
Table of Contents
Introduction
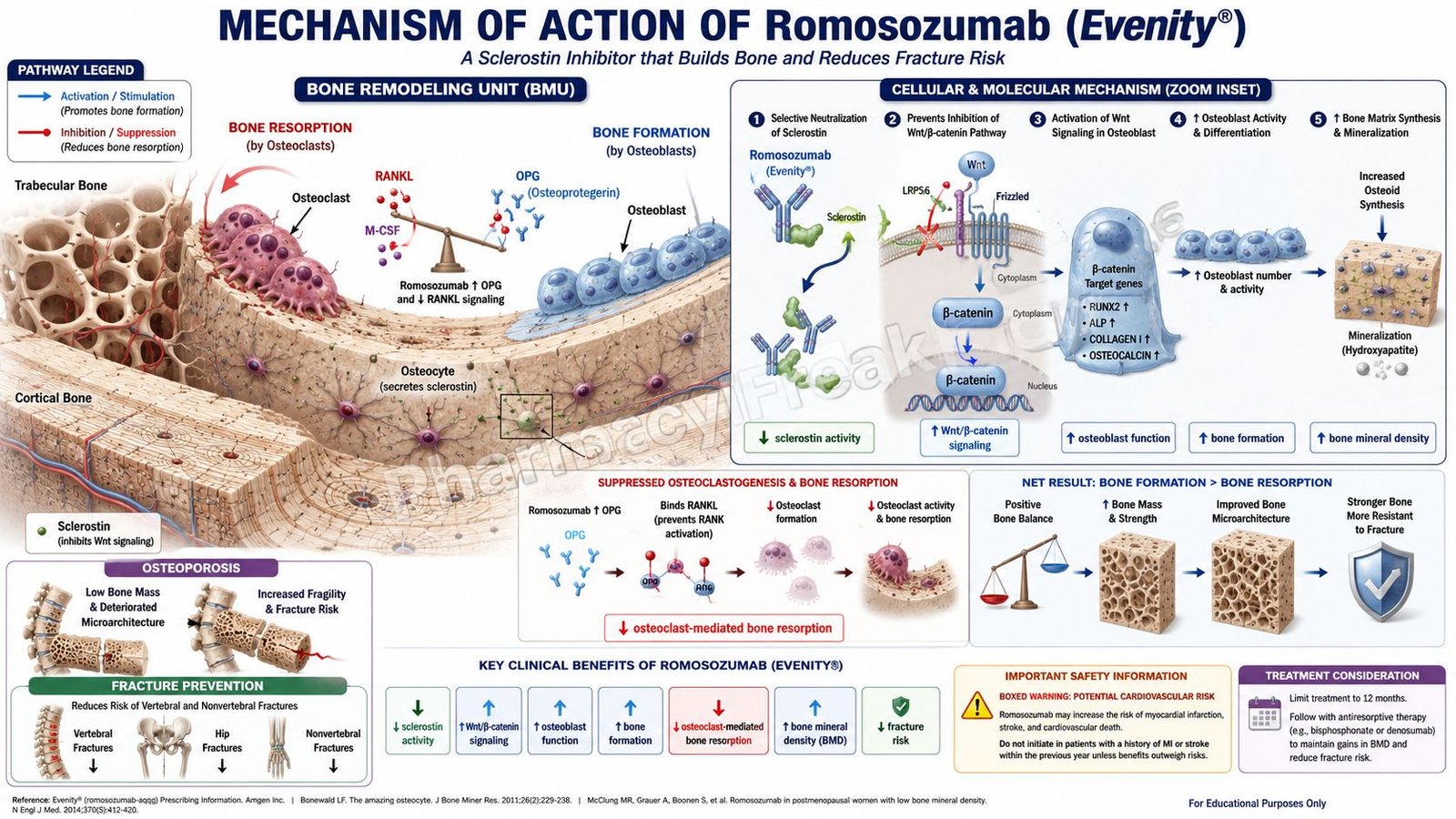
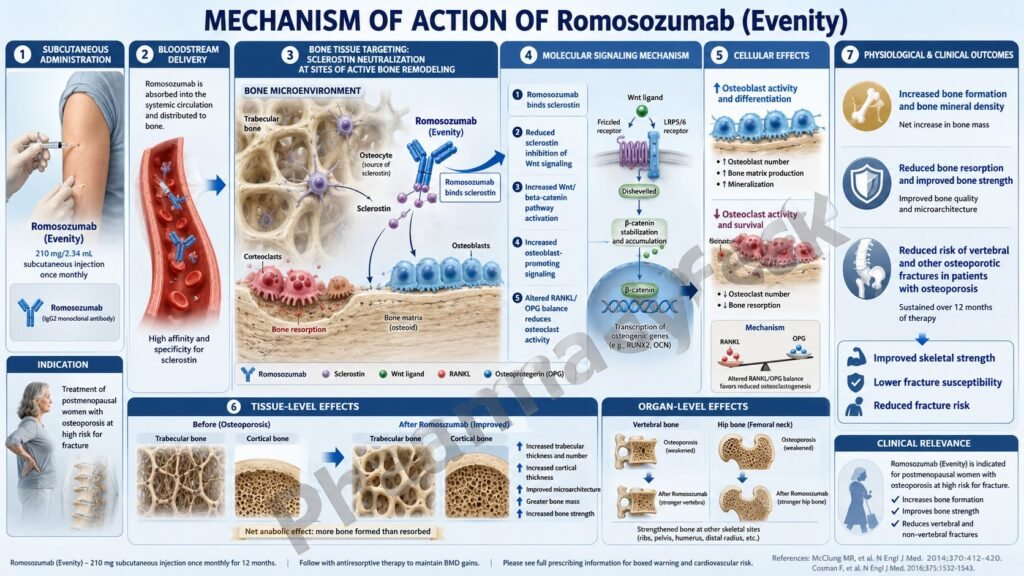
Romosozumab is a humanized monoclonal antibody used for the treatment of osteoporosis in postmenopausal women who are at high risk of fracture. It is marketed under the brand name Evenity. Pharmacologically, romosozumab belongs to the sclerostin inhibitor class and is considered an anabolic bone-forming therapy with an additional antiresorptive effect.
Osteoporosis is characterized by reduced bone mass, deterioration of bone microarchitecture, and increased fracture risk. In postmenopausal women, estrogen deficiency increases bone resorption and gradually reduces bone strength. Traditional osteoporosis drugs such as bisphosphonates mainly reduce bone resorption, while romosozumab has a distinct mechanism because it increases bone formation and also decreases bone resorption.
The main target of romosozumab is sclerostin, a regulatory glycoprotein produced mainly by osteocytes. Sclerostin normally inhibits bone formation by suppressing Wnt signaling in osteoblast-lineage cells. By binding to and inhibiting sclerostin, romosozumab stimulates osteoblast activity, increases bone matrix production, improves bone mass, and reduces fracture risk.
For exam purposes, romosozumab should be remembered as a monoclonal antibody against sclerostin that activates bone formation through the Wnt pathway and mildly decreases bone resorption. It is used for postmenopausal osteoporosis at high fracture risk, but it has an important boxed warning for potential risk of myocardial infarction, stroke, and cardiovascular death. Current labeling says it should not be initiated in patients who had myocardial infarction or stroke within the preceding year.
Mechanism of Action (Step-wise)
Step 1: Osteocytes produce sclerostin
Osteocytes are mature bone cells embedded within the mineralized bone matrix. They act as mechanical sensors and regulators of bone remodeling. One important protein produced by osteocytes is sclerostin.
Step 2: Sclerostin normally inhibits bone formation
Sclerostin is a negative regulator of bone formation. It suppresses osteoblast-mediated bone formation by inhibiting Wnt/β-catenin signaling. When sclerostin activity is high, osteoblast differentiation and activity decrease, leading to reduced bone formation.
Step 3: Wnt signaling promotes osteoblast function
The Wnt/β-catenin pathway is essential for osteoblast development, survival, and activity. When Wnt signaling is active, osteoblast-lineage cells produce bone matrix, promote mineralization, and increase bone strength.
