
Table of Contents
Introduction
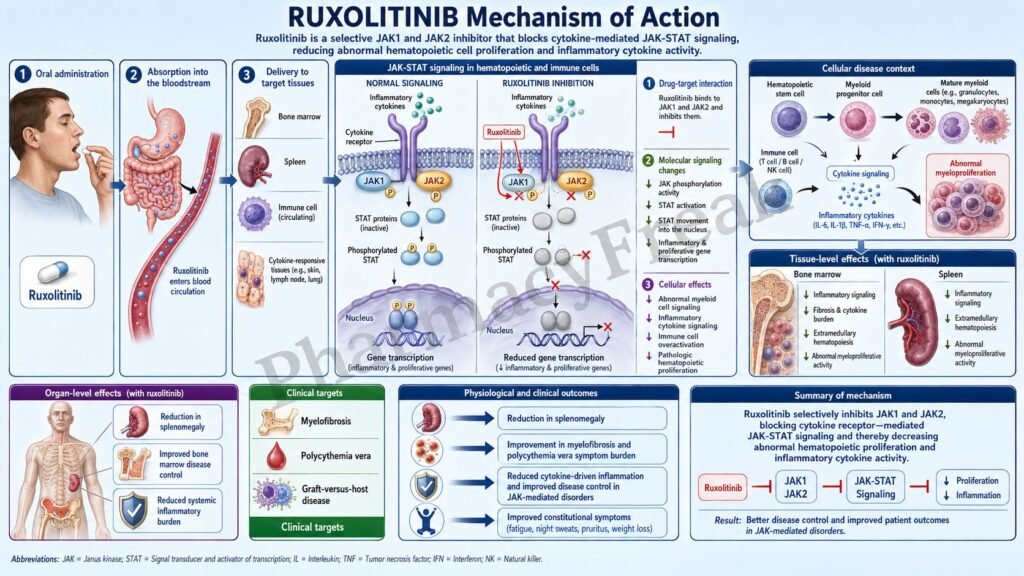
Ruxolitinib is an oral Janus kinase inhibitor used mainly in hematological and immune-mediated disorders. It is best known by the brand name Jakafi for systemic use, and it selectively inhibits Janus kinase 1 and Janus kinase 2, commonly called JAK1 and JAK2.
Ruxolitinib is important in pharmacology because JAK enzymes are central mediators of cytokine and growth factor signaling. These pathways regulate hematopoiesis, immune activation, inflammation, splenic enlargement, and abnormal myeloproliferative activity. In diseases such as myelofibrosis and polycythemia vera, dysregulated JAK-STAT signaling contributes to abnormal blood cell production, inflammatory cytokine release, constitutional symptoms, and splenomegaly.
Current prescribing information lists systemic ruxolitinib for intermediate or high-risk myelofibrosis in adults, polycythemia vera in adults with inadequate response or intolerance to hydroxyurea, steroid-refractory acute graft-versus-host disease in adults and pediatric patients 12 years and older, and chronic graft-versus-host disease after failure of one or two lines of systemic therapy in adults and pediatric patients 12 years and older.
For pharmacy, medical, nursing, and competitive exam students, ruxolitinib is an important example of targeted kinase inhibition. It does not work like conventional chemotherapy. Instead, it blocks intracellular JAK1/JAK2-mediated signaling, reduces STAT activation, decreases inflammatory cytokine signaling, and controls abnormal hematopoietic and immune activity.
