
Table of Contents
Introduction
Kesimpta is the brand name of ofatumumab, a subcutaneous monoclonal antibody used for relapsing forms of multiple sclerosis. Pharmacologically, Kesimpta is a CD20-directed cytolytic antibody. It is used in adults with relapsing forms of multiple sclerosis, including clinically isolated syndrome, relapsing-remitting multiple sclerosis, and active secondary progressive multiple sclerosis.
Multiple sclerosis is an immune-mediated demyelinating disorder of the central nervous system. In MS, immune cells attack myelin, oligodendrocytes, and axons, producing inflammation, demyelination, gliosis, and neurodegeneration. Although T cells are very important in MS pathology, B cells also play a major role by presenting antigen, producing inflammatory cytokines, forming ectopic lymphoid-like structures, and supporting autoreactive immune responses.
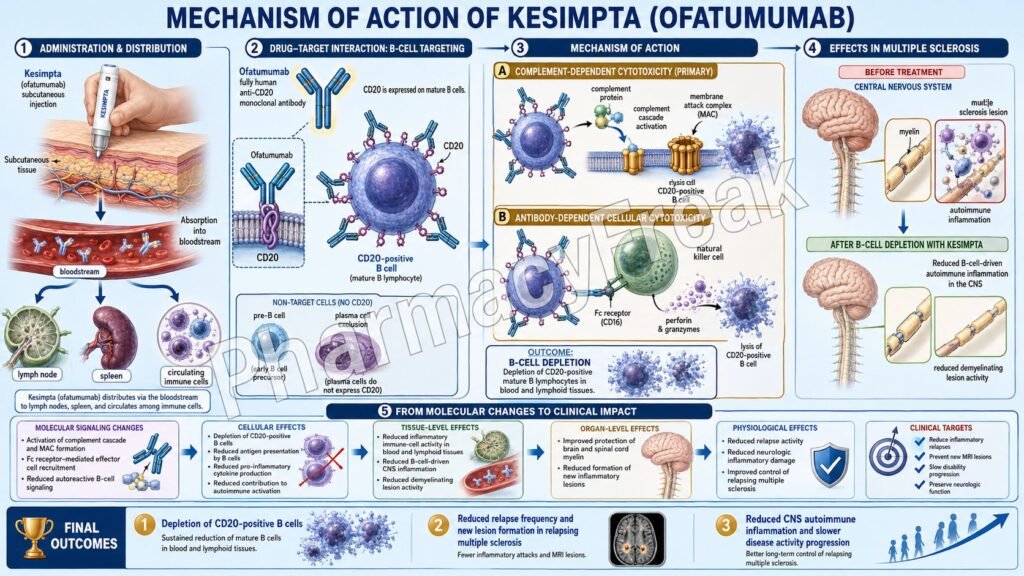
Kesimpta works by targeting CD20-positive B lymphocytes. CD20 is found mainly on pre-B cells, mature B cells, and memory B cells, but it is not present on stem cells or fully differentiated plasma cells. This allows ofatumumab to reduce pathogenic B-cell populations while preserving the ability of bone marrow stem cells to regenerate B cells over time.
