
Table of Contents
Introduction
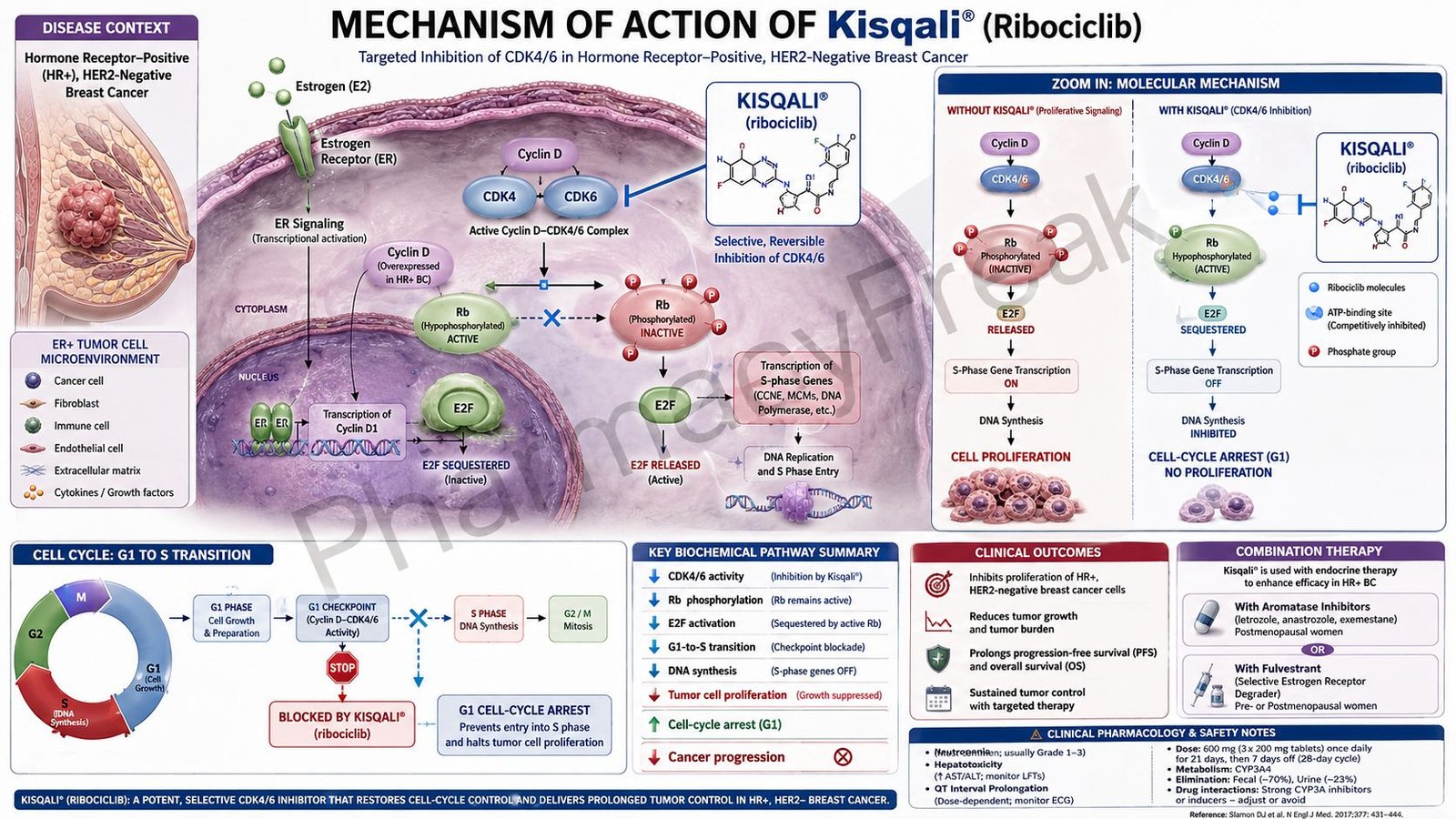
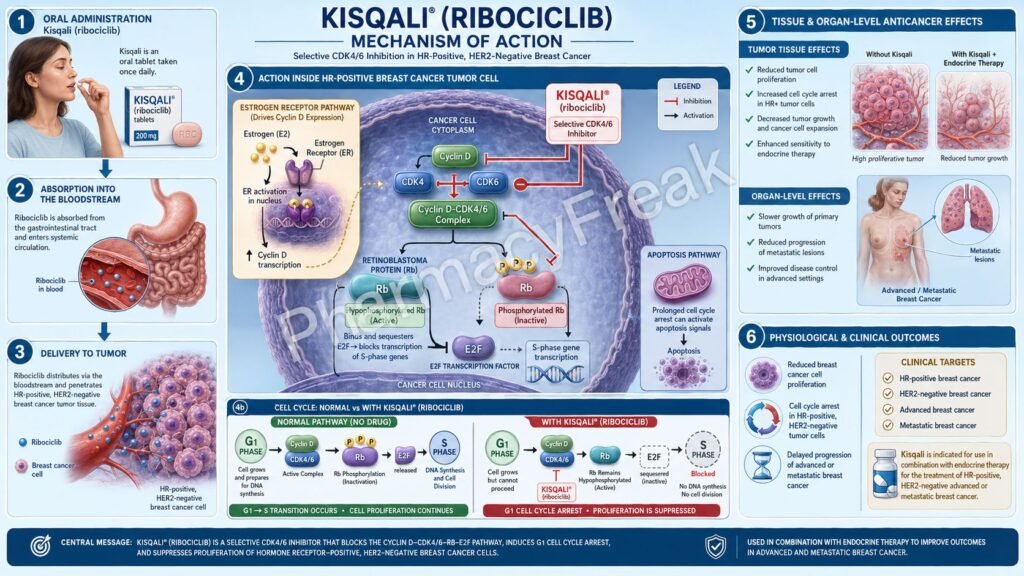
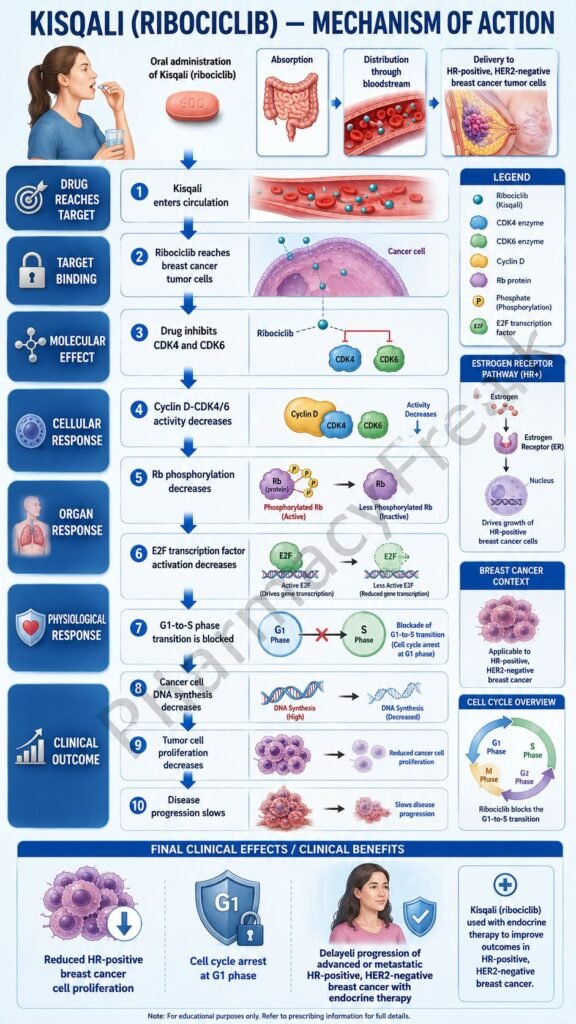
Kisqali is the brand name of ribociclib, an oral targeted anticancer drug used in hormone receptor-positive, HER2-negative breast cancer. It belongs to the class of cyclin-dependent kinase 4 and 6 inhibitors, commonly called CDK4/6 inhibitors.