Mechanism of Action (Step-wise)
- Primary target: JAK1 and JAK2
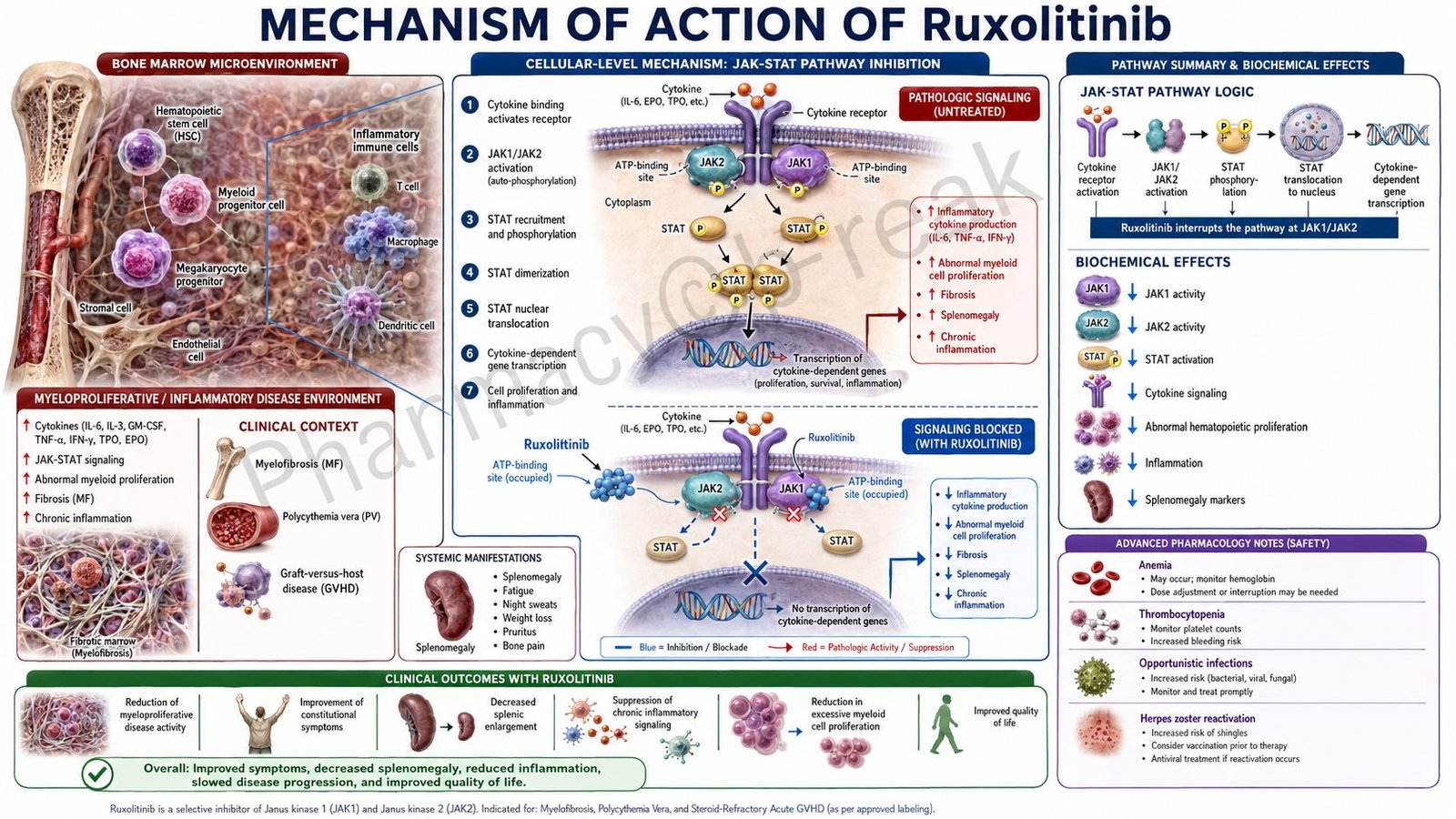
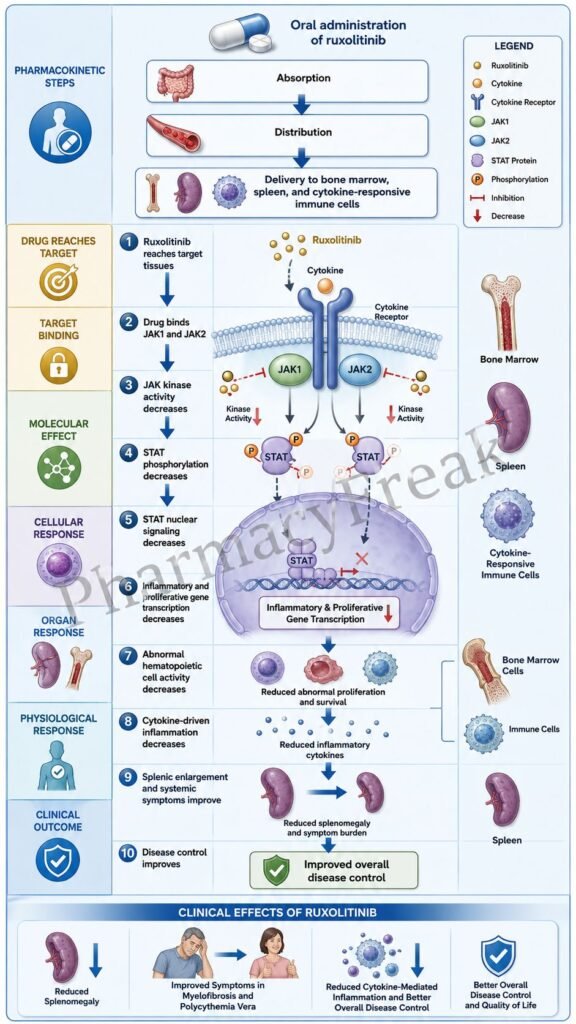
Ruxolitinib inhibits Janus-associated kinases JAK1 and JAK2. These enzymes are attached to cytokine receptors and growth factor receptors on the surface of hematopoietic and immune cells.