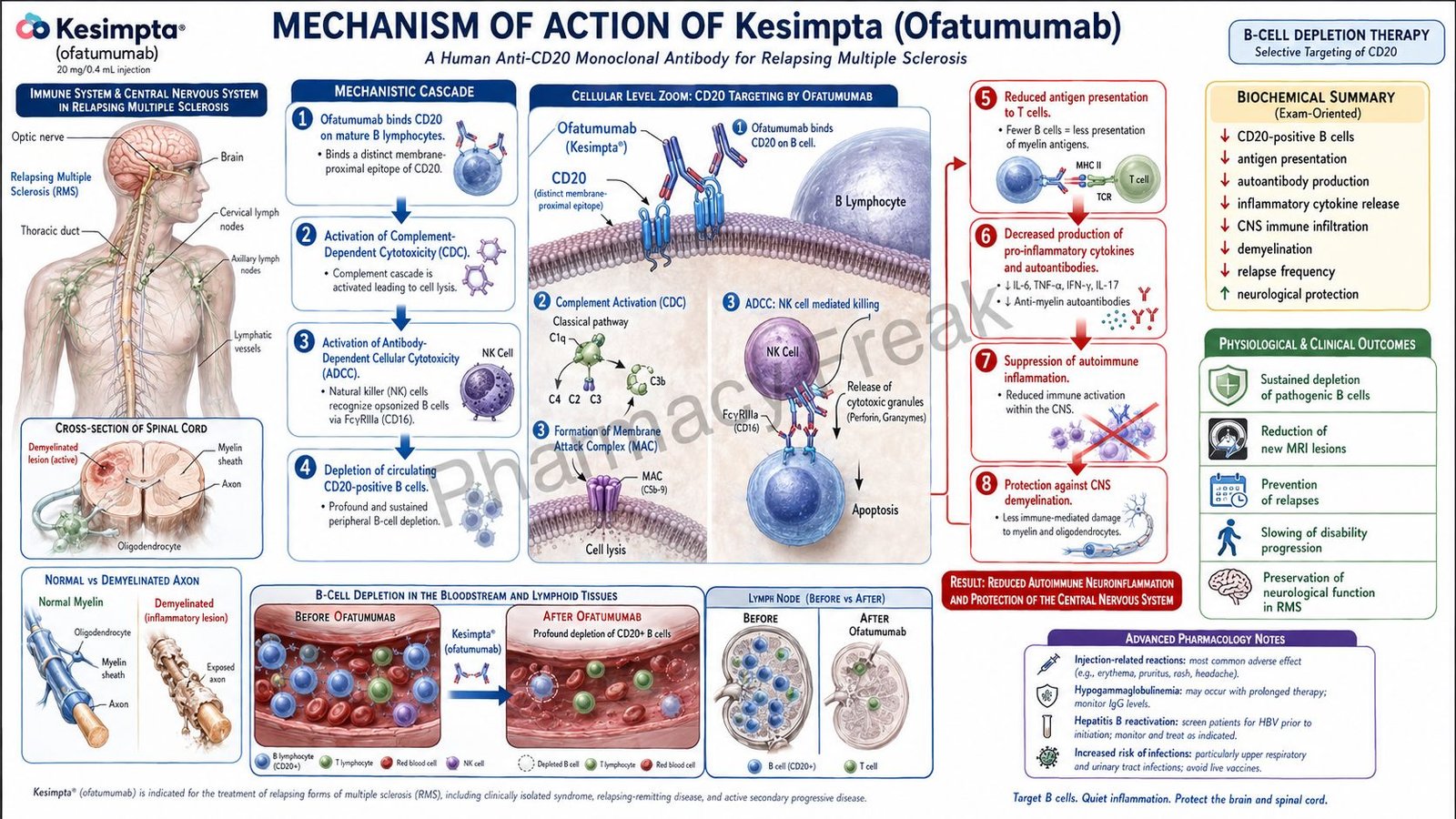
For exam purposes, Kesimpta should be remembered as a fully human anti-CD20 monoclonal antibody that binds CD20 on B cells and causes B-cell depletion through antibody-dependent cellular cytolysis and complement-mediated lysis. The exact therapeutic mechanism in multiple sclerosis is not fully established, but B-cell depletion is considered the key pharmacological action.
Mechanism of Action (Step-wise)
Step 1: Multiple sclerosis involves immune-mediated CNS injury
In multiple sclerosis, immune cells cross the blood-brain barrier and attack components of the central nervous system. This causes inflammatory plaques, demyelination, axonal injury, and neurological symptoms such as weakness, sensory disturbance, optic neuritis, coordination problems, fatigue, and cognitive dysfunction.
Step 2: B cells contribute to MS pathogenesis
B cells are not only antibody-producing cells. They also act as antigen-presenting cells, activate autoreactive T cells, release pro-inflammatory cytokines, and help maintain chronic inflammation. In MS, abnormal B-cell activity contributes to relapse formation and new inflammatory lesions.
Step 3: CD20 is expressed on selected B-cell stages
CD20 is a surface antigen present on pre-B lymphocytes, mature B lymphocytes, and memory B lymphocytes. It is not significantly expressed on early hematopoietic stem cells or most plasma cells. This is clinically important because anti-CD20 therapy can deplete many pathogenic B cells while allowing eventual B-cell reconstitution from precursor cells.
