
Table of Contents
Introduction
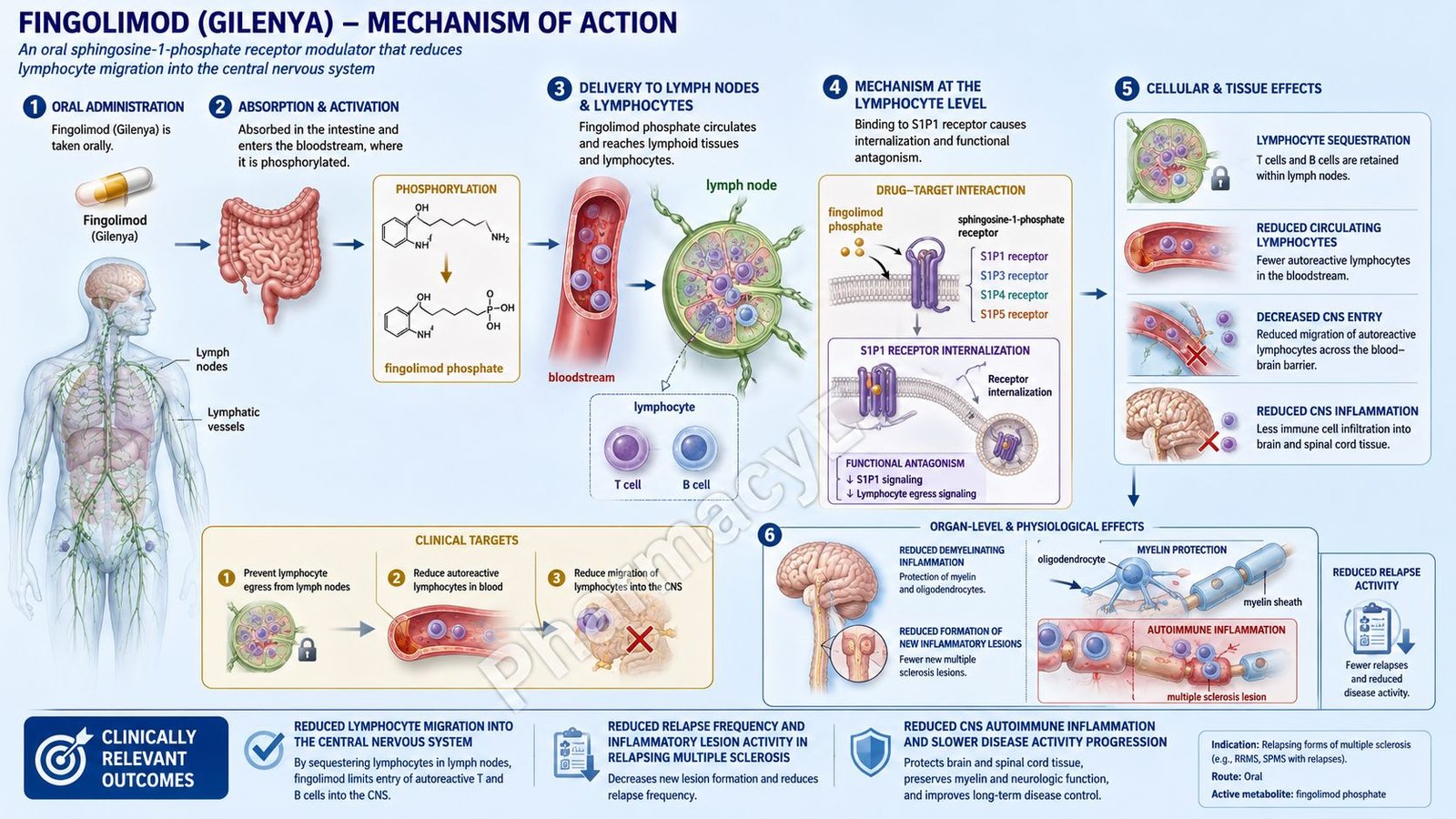
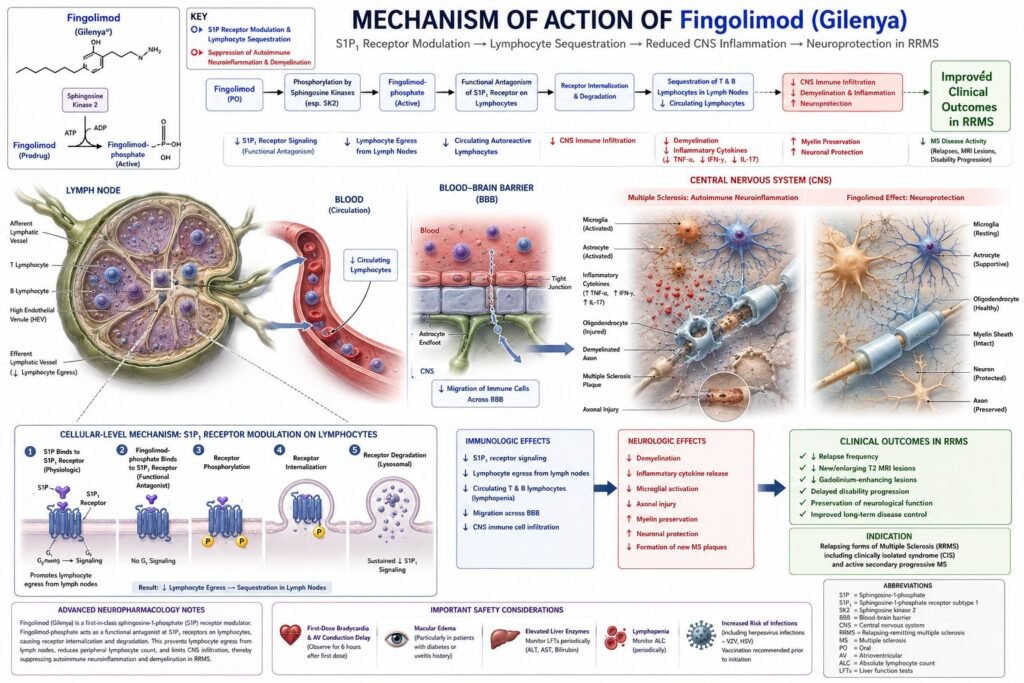
Fingolimod is an oral disease-modifying drug used in relapsing forms of multiple sclerosis. It was originally marketed under the brand name Gilenya. Pharmacologically, fingolimod is a sphingosine 1-phosphate receptor modulator, commonly called an S1P receptor modulator.
Multiple sclerosis is an immune-mediated demyelinating disease of the central nervous system. In MS, autoreactive lymphocytes cross the blood-brain barrier and attack myelin, oligodendrocytes, and axons. This leads to inflammation, demyelinating plaques, neurological relapses, and gradual accumulation of disability in some patients.
Fingolimod works after conversion to its active metabolite, fingolimod-phosphate. This active form binds to sphingosine 1-phosphate receptors, especially S1P receptor 1 on lymphocytes. By functionally blocking S1P1 signaling, fingolimod prevents lymphocytes from leaving lymph nodes. As a result, fewer autoreactive lymphocytes enter the blood and reach the central nervous system.