JAK1 and JAK2 help transmit signals from extracellular cytokines into the cell. These signals are important for immune regulation, inflammation, blood cell production, and growth factor responses. The official clinical pharmacology section describes ruxolitinib as a kinase inhibitor of JAK1 and JAK2, which mediate cytokine and growth factor signaling important for hematopoiesis and immune function.
- Cytokine receptor signaling is reduced
Normally, cytokines bind to their receptors on target cells. This causes receptor-associated JAK enzymes to become activated. Activated JAKs phosphorylate downstream proteins and amplify inflammatory and proliferative signaling.
By inhibiting JAK1 and JAK2, ruxolitinib reduces cytokine receptor-mediated signal transmission.
- STAT phosphorylation decreases
A key downstream effect of JAK activation is phosphorylation of STAT proteins. STAT stands for signal transducer and activator of transcription.
After phosphorylation, STAT proteins dimerize and move into the nucleus, where they regulate gene transcription. Ruxolitinib reduces cytokine-induced STAT phosphorylation, including STAT3 phosphorylation. In patients with myelofibrosis and polycythemia vera, maximal inhibition of STAT3 phosphorylation occurs about 2 hours after dosing and returns near baseline by about 10 hours.
- Reduced nuclear gene transcription
When STAT activation decreases, less phosphorylated STAT enters the nucleus. This reduces transcription of genes involved in inflammatory cytokine production, cell proliferation, survival, and immune activation.
This step is central to ruxolitinib’s therapeutic effect because many clinical features of myeloproliferative neoplasms and graft-versus-host disease are driven by excessive cytokine and JAK-STAT signaling.
- Effect in myelofibrosis and polycythemia vera
Myelofibrosis and polycythemia vera are myeloproliferative neoplasms associated with dysregulated JAK1 and JAK2 signaling. Some patients have JAK2V617F mutations, but ruxolitinib can be useful even when the disease biology involves broader pathway activation rather than only one mutation.
By blocking JAK1/JAK2 signaling, ruxolitinib reduces abnormal myeloproliferative signaling, decreases inflammatory cytokines such as TNF-alpha and IL-6, and helps reduce splenomegaly and systemic symptoms.
- Effect in graft-versus-host disease
In graft-versus-host disease, donor immune cells attack recipient tissues. JAK-STAT signaling contributes to immune cell activation, cytokine release, tissue infiltration, and inflammation.
Ruxolitinib reduces immune-cell activation and inflammatory cytokine signaling, helping control steroid-refractory acute GVHD and chronic GVHD after failure of systemic therapy. JAK-STAT pathways are specifically involved in the development, proliferation, and activation of immune cells important in GVHD pathogenesis.
- Final therapeutic effect
The final therapeutic effect of ruxolitinib is inhibition of JAK1/JAK2-mediated cytokine signaling, reduced STAT activation, decreased inflammatory cytokine production, reduced abnormal hematopoietic cell activity, decreased splenomegaly in myelofibrosis, improved hematocrit control in polycythemia vera, and reduced immune-mediated tissue injury in graft-versus-host disease.