Step 4: Ofatumumab binds to CD20 on B lymphocytes
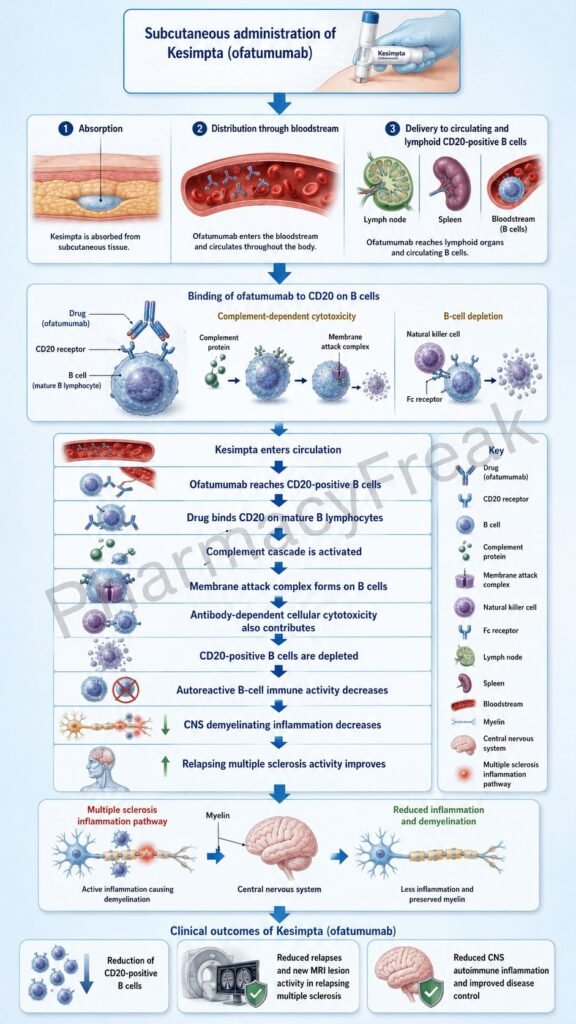
Ofatumumab is a recombinant human IgG1 monoclonal antibody that binds to human CD20 expressed on B cells. After binding to CD20, it marks the B cell for immune-mediated destruction. The official labeling describes the precise therapeutic mechanism in MS as unknown, but presumed to involve CD20 binding followed by antibody-dependent cellular cytolysis and complement-mediated lysis.
Step 5: Antibody-dependent cellular cytolysis occurs
After ofatumumab binds CD20, the Fc portion of the antibody can interact with Fc receptors on immune effector cells such as natural killer cells and macrophages. These effector cells then attack and destroy the antibody-coated B cell. This process is called antibody-dependent cellular cytolysis, or antibody-dependent cellular cytotoxicity.
Step 6: Complement-mediated lysis occurs
Ofatumumab binding can also activate the complement system on the B-cell surface. Complement activation leads to formation of the membrane attack complex, which damages the B-cell membrane and causes cell lysis. This is called complement-dependent cytotoxicity or complement-mediated lysis.
Step 7: Circulating CD20-positive B cells are depleted
The combined effect of antibody-dependent cellular cytolysis and complement-mediated lysis is depletion of CD20-positive B cells. In clinical monitoring, CD19-positive B-cell counts are commonly used because ofatumumab interferes with CD20-based assays. In trials, most treated patients had CD19-positive B-cell counts below the lower limit of normal within the early treatment period.
Step 8: Antigen presentation and inflammatory cytokine signaling decrease
With fewer pathogenic B cells available, antigen presentation to autoreactive T cells decreases. Pro-inflammatory cytokine production also decreases. This reduces immune activation against myelin and other CNS components.
Step 9: New inflammatory lesion formation is reduced
B-cell depletion reduces the immune processes that contribute to new demyelinating lesions. This helps reduce relapse activity and inflammatory disease activity on MRI.
Step 10: Relapse frequency decreases
The final therapeutic outcome is reduced relapse activity in relapsing forms of MS. Kesimpta does not cure MS or repair all existing CNS damage, but it reduces inflammatory disease activity and helps slow the accumulation of relapse-related neurological injury.
Step 11: B-cell repletion occurs after stopping therapy
After discontinuation, B-cell recovery occurs gradually. The label reports median B-cell recovery to the lower limit of normal or baseline value at about 24.6 weeks after treatment discontinuation. This delayed immune recovery is important for infection risk, vaccine planning, and treatment switching.