The exact therapeutic mechanism in multiple sclerosis is not completely established, but the key exam concept is lymphocyte sequestration in lymphoid tissues. Fingolimod does not directly repair myelin, does not act like a corticosteroid, and does not directly destroy B cells. It reduces immune-cell trafficking into the CNS.
Fingolimod is indicated for relapsing forms of multiple sclerosis, including clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in patients 10 years of age and older.
Mechanism of Action (Step-wise)
Step 1: Multiple sclerosis involves autoreactive lymphocytes
In multiple sclerosis, autoreactive T cells and B cells contribute to inflammation in the central nervous system. These immune cells can recognize CNS antigens and participate in immune-mediated damage to myelin and axons.
Step 2: Lymphocytes normally circulate between lymph nodes and blood
Lymphocytes are constantly moving between lymphoid organs, blood, and tissues. After lymphocytes enter lymph nodes, they usually need specific exit signals to leave the lymph node and return to the circulation.
Step 3: Sphingosine 1-phosphate guides lymphocyte exit
Sphingosine 1-phosphate, or S1P, is a lipid signaling molecule present in higher concentration in blood and lymph than in lymphoid tissues. Lymphocytes detect this gradient through S1P receptors, especially S1P receptor 1. This helps lymphocytes exit lymph nodes.