Pharmacokinetics
Ruxolitinib is administered orally as immediate-release tablets and is also available as an extended-release oral formulation. Immediate-release ruxolitinib is generally given twice daily, while extended-release ruxolitinib is designed for once-daily dosing.
Absorption:
Ruxolitinib is rapidly absorbed after oral administration. Immediate-release ruxolitinib reaches peak plasma concentration within approximately 1 to 2 hours after dosing. Oral absorption is estimated to be at least 95%. Extended-release ruxolitinib reaches peak concentration at approximately 3 hours. Food does not produce clinically relevant changes in ruxolitinib pharmacokinetics.
Distribution:
Ruxolitinib is widely distributed, with a mean volume of distribution at steady state of about 72 L in patients with myelofibrosis and 75 L in patients with polycythemia vera. It is approximately 97% protein-bound, mainly to albumin.
Metabolism:
Ruxolitinib is metabolized mainly by CYP3A4 and to a lesser extent by CYP2C9. This is clinically important because strong CYP3A4 inhibitors, fluconazole, and CYP3A4 inducers can affect ruxolitinib exposure.
Excretion:
After a single radiolabeled oral dose, about 74% of radioactivity is excreted in urine and about 22% in feces. Less than 1% of the excreted radioactivity is unchanged drug, showing that metabolism is the major route before elimination.
Half-life and duration:
The mean elimination half-life of immediate-release ruxolitinib is approximately 3 hours, and the half-life of ruxolitinib plus metabolites is about 5.8 hours in healthy volunteers. Extended-release ruxolitinib has a mean elimination half-life of approximately 5 hours.
Special pharmacokinetic point:
Dose modification may be needed in renal impairment, hepatic impairment, and with interacting drugs. Complete blood count monitoring is important because ruxolitinib can cause anemia, thrombocytopenia, and neutropenia.
Clinical Uses
- Intermediate or high-risk myelofibrosis:
Ruxolitinib is used in adults with intermediate or high-risk myelofibrosis, including primary myelofibrosis, post-polycythemia vera myelofibrosis, and post-essential thrombocythemia myelofibrosis. It helps reduce splenomegaly and constitutional symptoms. - Polycythemia vera:
Ruxolitinib is used in adults with polycythemia vera who have had an inadequate response to hydroxyurea or who are intolerant of hydroxyurea. It helps control hematocrit and disease-related symptoms. - Steroid-refractory acute graft-versus-host disease:
Ruxolitinib is used in adults and pediatric patients 12 years and older with acute GVHD that has not responded adequately to corticosteroids. - Chronic graft-versus-host disease:
Ruxolitinib is used in adults and pediatric patients 12 years and older with chronic GVHD after failure of one or two lines of systemic therapy. - Inflammatory cytokine-driven disease control:
Because ruxolitinib suppresses JAK-STAT cytokine signaling, it is useful in conditions where abnormal cytokine signaling contributes to symptoms and tissue damage. - Topical dermatologic use:
Ruxolitinib is also available as a topical cream formulation for selected dermatologic conditions such as atopic dermatitis and nonsegmental vitiligo. However, this article mainly focuses on systemic ruxolitinib pharmacology.
Adverse Effects
Common adverse effects of systemic ruxolitinib include:
- Anemia
- Thrombocytopenia
- Neutropenia
- Bruising
- Dizziness
- Headache
- Diarrhea
- Fatigue
- Edema
- Increased liver enzymes
- Hypercholesterolemia
- Hypertriglyceridemia
- Infections
- Viral infections, including herpes zoster
Important serious adverse effects include:
- Severe anemia
- Severe thrombocytopenia
- Severe neutropenia
- Serious bacterial, viral, fungal, or opportunistic infections
- Tuberculosis reactivation
- Hepatitis B reactivation
- Progressive multifocal leukoencephalopathy, rarely
- Non-melanoma skin cancer
- Lipid elevations
- Major adverse cardiovascular events
- Thrombosis
- Secondary malignancies
- Symptom exacerbation after abrupt interruption or discontinuation
The prescribing information highlights thrombocytopenia, anemia, neutropenia, risk of infection, symptom exacerbation after interruption or discontinuation, non-melanoma skin cancer, lipid elevations, major adverse cardiovascular events, thrombosis, and secondary malignancies as important warnings and precautions.