Pharmacokinetics
Kesimpta is administered by subcutaneous injection. The recommended dosing schedule is 20 mg at Weeks 0, 1, and 2, followed by 20 mg once monthly starting at Week 4. It is available as a single-dose Sensoready Pen or single-dose prefilled syringe containing 20 mg/0.4 mL.
Because Kesimpta is a monoclonal antibody, it is not given orally. If taken by mouth, it would be degraded in the gastrointestinal tract like other proteins. Subcutaneous administration allows gradual absorption into the systemic circulation, largely through the lymphatic system.
After repeated subcutaneous dosing, ofatumumab reaches a steady-state exposure suitable for sustained B-cell depletion. At steady state, the estimated half-life is approximately 16 days after repeated 20 mg subcutaneous dosing. This supports once-monthly maintenance dosing.
Ofatumumab is a large protein molecule and is not primarily metabolized by hepatic cytochrome P450 enzymes. Instead, it is expected to be degraded into small peptides and amino acids by proteolytic catabolic pathways. Therefore, classic CYP-based drug interactions are not a major concern.
Renal excretion of unchanged ofatumumab is not expected to be important because monoclonal antibodies are large molecules. Formal pharmacokinetic studies in renal or hepatic impairment have not been fully established, so clinical judgment is needed in patients with significant organ dysfunction.
Before starting Kesimpta, important baseline assessments include hepatitis B virus screening, quantitative serum immunoglobulins, vaccination review, and liver function tests. Live or live-attenuated vaccines should generally be completed at least 4 weeks before starting therapy, and non-live vaccines should be given at least 2 weeks before therapy whenever possible.
Clinical Uses
Kesimpta is used for relapsing forms of multiple sclerosis in adults. These include clinically isolated syndrome, relapsing-remitting multiple sclerosis, and active secondary progressive multiple sclerosis.
Clinically isolated syndrome refers to a first clinical episode suggestive of demyelination. Not every patient with clinically isolated syndrome has definite MS immediately, but high-risk patients may benefit from disease-modifying therapy to reduce future inflammatory activity.
Relapsing-remitting multiple sclerosis is the most common early pattern of MS. It is characterized by relapses followed by periods of partial or complete recovery. Kesimpta reduces relapse activity by depleting CD20-positive B cells involved in inflammatory disease activity.
Active secondary progressive multiple sclerosis refers to a later MS stage in which disability progression occurs, but inflammatory activity such as relapses or new MRI lesions is still present. Kesimpta is used only in active disease within its approved relapsing MS indication.
Kesimpta is not approved for primary progressive multiple sclerosis. It is also not established as safe or effective in pediatric patients. Its use requires infection screening, vaccination planning, and ongoing monitoring because B-cell depletion can increase infection risk.
Adverse Effects
The most important adverse effects of Kesimpta are related to immune suppression, injection reactions, and reduced immunoglobulin levels. Because it depletes B cells, patients may become more susceptible to infections.
Common adverse reactions include upper respiratory tract infections, headache, systemic injection-related reactions, local injection-site reactions, urinary tract infection, back pain, and decreased immunoglobulin M levels. Injection-related symptoms may include fever, headache, muscle pain, chills, and fatigue, especially after the first injection. Local injection-site reactions may include redness, swelling, itching, and pain.
Hepatitis B virus reactivation is a major safety concern. Kesimpta is contraindicated in patients with active HBV infection. HBV screening should be performed before treatment, and patients with evidence of prior HBV exposure require specialist evaluation and monitoring.
Progressive multifocal leukoencephalopathy, or PML, is a rare but serious brain infection caused by JC virus. PML has been reported with anti-CD20 therapies and related immunosuppressive treatments. Symptoms may include progressive weakness, visual disturbance, impaired coordination, confusion, personality change, or memory problems.
Reduction in immunoglobulins can occur, especially IgM. Quantitative immunoglobulin levels should be monitored at baseline, during treatment, and after discontinuation until B-cell repletion. Treatment discontinuation may be considered if serious opportunistic infection, recurrent infection, or prolonged hypogammaglobulinemia occurs.