Kisqali is important in oncology pharmacology because it targets the cell cycle machinery that allows cancer cells to divide and proliferate. In hormone receptor-positive breast cancer, estrogen receptor signaling promotes cyclin D production, which activates CDK4 and CDK6. These kinases drive the cell from the G1 phase into the S phase of the cell cycle. By blocking CDK4/6, ribociclib prevents uncontrolled cell-cycle progression and slows tumor growth.
Current prescribing information lists Kisqali in combination with an aromatase inhibitor for adjuvant treatment of adults with HR-positive, HER2-negative stage II and III early breast cancer at high risk of recurrence. It is also indicated in adults with HR-positive, HER2-negative advanced or metastatic breast cancer in combination with an aromatase inhibitor as initial endocrine-based therapy, or with fulvestrant as initial therapy or after progression on endocrine therapy.
For pharmacy, medical, nursing, and competitive exam students, Kisqali is an important example of targeted cancer therapy. It is not traditional cytotoxic chemotherapy. Instead, it selectively blocks CDK4/6-mediated phosphorylation of retinoblastoma protein, causing G1 phase cell-cycle arrest and reduced cancer cell proliferation.
Mechanism of Action (Step-wise)
- Kisqali inhibits CDK4 and CDK6
Kisqali contains ribociclib, which inhibits cyclin-dependent kinases 4 and 6. CDK4 and CDK6 are enzymes that regulate cell-cycle progression. They become active after binding to cyclin D proteins.
The official prescribing information describes ribociclib as an inhibitor of CDK4 and CDK6, which are activated by binding to D-cyclins and are downstream of signaling pathways that lead to cell-cycle progression and cellular proliferation.
- Cyclin D-CDK4/6 normally phosphorylates retinoblastoma protein
In normal cell-cycle regulation, the cyclin D-CDK4/6 complex phosphorylates retinoblastoma protein, also called Rb or pRb. Rb is a tumor suppressor protein that normally restrains the transition from G1 phase to S phase.
When Rb is phosphorylated, it releases E2F transcription factors. These transcription factors activate genes required for DNA synthesis and cell division.
- Ribociclib reduces Rb phosphorylation
By inhibiting CDK4/6, Kisqali reduces phosphorylation of retinoblastoma protein. When Rb remains unphosphorylated or less phosphorylated, it continues to suppress E2F-mediated transcription.
This prevents the cancer cell from efficiently entering the DNA synthesis phase.
- G1 phase cell-cycle arrest
Reduced Rb phosphorylation causes arrest of cells in the G1 phase of the cell cycle. This means the cell is unable to progress normally into the S phase, where DNA replication occurs.
The result is reduced proliferation of breast cancer cells.
- Effect in HR-positive breast cancer
Hormone receptor-positive breast cancer often depends on estrogen receptor signaling. Estrogen signaling increases cyclin D expression, which activates CDK4/6 and promotes cell-cycle progression.
Kisqali blocks this downstream cell-cycle pathway. This is why it is combined with endocrine therapy such as aromatase inhibitors or fulvestrant. Endocrine therapy suppresses estrogen receptor signaling, while Kisqali blocks CDK4/6-driven cell division.
- Synergistic effect with endocrine therapy
Aromatase inhibitors reduce estrogen production, and fulvestrant blocks and degrades estrogen receptors. Ribociclib adds another level of control by inhibiting the cell-cycle machinery downstream of estrogen signaling.
This combination produces stronger tumor growth inhibition than endocrine therapy alone in suitable patients.