Myelosuppression is one of the most exam-important adverse effects. Complete blood count monitoring is required before and during treatment. Dose interruption or dose reduction may be needed for cytopenias.
Infection risk is another major safety concern because JAK inhibition suppresses cytokine pathways involved in immune defense. Patients should be assessed for infection history, including tuberculosis, herpes infections, and hepatitis B, before treatment.
Abrupt discontinuation can lead to recurrence or worsening of disease symptoms. When possible, therapy should be tapered or carefully managed under medical supervision.
Comparative Analysis
| Feature | Ruxolitinib | Fedratinib | Pacritinib | Hydroxyurea |
|---|---|---|---|---|
| Drug class | JAK1/JAK2 inhibitor | JAK2 inhibitor | JAK2/IRAK1/ACVR1 inhibitor | Antimetabolite/cytoreductive agent |
| Main target | JAK1 and JAK2 | JAK2 | JAK2 and other kinases | Ribonucleotide reductase |
| Main pathway | JAK-STAT signaling | JAK-STAT signaling | JAK-STAT and inflammatory signaling | DNA synthesis inhibition |
| Main use | MF, PV, GVHD | Myelofibrosis | Myelofibrosis with thrombocytopenia | PV, essential thrombocythemia, sickle cell disease |
| Route | Oral | Oral | Oral | Oral |
| Key benefit | Reduces splenomegaly, symptoms, cytokine activity | Reduces spleen size and symptoms | Useful in selected thrombocytopenic MF patients | Reduces blood cell production |
| Major adverse effect | Cytopenias, infections, lipid elevation | GI toxicity, Wernicke encephalopathy warning | Diarrhea, thrombocytopenia, bleeding risk | Myelosuppression, ulcers, skin/nail changes |
| GVHD use | Yes | No routine use | No routine use | No routine use |
Ruxolitinib differs from hydroxyurea because it targets cytokine and growth factor signaling through JAK1/JAK2 rather than directly inhibiting DNA synthesis. Fedratinib and pacritinib are also JAK-pathway drugs used mainly in myelofibrosis, but they have different kinase selectivity and toxicity profiles. Ruxolitinib is especially notable because it is used not only in myeloproliferative neoplasms but also in graft-versus-host disease.
MCQs
- Ruxolitinib primarily inhibits which enzymes?
a) COX-1 and COX-2
b) JAK1 and JAK2
c) ACE and renin
d) CYP2D6 and CYP3A4
Answer: b) JAK1 and JAK2
- Ruxolitinib belongs to which drug class?
a) Antimetabolite
b) JAK inhibitor
c) Alkylating agent
d) Proteasome inhibitor
Answer: b) JAK inhibitor
- The major intracellular pathway affected by ruxolitinib is:
a) JAK-STAT pathway
b) GABA pathway
c) Cyclooxygenase pathway
d) Cholinergic pathway
Answer: a) JAK-STAT pathway
- Ruxolitinib decreases activation of which transcription factor family?
a) STAT proteins
b) GABA receptors
c) Histamine receptors
d) Insulin receptors
Answer: a) STAT proteins
- Which disease is commonly treated with ruxolitinib?
a) Myelofibrosis
b) Acute bacterial meningitis
c) Type 1 diabetes mellitus
d) Malaria
Answer: a) Myelofibrosis
- In polycythemia vera, ruxolitinib is used especially when patients are:
a) Resistant or intolerant to hydroxyurea
b) Newly diagnosed with mild iron deficiency
c) Allergic to penicillin
d) Hypoglycemic after insulin
Answer: a) Resistant or intolerant to hydroxyurea
- Ruxolitinib helps reduce splenomegaly mainly by:
a) Blocking abnormal JAK-STAT myeloproliferative signaling
b) Increasing platelet aggregation
c) Stimulating erythropoietin release
d) Blocking bacterial ribosomes
Answer: a) Blocking abnormal JAK-STAT myeloproliferative signaling
- Which adverse effect is especially important with ruxolitinib?