A recent important label warning is liver injury. Clinically significant liver injury has been reported in the postmarketing setting with anti-CD20 B-cell-depleting therapies used for MS, including Kesimpta. Liver function tests should be obtained before treatment, and symptoms such as fatigue, anorexia, nausea, vomiting, right upper abdominal discomfort, dark urine, or jaundice should prompt evaluation.
Hypersensitivity reactions can occur, including anaphylaxis and angioedema. Kesimpta is contraindicated in patients with a history of hypersensitivity to ofatumumab or a life-threatening injection-related reaction to Kesimpta.
Fetal risk is also important. Based on animal data and the pharmacology of anti-CD20 therapy, ofatumumab may cause fetal B-cell depletion. Females of reproductive potential should use effective contraception during treatment and for 6 months after the last dose.
Comparative Analysis
Kesimpta is commonly compared with other MS disease-modifying therapies such as ocrelizumab, rituximab, ublituximab, natalizumab, fingolimod, siponimod, dimethyl fumarate, teriflunomide, interferon beta, glatiramer acetate, and cladribine.
Compared with ocrelizumab, Kesimpta also targets CD20-positive B cells. Ocrelizumab is given by intravenous infusion, while Kesimpta is given by subcutaneous self-injection after the first dose is performed under healthcare professional guidance. Both reduce B-cell-mediated inflammatory activity, but their dosing route and administration setting differ.
Compared with rituximab, ofatumumab is a fully human anti-CD20 antibody, while rituximab is a chimeric anti-CD20 antibody. Rituximab has been widely used off-label in MS in some settings, while Kesimpta has a formal approved relapsing MS indication.
Compared with ublituximab, another anti-CD20 monoclonal antibody for relapsing MS, Kesimpta differs mainly in formulation and route. Ublituximab is administered by intravenous infusion, while Kesimpta is administered subcutaneously.
Compared with natalizumab, Kesimpta targets B cells, while natalizumab blocks alpha-4 integrin and prevents immune-cell migration across the blood-brain barrier. Natalizumab is highly effective but has a well-known PML risk, especially in JC virus antibody-positive patients.
Compared with S1P receptor modulators such as fingolimod and siponimod, Kesimpta does not mainly trap lymphocytes in lymph nodes. S1P modulators prevent lymphocyte egress from lymphoid tissues, while Kesimpta depletes CD20-positive B cells.
Compared with cladribine, Kesimpta is a monoclonal antibody that selectively targets CD20-positive B cells. Cladribine is a purine nucleoside analogue that causes broader lymphocyte depletion through intracellular DNA damage and apoptosis.
Compared with interferon beta and glatiramer acetate, Kesimpta is generally considered a higher-efficacy disease-modifying therapy because it directly depletes pathogenic B-cell populations. However, higher efficacy comes with stronger infection-related monitoring requirements.
MCQs
- Kesimpta contains which active drug?
a) Ocrelizumab
b) Ofatumumab
c) Natalizumab
d) Alemtuzumab
Answer: b) Ofatumumab
- Kesimpta belongs to which pharmacological class?
a) CD20-directed cytolytic monoclonal antibody
b) S1P receptor modulator
c) Integrin receptor antagonist
d) Purine nucleoside analogue
Answer: a) CD20-directed cytolytic monoclonal antibody
- Kesimpta is mainly used for:
a) Primary progressive multiple sclerosis only
b) Relapsing forms of multiple sclerosis in adults
c) Acute bacterial meningitis
d) Parkinson’s disease tremor
Answer: b) Relapsing forms of multiple sclerosis in adults
- The main cellular target of Kesimpta is:
a) CD20-positive B lymphocytes
b) Dopamine neurons
c) Red blood cells
d) Platelet glycoprotein IIb/IIIa receptors
Answer: a) CD20-positive B lymphocytes
- CD20 is mainly present on:
a) Pre-B and mature B lymphocytes
b) Mature plasma cells only
c) Neutrophils only
d) Hepatocytes only
Answer: a) Pre-B and mature B lymphocytes
- The precise therapeutic mechanism of ofatumumab in MS is:
a) Fully explained only by direct myelin regeneration
b) Unknown, but presumed to involve CD20 binding and B-cell depletion
c) Due to direct dopamine receptor blockade
d) Due to irreversible COX inhibition
Answer: b) Unknown, but presumed to involve CD20 binding and B-cell depletion
- After binding CD20, ofatumumab causes B-cell destruction mainly through:
a) Antibody-dependent cellular cytolysis and complement-mediated lysis
b) Direct inhibition of DNA gyrase
c) Cyclooxygenase inhibition
d) Sodium channel blockade
Answer: a) Antibody-dependent cellular cytolysis and complement-mediated lysis
- Which marker is commonly used to monitor B-cell depletion with Kesimpta?