- Reduced tumor cell proliferation
By preventing G1-to-S phase transition, Kisqali slows the multiplication of cancer cells. It does not directly kill all cancer cells immediately like some cytotoxic agents. Instead, it suppresses proliferation and helps delay disease progression.
- Final therapeutic effect
The final therapeutic effect of Kisqali is inhibition of CDK4/6 activity, reduced Rb phosphorylation, G1 phase cell-cycle arrest, decreased breast cancer cell proliferation, improved disease control, reduced recurrence risk in selected early breast cancer patients, and improved outcomes in advanced or metastatic HR-positive, HER2-negative breast cancer.
Pharmacokinetics
Kisqali is administered orally as ribociclib tablets. It is taken once daily for 21 consecutive days followed by 7 days off treatment in a 28-day cycle. For early breast cancer, the recommended dose is 400 mg once daily with an aromatase inhibitor. For advanced or metastatic breast cancer, the recommended dose is 600 mg once daily with endocrine therapy.
Absorption:
Ribociclib is absorbed after oral administration. It may be taken with or without food. A high-fat, high-calorie meal does not produce clinically meaningful differences in ribociclib exposure.
Distribution:
Ribociclib is approximately 70% bound to plasma proteins. It has a large apparent volume of distribution at steady state, suggesting extensive tissue distribution.
Metabolism:
Ribociclib undergoes extensive hepatic metabolism mainly through CYP3A4. Its major circulating activity is mainly due to the parent drug, while circulating metabolites contribute minimally to clinical activity.
Excretion:
Ribociclib and its metabolites are eliminated mainly through feces, with a smaller amount eliminated in urine. After a radiolabeled dose, most of the administered radioactivity was recovered in feces and urine over time.
Half-life and duration:
The mean effective half-life of ribociclib is about 32 hours at steady state after the 600 mg dose in patients with advanced cancer. This supports once-daily dosing during the active 21-day treatment period.
Special pharmacokinetic point:
Because ribociclib is mainly metabolized by CYP3A4, strong CYP3A inhibitors can increase exposure and strong CYP3A inducers can reduce exposure. Ribociclib can also increase exposure of some CYP3A substrates. Drug interaction review is important before starting therapy.
Clinical Uses
- HR-positive, HER2-negative early breast cancer:
Kisqali is used with an aromatase inhibitor as adjuvant therapy in adults with stage II and III HR-positive, HER2-negative early breast cancer at high risk of recurrence.
- HR-positive, HER2-negative advanced or metastatic breast cancer:
Kisqali is used with an aromatase inhibitor as initial endocrine-based therapy in adults with advanced or metastatic disease.
- Combination with fulvestrant:
Kisqali is used with fulvestrant as initial endocrine-based therapy or after disease progression on endocrine therapy in adults with HR-positive, HER2-negative advanced or metastatic breast cancer.
- Premenopausal and perimenopausal patients:
When Kisqali is used with endocrine therapy in premenopausal or perimenopausal women, ovarian suppression with an LHRH agonist is used according to clinical practice.
- Male breast cancer:
Kisqali may also be used in men with HR-positive, HER2-negative advanced or metastatic breast cancer in combination with appropriate endocrine therapy and gonadal suppression where clinically required.
Adverse Effects
Common adverse effects of Kisqali include:
- Neutropenia
- Leukopenia
- Nausea
- Fatigue
- Diarrhea
- Vomiting
- Headache
- Constipation
- Alopecia
- Rash
- Cough
- Back pain
- Abdominal pain
- Decreased appetite
- Stomatitis
- Anemia
- Thrombocytopenia
- Increased liver enzymes
Important serious adverse effects include:
- QT interval prolongation
- Hepatotoxicity
- Severe neutropenia
- Interstitial lung disease or pneumonitis
- Severe cutaneous adverse reactions
- Embryo-fetal toxicity
- Serious infections due to myelosuppression
QT prolongation is a major exam point. Kisqali can prolong the QT interval in a concentration-dependent manner. ECG and electrolyte monitoring are recommended before and during therapy, and concomitant use with drugs known to prolong QT interval should generally be avoided.