a) Anemia and thrombocytopenia
b) Severe ototoxicity
c) Gingival hyperplasia
d) Hypocalcemia only
Answer: a) Anemia and thrombocytopenia
- Which infection risk is relevant during ruxolitinib therapy?
a) Herpes zoster and opportunistic infections
b) Only common cold without any serious risk
c) No infection risk at all
d) Only fungal nail infection
Answer: a) Herpes zoster and opportunistic infections
- Ruxolitinib is metabolized mainly by:
a) CYP3A4
b) Acetylcholinesterase
c) Monoamine oxidase-B
d) Xanthine oxidase only
Answer: a) CYP3A4
- Ruxolitinib is used in graft-versus-host disease because it:
a) Reduces immune-cell activation and cytokine signaling
b) Directly kills bacteria
c) Increases gastric acid secretion
d) Blocks insulin receptors
Answer: a) Reduces immune-cell activation and cytokine signaling
- Which monitoring is important during ruxolitinib therapy?
a) Complete blood count
b) Blood group only
c) Serum calcium only
d) Visual acuity only
Answer: a) Complete blood count
- Which cytokine-related effect is reduced by ruxolitinib?
a) Inflammatory cytokine signaling
b) Insulin secretion only
c) Thyroxine release only
d) Histamine degradation only
Answer: a) Inflammatory cytokine signaling
- Ruxolitinib differs from hydroxyurea because hydroxyurea mainly:
a) Inhibits DNA synthesis through ribonucleotide reductase inhibition
b) Blocks JAK1 and JAK2 selectively
c) Activates STAT proteins
d) Stimulates megakaryocyte growth
Answer: a) Inhibits DNA synthesis through ribonucleotide reductase inhibition
- Which statement about ruxolitinib is correct?
a) It inhibits JAK1/JAK2 and reduces STAT-mediated gene transcription
b) It is a beta-lactam antibiotic
c) It directly replaces insulin
d) It is a rescue bronchodilator
Answer: a) It inhibits JAK1/JAK2 and reduces STAT-mediated gene transcription
FAQs
- What is ruxolitinib used for?
Ruxolitinib is used for intermediate or high-risk myelofibrosis, polycythemia vera after inadequate response or intolerance to hydroxyurea, steroid-refractory acute graft-versus-host disease, and chronic graft-versus-host disease after failure of systemic therapy.
- What is the mechanism of action of ruxolitinib?
Ruxolitinib inhibits JAK1 and JAK2. This reduces cytokine receptor signaling, decreases STAT phosphorylation, reduces STAT-mediated gene transcription, and suppresses abnormal inflammatory, immune, and myeloproliferative signaling.
- Is ruxolitinib chemotherapy?
Ruxolitinib is not traditional cytotoxic chemotherapy. It is a targeted kinase inhibitor that blocks JAK1/JAK2 signaling pathways.
- Why does ruxolitinib reduce spleen size in myelofibrosis?
In myelofibrosis, dysregulated JAK-STAT signaling contributes to abnormal hematopoiesis and splenomegaly. By inhibiting JAK1/JAK2 signaling, ruxolitinib reduces myeloproliferative and inflammatory activity, which can decrease spleen size.
- Does ruxolitinib cure myelofibrosis?
Ruxolitinib does not usually cure myelofibrosis. It helps control symptoms, reduce spleen size, and improve disease-related inflammatory features.
- Why does ruxolitinib cause anemia and thrombocytopenia?
JAK2 signaling is involved in normal hematopoiesis. Inhibition of JAK2 can suppress blood cell production, leading to anemia, thrombocytopenia, or neutropenia.
- Can ruxolitinib increase infection risk?
Yes. Ruxolitinib can increase the risk of infections because JAK signaling is important for immune function. Serious bacterial, viral, fungal, and opportunistic infections may occur.
- Why should ruxolitinib not be stopped suddenly?
Abrupt interruption or discontinuation can cause return or worsening of disease symptoms. Discontinuation should be managed carefully under medical supervision.
- Which enzyme metabolizes ruxolitinib?
Ruxolitinib is mainly metabolized by CYP3A4 and to a lesser extent by CYP2C9. Drug interactions with CYP3A4 inhibitors or inducers are clinically important.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