a) CD19-positive B-cell count
b) Serum potassium only
c) Hemoglobin A1c
d) Troponin I
Answer: a) CD19-positive B-cell count
- Kesimpta is administered by which route?
a) Subcutaneous injection
b) Oral tablet
c) Intranasal spray
d) Intrathecal injection
Answer: a) Subcutaneous injection
- The recommended maintenance dosing of Kesimpta after initial loading is:
a) 20 mg once monthly
b) 500 mg daily orally
c) 1 g intravenously every week
d) 10 mg every 6 months only
Answer: a) 20 mg once monthly
- Which infection must be screened for before starting Kesimpta?
a) Hepatitis B virus
b) Malaria only
c) H. pylori only
d) Dermatophyte infection only
Answer: a) Hepatitis B virus
- Which serious CNS infection is an important warning with anti-CD20 therapy?
a) Progressive multifocal leukoencephalopathy
b) Migraine aura
c) Benign positional vertigo
d) Essential tremor
Answer: a) Progressive multifocal leukoencephalopathy
- Which immunoglobulin abnormality is especially noted with Kesimpta?
a) Decreased IgM
b) Increased IgE only
c) Increased IgA in all patients
d) Complete absence of albumin
Answer: a) Decreased IgM
- Which adverse reaction commonly occurs after the first Kesimpta injection?
a) Injection-related reaction
b) Severe hypoglycemia
c) Irreversible hearing loss
d) Gingival hyperplasia
Answer: a) Injection-related reaction
- Which statement correctly compares Kesimpta with ocrelizumab?
a) Both target CD20-positive B cells, but Kesimpta is subcutaneous and ocrelizumab is intravenous
b) Kesimpta blocks S1P receptors, while ocrelizumab blocks dopamine receptors
c) Both are oral tablets
d) Ocrelizumab is an antibiotic, while Kesimpta is an NSAID
Answer: a) Both target CD20-positive B cells, but Kesimpta is subcutaneous and ocrelizumab is intravenous
FAQs
What is the mechanism of action of Kesimpta?
Kesimpta, or ofatumumab, binds to CD20 on B lymphocytes and causes B-cell depletion through antibody-dependent cellular cytolysis and complement-mediated lysis. The exact therapeutic mechanism in multiple sclerosis is not fully established, but depletion of pathogenic B cells is considered the main pharmacological action.
What is the generic name of Kesimpta?
The generic name of Kesimpta is ofatumumab.
What is Kesimpta used for?
Kesimpta is used in adults with relapsing forms of multiple sclerosis, including clinically isolated syndrome, relapsing-remitting multiple sclerosis, and active secondary progressive multiple sclerosis.
Is Kesimpta used for primary progressive multiple sclerosis?
Kesimpta is not approved for primary progressive multiple sclerosis. Its approved use is for relapsing forms of MS in adults.
Why does Kesimpta target B cells in multiple sclerosis?
B cells contribute to MS by presenting antigen, activating T cells, producing inflammatory cytokines, and supporting CNS inflammation. Depleting CD20-positive B cells reduces these immune processes and lowers relapse activity.
What are the most important adverse effects of Kesimpta?
Important adverse effects include infections, injection-related reactions, injection-site reactions, reduced immunoglobulins, hepatitis B reactivation, possible PML, hypersensitivity reactions, liver injury, and fetal risk.
Why is hepatitis B screening needed before Kesimpta?
Kesimpta can reactivate hepatitis B infection because it suppresses B-cell immunity. Active HBV infection is a contraindication, and patients with prior HBV exposure require specialist evaluation and monitoring.
Can vaccines be given during Kesimpta therapy?
Live or live-attenuated vaccines are generally not recommended during treatment and until B-cell recovery. Required live vaccines should be given at least 4 weeks before starting therapy, and non-live vaccines should ideally be given at least 2 weeks before starting therapy.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