Hepatotoxicity is another important adverse effect. Liver function tests should be monitored before and during treatment. Dose interruption, dose reduction, or discontinuation may be needed depending on severity.
Neutropenia is one of the most common dose-limiting adverse effects of CDK4/6 inhibitors. Complete blood counts should be monitored regularly. Unlike chemotherapy-associated neutropenia, CDK4/6 inhibitor-associated neutropenia is often reversible with dose interruption or reduction.
Kisqali can cause embryo-fetal harm based on its mechanism of action. Pregnancy should be avoided during therapy, and effective contraception is required for females of reproductive potential.
Comparative Analysis
| Feature | Kisqali | Ibrance | Verzenio | Fulvestrant |
|---|---|---|---|---|
| Generic name | Ribociclib | Palbociclib | Abemaciclib | Fulvestrant |
| Drug class | CDK4/6 inhibitor | CDK4/6 inhibitor | CDK4/6 inhibitor | Estrogen receptor antagonist/downregulator |
| Main target | CDK4 and CDK6 | CDK4 and CDK6 | CDK4 and CDK6 | Estrogen receptor |
| Main action | Blocks Rb phosphorylation and causes G1 arrest | Blocks Rb phosphorylation and causes G1 arrest | Blocks CDK4/6 with relatively continuous dosing | Blocks and degrades estrogen receptor |
| Main use | HR-positive, HER2-negative breast cancer | HR-positive, HER2-negative breast cancer | HR-positive, HER2-negative breast cancer | HR-positive breast cancer |
| Route | Oral | Oral | Oral | Intramuscular |
| Common schedule | 21 days on, 7 days off | 21 days on, 7 days off | Usually continuous dosing | Monthly after loading doses |
| Key adverse effect | Neutropenia, QT prolongation, hepatotoxicity | Neutropenia | Diarrhea, neutropenia, hepatotoxicity | Injection site pain, hot flashes |
| QT concern | Important | Less prominent | Less prominent | Not a major class issue |
Kisqali, Ibrance, and Verzenio are all CDK4/6 inhibitors used in HR-positive, HER2-negative breast cancer. Kisqali is especially associated with QT interval monitoring and liver function monitoring. Ibrance is strongly associated with neutropenia. Verzenio is more commonly associated with diarrhea and is often given continuously. Fulvestrant is different because it targets estrogen receptor signaling rather than directly inhibiting CDK4/6.
MCQs
- Kisqali contains which active drug?
a) Palbociclib
b) Ribociclib
c) Abemaciclib
d) Fulvestrant
Answer: b) Ribociclib
- Kisqali belongs to which drug class?
a) Aromatase inhibitor
b) CDK4/6 inhibitor
c) Alkylating agent
d) Anti-HER2 monoclonal antibody
Answer: b) CDK4/6 inhibitor
- The main enzymes inhibited by ribociclib are:
a) COX-1 and COX-2
b) CDK4 and CDK6
c) ACE and renin
d) CYP2D6 and CYP2C19
Answer: b) CDK4 and CDK6
- The cyclin D-CDK4/6 complex normally promotes phosphorylation of:
a) Retinoblastoma protein
b) Hemoglobin
c) Albumin
d) Insulin receptor only
Answer: a) Retinoblastoma protein
- Inhibition of CDK4/6 by Kisqali causes arrest in which cell-cycle phase?
a) G1 phase
b) M phase
c) G2 phase only
d) Cytokinesis only
Answer: a) G1 phase
- Kisqali is mainly used in which breast cancer subtype?
a) HR-positive, HER2-negative breast cancer
b) HER2-positive only breast cancer
c) Triple-negative breast cancer only
d) BRCA-negative ovarian cancer only
Answer: a) HR-positive, HER2-negative breast cancer
- Kisqali is commonly combined with:
a) Endocrine therapy
b) Penicillin
c) Insulin only
d) Heparin only
Answer: a) Endocrine therapy
- Which adverse effect is an important warning with Kisqali?