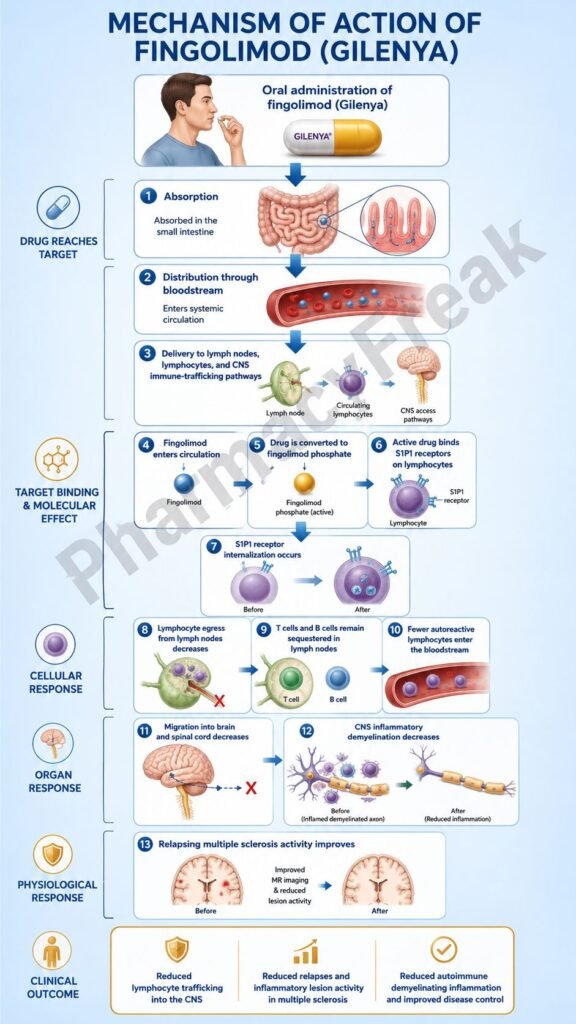
Step 4: Fingolimod is converted to fingolimod-phosphate
Fingolimod itself is a prodrug-like molecule. After oral administration, it is phosphorylated mainly by sphingosine kinase to form fingolimod-phosphate, the active metabolite. Fingolimod-phosphate is structurally similar to sphingosine 1-phosphate.
Step 5: Fingolimod-phosphate binds S1P receptors
Fingolimod-phosphate binds to S1P receptors, including S1P1, S1P3, S1P4, and S1P5. The most important receptor for MS pharmacology is S1P1 on lymphocytes.
Step 6: S1P1 receptors become functionally antagonized
Although fingolimod-phosphate initially acts as an agonist at S1P receptors, it causes internalization and degradation of S1P1 receptors on lymphocytes. This produces functional antagonism because lymphocytes can no longer properly respond to S1P gradients.
Step 7: Lymphocyte egress from lymph nodes decreases
When S1P1 signaling is reduced, lymphocytes become trapped inside lymph nodes. They cannot efficiently exit into blood. This lowers the number of circulating lymphocytes available to enter the CNS.
Step 8: CNS entry of autoreactive lymphocytes decreases
With fewer autoreactive lymphocytes in circulation, fewer immune cells cross the blood-brain barrier. This reduces CNS inflammation and demyelinating lesion formation.
Step 9: Relapse activity decreases
Reduced CNS immune-cell infiltration decreases inflammatory attacks in relapsing MS. Clinically, this helps reduce relapse frequency and new inflammatory MRI lesions.
Step 10: Fingolimod may also affect CNS S1P receptors
S1P receptors are also found on CNS cells such as astrocytes, oligodendrocytes, neurons, and microglia. Fingolimod may have additional CNS-related effects, but the main clinically accepted mechanism remains reduction of lymphocyte migration into the CNS.
Step 11: Immune surveillance is reduced
Because fingolimod reduces circulating lymphocytes, immune surveillance against infections and some malignancies may decrease. This explains important adverse effects such as infections, herpes viral complications, and skin cancer warnings.
Step 12: Stopping fingolimod may cause rebound disease activity
After fingolimod is discontinued, lymphocytes can gradually return to circulation. In some patients, severe increase in MS disability and disease activity has been reported after stopping fingolimod. This is an important exam and clinical safety point.
