgovyx is used for adult patients with advanced prostate cancer. Its purpose is androgen deprivation, meaning reduction of testosterone to levels that limit androgen receptor-driven tumor growth.
It is useful when a clinician wants medical castration without surgical removal of the testes. It provides an oral option for androgen deprivation therapy, unlike injectable GnRH agonists or injectable GnRH antagonists.
Orgovyx is not a chemotherapy drug. It does not directly damage DNA like docetaxel or platinum-based chemotherapy. It is a hormonal therapy that targets the hypothalamic-pituitary-gonadal axis.
Orgovyx is not the same as relugolix combination products used in gynecological conditions. Orgovyx contains relugolix alone and is used for advanced prostate cancer.
It may be used alone or as part of a broader prostate cancer treatment plan depending on disease stage, risk category, metastatic status, symptoms, radiation plan, systemic therapy plan, and oncologist decision.
Adverse Effects
The adverse effects of Orgovyx are mainly related to testosterone suppression and drug-specific safety warnings.
Common adverse reactions include hot flushes, increased glucose, increased triglycerides, musculoskeletal pain, decreased hemoglobin, increased liver enzymes, fatigue, constipation, and diarrhea.
Hot flushes occur because androgen deprivation alters hypothalamic thermoregulation. Patients may experience sudden warmth, sweating, flushing, sleep disturbance, or discomfort.
Metabolic effects are important. Androgen deprivation therapy can worsen glucose control, increase lipids, promote weight gain, reduce muscle mass, and increase cardiometabolic risk. Monitoring is important in patients with diabetes, obesity, cardiovascular disease, or metabolic syndrome.
Musculoskeletal effects can occur because testosterone is important for muscle and bone health. Long-term androgen deprivation may contribute to fatigue, muscle loss, decreased strength, osteoporosis, and fracture risk.
QT or QTc interval prolongation is an important warning with androgen deprivation therapy, including Orgovyx. Caution is needed in patients with congenital long QT syndrome, electrolyte abnormalities, heart disease, or drugs that prolong QT interval.
Embryo-fetal toxicity is an important safety warning. Based on animal findings and mechanism of action, Orgovyx can cause fetal harm and pregnancy loss if administered to a pregnant female.
Severe hypersensitivity to relugolix or any component is a contraindication. Patients should seek urgent care for swelling, rash, breathing difficulty, or severe allergic symptoms.
Other possible androgen deprivation effects include reduced libido, erectile dysfunction, mood changes, gynecomastia, breast tenderness, anemia, and reduced quality of life. Patients should be counseled that many adverse effects are related to testosterone lowering.
Comparative Analysis
Orgovyx is commonly compared with GnRH agonists such as leuprolide, goserelin, triptorelin, and histrelin.
Compared with GnRH agonists, Orgovyx directly blocks GnRH receptors and does not cause an initial testosterone flare. GnRH agonists first stimulate GnRH receptors, causing a temporary rise in LH and testosterone before receptor downregulation suppresses testosterone.
Compared with leuprolide, Orgovyx is taken orally once daily, while leuprolide is given as an injection or depot formulation. This makes Orgovyx convenient for some patients but also makes daily adherence essential.
Compared with degarelix, Orgovyx is also a GnRH antagonist, but degarelix is administered by subcutaneous injection. Both avoid testosterone flare, but they differ in route, dosing schedule, and injection-site issues.
Compared with antiandrogens such as bicalutamide, enzalutamide, apalutamide, and darolutamide, Orgovyx reduces testosterone production upstream. Antiandrogens block androgen receptor signaling at the receptor level, while Orgovyx suppresses testicular testosterone production through pituitary GnRH receptor blockade.
Compared with abiraterone, Orgovyx has a different hormonal target. Abiraterone inhibits CYP17 and reduces androgen synthesis in the testes, adrenal glands, and tumor tissue. Orgovyx suppresses pituitary LH and thereby reduces testicular testosterone production.
Compared with orchiectomy, Orgovyx provides medical rather than surgical castration. Orchiectomy permanently removes the main source of testosterone, while Orgovyx produces reversible testosterone suppression when therapy is stopped.