a) QT interval prolongation
b) Severe ototoxicity
c) Gingival hyperplasia
d) Hypocalcemia only
Answer: a) QT interval prolongation
- Which blood-related adverse effect is common with Kisqali?
a) Neutropenia
b) Polycythemia
c) Eosinophilia only
d) Thrombocytosis
Answer: a) Neutropenia
- Ribociclib is mainly metabolized by:
a) CYP3A4
b) CYP2D6
c) Acetylcholinesterase
d) Monoamine oxidase-B
Answer: a) CYP3A4
- Which monitoring is important during Kisqali therapy?
a) ECG, electrolytes, liver function tests, and complete blood count
b) Only serum calcium
c) Only blood group
d) Only uric acid
Answer: a) ECG, electrolytes, liver function tests, and complete blood count
- Kisqali reduces cancer cell proliferation by:
a) Preventing G1-to-S phase cell-cycle progression
b) Directly blocking bacterial cell wall synthesis
c) Increasing insulin secretion
d) Blocking histamine receptors only
Answer: a) Preventing G1-to-S phase cell-cycle progression
- Which drug is another CDK4/6 inhibitor?
a) Palbociclib
b) Trastuzumab
c) Tamoxifen
d) Letrozole
Answer: a) Palbociclib
- Kisqali should generally be avoided with drugs that:
a) Prolong QT interval
b) Contain vitamin C
c) Increase dietary fiber
d) Reduce gastric acid only
Answer: a) Prolong QT interval
- Which statement about Kisqali is correct?
a) It inhibits CDK4/6, reduces Rb phosphorylation, and causes G1 arrest
b) It is a HER2 receptor antibody
c) It is a direct estrogen replacement therapy
d) It is a rescue medicine for asthma
Answer: a) It inhibits CDK4/6, reduces Rb phosphorylation, and causes G1 arrest
FAQs
- What is Kisqali used for?
Kisqali is used in HR-positive, HER2-negative breast cancer. It is used with endocrine therapy in selected early breast cancer patients at high risk of recurrence and in adults with advanced or metastatic breast cancer.
- What is the mechanism of action of Kisqali?
Kisqali inhibits CDK4 and CDK6. This reduces phosphorylation of retinoblastoma protein, prevents G1-to-S phase cell-cycle progression, and decreases breast cancer cell proliferation.
- Is Kisqali chemotherapy?
Kisqali is not traditional cytotoxic chemotherapy. It is a targeted anticancer drug that blocks CDK4/6-mediated cell-cycle progression.
- Why is Kisqali combined with endocrine therapy?
HR-positive breast cancer growth is driven by estrogen receptor signaling, which promotes cyclin D-CDK4/6 activity. Endocrine therapy blocks estrogen signaling, while Kisqali blocks downstream cell-cycle progression.
- What is the most important adverse effect of Kisqali?
Neutropenia is very common and clinically important. QT interval prolongation and hepatotoxicity are also major safety concerns.
- Why is ECG monitoring needed with Kisqali?
Kisqali can prolong the QT interval, which may increase the risk of serious heart rhythm abnormalities. ECG and electrolyte monitoring help reduce this risk.
- Can Kisqali cause liver injury?
Yes. Kisqali can cause hepatotoxicity, including increased ALT and AST. Liver function tests should be monitored before and during therapy.
- How is Kisqali taken?
Kisqali is taken orally once daily for 21 consecutive days followed by 7 days off treatment in a 28-day cycle. It may be taken with or without food.
- Which enzyme metabolizes Kisqali?
Ribociclib is mainly metabolized by CYP3A4, so CYP3A inhibitors and inducers can significantly affect ribociclib exposure.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology
K.D. Tripathi Essentials of Medical Pharmacology
Harrison’s Principles of Internal Medicine