Step 13: Final therapeutic outcome
The final therapeutic effect is reduction of inflammatory immune-cell trafficking into the CNS, decreased relapse activity, fewer new demyelinating lesions, and better disease control in relapsing forms of MS.
Pharmacokinetics
Fingolimod is administered orally as capsules. The usual adult dose and pediatric dose for patients weighing more than 40 kg is 0.5 mg once daily. For pediatric patients 10 years and older weighing 40 kg or less, the recommended dose is 0.25 mg once daily. It may be taken with or without food.
After oral administration, fingolimod is slowly absorbed. Its oral bioavailability is high, and food does not meaningfully affect exposure. Because of its long pharmacokinetic profile, fingolimod is suitable for once-daily dosing.
Fingolimod is phosphorylated to fingolimod-phosphate, the pharmacologically active metabolite. This active metabolite is responsible for S1P receptor modulation.
Fingolimod and fingolimod-phosphate are highly protein bound. Fingolimod also distributes extensively into red blood cells, while fingolimod-phosphate has less red blood cell distribution.
Metabolism occurs through reversible phosphorylation and dephosphorylation, as well as oxidative metabolism involving CYP4F2 and other CYP enzymes. Because metabolism is not limited to one pathway, drug interactions are more nuanced than simple CYP3A4-only drugs.
The terminal half-life of fingolimod is long, approximately 6 to 9 days. This explains why its immunological effects continue after stopping therapy. Immune effects may persist for up to about 2 months after discontinuation, which matters for infection risk, vaccination planning, pregnancy planning, and switching to another immunosuppressive therapy.
Fingolimod can cause first-dose bradycardia and atrioventricular conduction delay. For this reason, first-dose observation with pulse and blood pressure monitoring is required, and ECG assessment is used in appropriate patients. Some patients require extended or overnight monitoring depending on cardiac risk factors and concomitant medications.
Before treatment, important baseline assessments include complete blood count, liver function tests, ophthalmic evaluation in selected patients, varicella zoster virus immunity assessment when appropriate, medication review for cardiac conduction effects, and vaccination review.
Clinical Uses
Fingolimod is used for relapsing forms of multiple sclerosis in patients 10 years of age and older. These include clinically isolated syndrome, relapsing-remitting multiple sclerosis, and active secondary progressive multiple sclerosis.
Clinically isolated syndrome refers to a first neurological episode suggestive of demyelination. Treatment may be considered when clinical and imaging findings indicate high risk of future MS activity.
Relapsing-remitting MS is characterized by acute relapses followed by partial or complete recovery. Fingolimod reduces relapse frequency by limiting lymphocyte movement from lymph nodes into the CNS.
Active secondary progressive MS refers to progressive disability with ongoing inflammatory activity, such as relapses or new MRI lesions. Fingolimod is used only when disease activity fits the relapsing MS indication.
Fingolimod is not approved for primary progressive multiple sclerosis. It is also not used as emergency treatment for acute MS relapse. Acute relapses are usually treated with high-dose corticosteroids or other specialist-directed interventions.
Fingolimod is not a steroid, interferon, monoclonal antibody, or B-cell-depleting therapy. It is an oral S1P receptor modulator that changes lymphocyte trafficking.
Adverse Effects
The most important adverse effects of fingolimod are related to cardiac effects, infection risk, macular edema, liver injury, respiratory effects, malignancy risk, fetal risk, and possible severe disease worsening after discontinuation.
First-dose bradycardia is a major warning. Fingolimod can decrease heart rate after the first dose and may cause atrioventricular conduction delay. The heart-rate effect usually begins within hours after dosing. Patients require first-dose monitoring, and those with higher cardiac risk may require overnight monitoring.
Serious infections can occur because fingolimod reduces circulating lymphocytes. Viral infections, including herpes virus infections, are important. Before starting therapy, patients without evidence of varicella zoster virus immunity should generally be vaccinated before treatment according to prescribing guidance.
Progressive multifocal leukoencephalopathy, or PML, has been reported with fingolimod. PML is a rare but serious JC virus-related brain infection. Symptoms may include progressive weakness, visual changes, cognitive decline, personality change, clumsiness, or speech difficulty.
Macular edema is an important adverse effect. It can occur with or without visual symptoms and is more likely in patients with diabetes or a history of uveitis. Symptoms include blurred vision, shadows, blind spots, or changes in central vision.