MCQs
- Orgovyx contains which active drug?
a) Leuprolide
b) Relugolix
c) Degarelix
d) Bicalutamide
Answer: b) Relugolix
- Orgovyx belongs to which pharmacological class?
a) GnRH receptor antagonist
b) GnRH receptor agonist
c) Androgen receptor blocker
d) Aromatase inhibitor
Answer: a) GnRH receptor antagonist
- Orgovyx is mainly used for:
a) Advanced prostate cancer
b) Breast cancer prevention
c) Benign prostatic hyperplasia only
d) Acute bacterial prostatitis
Answer: a) Advanced prostate cancer
- Relugolix acts primarily at which site?
a) Anterior pituitary GnRH receptors
b) Prostate alpha-1 receptors
c) Testicular androgen receptors only
d) Adrenal mineralocorticoid receptors
Answer: a) Anterior pituitary GnRH receptors
- Blocking GnRH receptors reduces secretion of:
a) LH and FSH
b) Insulin and glucagon
c) TSH and prolactin only
d) Cortisol and aldosterone
Answer: a) LH and FSH
- Reduced LH secretion leads to decreased production of:
a) Testosterone
b) Thyroxine
c) Insulin
d) Aldosterone
Answer: a) Testosterone
- Orgovyx differs from leuprolide because Orgovyx:
a) Directly blocks GnRH receptors without testosterone flare
b) Initially increases testosterone by receptor stimulation
c) Is a cytotoxic chemotherapy drug
d) Blocks bacterial DNA replication
Answer: a) Directly blocks GnRH receptors without testosterone flare
- The recommended Day 1 loading dose of Orgovyx is:
a) 360 mg
b) 40 mg
c) 80 mg
d) 1,000 mg
Answer: a) 360 mg
- The usual maintenance dose of Orgovyx is:
a) 120 mg once daily
b) 500 mg twice daily
c) 10 mg once weekly
d) 1 mg monthly injection
Answer: a) 120 mg once daily
- Which hormone is the main driver of testicular testosterone production?
a) Luteinizing hormone
b) Prolactin
c) Thyroid-stimulating hormone
d) Oxytocin
Answer: a) Luteinizing hormone
- Which adverse effect is common with Orgovyx?
a) Hot flushes
b) Severe hypoglycemia
c) Ototoxicity
d) Gingival hyperplasia
Answer: a) Hot flushes
- Which ECG-related warning is important with Orgovyx?
a) QT/QTc interval prolongation
b) Complete protection from arrhythmia
c) Mandatory atrial fibrillation in every patient
d) Shortened PR interval only
Answer: a) QT/QTc interval prolongation
- Which transporter interaction is important for relugolix?
a) P-glycoprotein
b) Dopamine transporter only
c) Sodium-glucose cotransporter only
d) Serotonin transporter only
Answer: a) P-glycoprotein
- Orgovyx can cause fetal harm mainly because it:
a) Alters reproductive hormone signaling
b) Acts as a folic acid supplement
c) Stimulates fetal growth directly
d) Is a local anesthetic
Answer: a) Alters reproductive hormone signaling
- Which statement best describes Orgovyx?
a) It competitively blocks pituitary GnRH receptors and rapidly lowers testosterone
b) It blocks androgen receptors directly in prostate cancer cells only
c) It inhibits bacterial cell wall synthesis
d) It stimulates soluble guanylate cyclase
Answer: a) It competitively blocks pituitary GnRH receptors and rapidly lowers testosterone
FAQs
What is the mechanism of action of Orgovyx?
Orgovyx, or relugolix, competitively blocks GnRH receptors in the anterior pituitary gland. This reduces LH and FSH secretion, lowers testicular testosterone production, and decreases androgen receptor stimulation in prostate cancer cells.
What is the generic name of Orgovyx?
The generic name of Orgovyx is relugolix.
Is Orgovyx a GnRH agonist or antagonist?
Orgovyx is a GnRH receptor antagonist. It directly blocks GnRH receptors and does not cause the initial testosterone flare seen with GnRH agonists such as leuprolide.
What is Orgovyx used for?
Orgovyx is used for the treatment of adult patients with advanced prostate cancer.
Does Orgovyx lower testosterone?
Yes. Orgovyx lowers testosterone by blocking pituitary GnRH receptors, reducing LH release, and decreasing testicular testosterone production.
How is Orgovyx taken?
Orgovyx is taken orally. Treatment starts with a 360 mg loading dose on Day 1, followed by 120 mg once daily at approximately the same time each day.
What are common adverse effects of Orgovyx?
Common adverse effects include hot flushes, increased glucose, increased triglycerides, musculoskeletal pain, decreased hemoglobin, increased liver enzymes, fatigue, constipation, and diarrhea.
How is Orgovyx different from leuprolide?
Orgovyx is an oral GnRH antagonist that blocks GnRH receptors directly. Leuprolide is an injectable GnRH agonist that initially stimulates GnRH receptors and can cause a temporary testosterone flare before suppression.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