Liver injury can occur. Fingolimod may increase liver transaminases, and clinically significant liver injury has been reported. Liver function should be checked before treatment and monitored during therapy. Symptoms such as jaundice, dark urine, fatigue, nausea, vomiting, or right upper abdominal pain require evaluation.
Respiratory effects may occur because S1P receptors are involved in airway and vascular biology. Fingolimod can reduce forced expiratory volume and diffusion capacity in some patients. Patients with respiratory disease should be monitored clinically.
Hypertension may occur during treatment. Blood pressure should be monitored because fingolimod can increase blood pressure over time.
Skin malignancies are important safety concerns. Basal cell carcinoma, melanoma, and squamous cell carcinoma have been reported with fingolimod. Skin examination is recommended before or shortly after treatment initiation and periodically thereafter.
Posterior reversible encephalopathy syndrome, or PRES, has been reported rarely. Symptoms may include sudden severe headache, confusion, seizures, visual disturbance, or neurological deficits.
Fingolimod can cause fetal harm. Pregnancy should be avoided during treatment, and effective contraception is recommended during therapy and for 2 months after stopping because the drug remains in the body for a prolonged period.
Live vaccines should generally be avoided during fingolimod therapy and for 2 months after discontinuation because the immune response is reduced and vaccine infection risk may increase.
Severe increase in disability after stopping fingolimod has been reported. Patients should not discontinue therapy without medical supervision, and clinicians should monitor for rebound disease activity after discontinuation.
Comparative Analysis
Fingolimod is commonly compared with other S1P receptor modulators such as siponimod, ozanimod, and ponesimod.
Compared with siponimod, fingolimod is less selective. Fingolimod-phosphate interacts with S1P1, S1P3, S1P4, and S1P5, while siponimod is more selective for S1P1 and S1P5. Siponimod also requires CYP2C9 genotype consideration, while fingolimod does not require CYP2C9 genotyping.
Compared with ozanimod, fingolimod has stronger emphasis on first-dose cardiac monitoring in labeling. Ozanimod is more selective for S1P1 and S1P5 and is also used in ulcerative colitis, while fingolimod is used in relapsing MS.
Compared with ponesimod, fingolimod has a longer half-life and more prolonged immune effects after discontinuation. Ponesimod has a faster reversibility profile, while fingolimod effects may persist for weeks.
Compared with natalizumab, fingolimod reduces lymphocyte exit from lymph nodes, while natalizumab blocks alpha-4 integrin and prevents immune-cell adhesion and migration across the blood-brain barrier. Both reduce CNS immune-cell entry but act at different points in immune trafficking.
Compared with interferon beta, fingolimod is an oral immune-trafficking modulator, while interferon beta is an injectable immunomodulator with broad cytokine effects. Fingolimod is generally considered more potent but has more complex cardiac, ophthalmic, infection, and malignancy monitoring issues.
Compared with glatiramer acetate, fingolimod has a more defined lymphocyte-sequestration mechanism. Glatiramer acetate modulates immune responses to myelin-related antigens but does not primarily trap lymphocytes in lymph nodes.
Compared with anti-CD20 drugs such as ocrelizumab, ofatumumab, and rituximab, fingolimod does not deplete B cells directly. Anti-CD20 drugs remove CD20-positive B lymphocytes, while fingolimod retains lymphocytes in lymphoid tissues by altering S1P signaling.
Compared with cladribine, fingolimod causes reversible redistribution of lymphocytes rather than direct lymphocyte depletion through DNA damage. Cladribine is an immune reconstitution therapy, while fingolimod is continuous daily therapy.
MCQs
- Fingolimod belongs to which pharmacological class?
a) Sphingosine 1-phosphate receptor modulator
b) CD20 monoclonal antibody
c) Interferon beta analogue
d) Acetylcholinesterase inhibitor
Answer: a) Sphingosine 1-phosphate receptor modulator
- The original brand name of fingolimod is:
a) Gilenya
b) Tysabri
c) Ocrevus
d) Aubagio
Answer: a) Gilenya
- Fingolimod is mainly used for:
a) Relapsing forms of multiple sclerosis
b) Parkinson’s disease
c) Myasthenia gravis crisis
d) Acute bacterial meningitis
Answer: a) Relapsing forms of multiple sclerosis
- Fingolimod is converted to its active metabolite by:
a) Phosphorylation
b) Acetylation only
c) Glucuronidation only
d) Decarboxylation only
Answer: a) Phosphorylation
- The active metabolite of fingolimod is:
a) Fingolimod-phosphate
b) Fingolimod-glucuronide
c) Fingolimod-sulfate
d) Fingolimod-acetate
Answer: a) Fingolimod-phosphate
- Fingolimod primarily prevents lymphocytes from:
a) Exiting lymph nodes
b) Producing insulin
c) Binding acetylcholine receptors
d) Making red blood cells
Answer: a) Exiting lymph nodes
- The most important S1P receptor involved in lymphocyte egress is:
a) S1P1
b) Beta-1 receptor
c) Dopamine D2 receptor
d) Muscarinic M3 receptor
Answer: a) S1P1
- Fingolimod reduces MS activity mainly by:
a) Reducing lymphocyte trafficking into the CNS
b) Directly regenerating myelin in all lesions
c) Blocking acetylcholinesterase
d) Stimulating dopamine release
Answer: a) Reducing lymphocyte trafficking into the CNS
- Which monitoring is important after the first dose of fingolimod?
a) Heart rate and blood pressure monitoring
b) Serum uric acid only
c) Blood glucose every minute
d) Audiometry only
Answer: a) Heart rate and blood pressure monitoring
- Which eye-related adverse effect is associated with fingolimod?
a) Macular edema
b) Cataract cure
c) Retinal detachment in every patient
d) Permanent myopia reversal
Answer: a) Macular edema
- Which serious infection has been reported with fingolimod?
a) Progressive multifocal leukoencephalopathy
b) Acute tetanus in all patients
c) Mandatory malaria
d) Rabies reactivation only
Answer: a) Progressive multifocal leukoencephalopathy
- Which vaccine type should generally be avoided during fingolimod therapy?
a) Live vaccines
b) Inactivated influenza vaccine only
c) Recombinant vaccines only
d) Toxoid vaccines only
Answer: a) Live vaccines
- Fingolimod can cause which cardiovascular effect after initiation?
a) Bradycardia
b) Severe tachycardia in all patients
c) Complete heart protection
d) Permanent hypertension after first dose only
Answer: a) Bradycardia
- Which adverse effect is important to monitor with liver function tests?
a) Liver injury
b) Ototoxicity
c) Gingival hyperplasia
d) Hypoglycemic coma
Answer: a) Liver injury
- Which statement best describes fingolimod?
a) It functionally antagonizes S1P1 on lymphocytes and traps them in lymph nodes
b) It depletes CD20-positive B cells directly
c) It blocks IL-17A
d) It inhibits acetylcholinesterase
Answer: a) It functionally antagonizes S1P1 on lymphocytes and traps them in lymph nodes
FAQs
What is the mechanism of action of fingolimod?
Fingolimod is converted to fingolimod-phosphate, which modulates S1P receptors. It functionally blocks S1P1 on lymphocytes, preventing lymphocyte exit from lymph nodes and reducing autoreactive lymphocyte entry into the CNS.
What is the brand name of fingolimod?
The original brand name of fingolimod is Gilenya.
What is fingolimod used for?
Fingolimod is used for relapsing forms of multiple sclerosis, including clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in patients 10 years of age and older.
Is fingolimod an immunosuppressant?
Fingolimod has immunosuppressive effects because it reduces circulating lymphocytes. It does not destroy all immune cells, but it lowers immune-cell availability in blood and can increase infection risk.
Why does fingolimod cause bradycardia?
S1P receptors are also present in cardiac tissue. Fingolimod can affect cardiac conduction after the first dose, causing reduced heart rate and possible atrioventricular conduction delay.
Does fingolimod cure multiple sclerosis?
No. Fingolimod does not cure MS. It reduces relapse activity and inflammatory lesion formation by decreasing lymphocyte migration into the CNS.
Why is macular edema important with fingolimod?
Fingolimod can affect vascular permeability in the retina and may cause macular edema. Patients with diabetes or uveitis have higher risk and may need careful ophthalmic monitoring.
Can fingolimod be stopped suddenly?
Fingolimod should not be stopped without medical supervision. Severe increase in MS disability and rebound disease activity have been reported after discontinuation.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