Step 4: Romosozumab binds to sclerostin
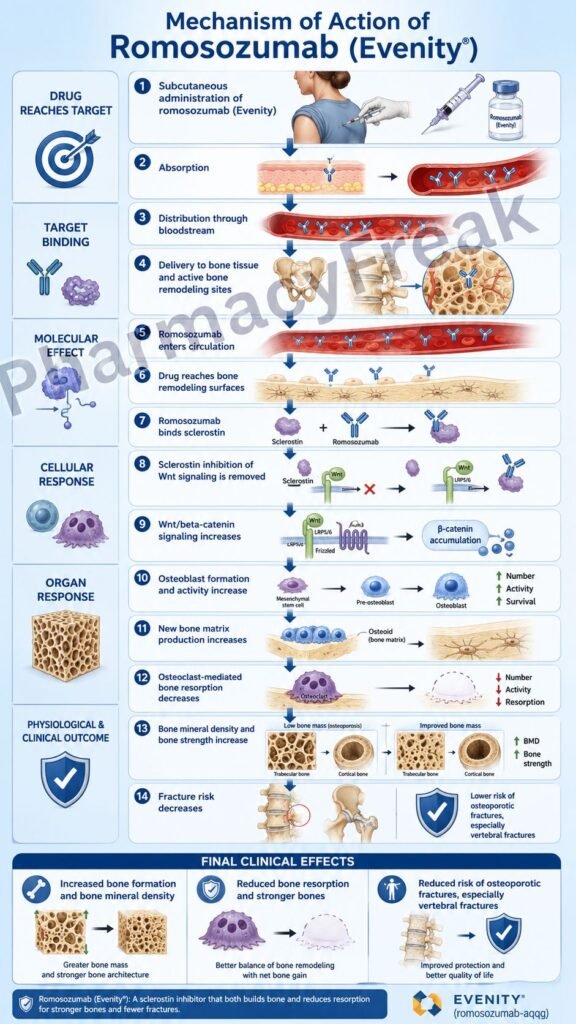
Romosozumab is a humanized IgG2 monoclonal antibody that binds to sclerostin and inhibits its action. By neutralizing sclerostin, romosozumab removes an important inhibitory signal from bone-forming cells.
Step 5: Wnt/β-catenin signaling increases
When sclerostin is inhibited, Wnt signaling becomes more active in osteoblast-lineage cells. This promotes osteoblast differentiation, osteoblast activity, and bone matrix production.
Step 6: Bone formation increases
The major therapeutic effect of romosozumab is increased bone formation. It activates bone lining cells, increases osteoblast-mediated bone matrix production, and recruits osteoprogenitor cells. This leads to new bone formation on trabecular and cortical bone surfaces.
Step 7: Bone resorption decreases
Romosozumab also produces a mild antiresorptive effect. It changes the expression of osteoclast-regulating mediators, resulting in reduced osteoclast activity and decreased bone resorption. This dual action is clinically important because most osteoporosis drugs either mainly stimulate formation or mainly inhibit resorption, while romosozumab does both.
Step 8: Trabecular and cortical bone mass improve
By increasing bone formation and decreasing bone resorption, romosozumab increases both trabecular and cortical bone mass. Trabecular bone is important in vertebrae, while cortical bone contributes significantly to hip and long-bone strength.
Step 9: Bone mineral density increases
As bone formation rises and resorption falls, bone mineral density increases. Improvements are commonly seen at clinically important sites such as the lumbar spine, total hip, and femoral neck.
Step 10: Fracture risk decreases
The final therapeutic outcome is reduction in fracture risk. Romosozumab helps reduce vertebral and clinical fractures in appropriately selected postmenopausal women with osteoporosis at high fracture risk.
Step 11: Treatment effect should be followed by antiresorptive therapy
Romosozumab treatment is limited to 12 monthly doses. After completing therapy, patients are commonly transitioned to an antiresorptive drug such as a bisphosphonate or denosumab to maintain gains in bone mineral density and fracture protection.
Pharmacokinetics
Romosozumab is administered by subcutaneous injection. The recommended dose is 210 mg once every month for 12 doses. A full monthly dose is given as two separate subcutaneous injections, each containing 105 mg. The injections are usually given in the abdomen, thigh, or upper arm.
After subcutaneous administration, romosozumab is absorbed slowly into the systemic circulation. Because it is a monoclonal antibody, it is not absorbed orally and cannot be given as a conventional tablet or capsule.
Romosozumab has pharmacokinetics typical of therapeutic antibodies. It is expected to be degraded into small peptides and amino acids through catabolic pathways rather than being primarily metabolized by hepatic cytochrome P450 enzymes. Therefore, CYP450-mediated drug interactions are not a major concern.
Its elimination pathway has not been fully characterized, which is common for monoclonal antibodies. Renal excretion of unchanged drug is not expected to be a major elimination route because romosozumab is a large protein molecule. However, patients with severe renal impairment or dialysis are at increased risk of hypocalcemia and require careful calcium monitoring and supplementation.
Calcium and vitamin D supplementation are important during treatment. Pre-existing hypocalcemia must be corrected before starting romosozumab, and patients should receive adequate calcium and vitamin D during therapy.
The duration of therapy is limited to 12 monthly doses because the anabolic effect decreases over time and because product labeling does not recommend use beyond one year. After completion, antiresorptive therapy is usually used to preserve bone density improvements.
Clinical Uses
Romosozumab is used for the treatment of osteoporosis in postmenopausal women at high risk for fracture. High-risk patients may include those with a history of osteoporotic fracture, multiple fracture risk factors, or patients who have failed or cannot tolerate other osteoporosis therapies.
It is especially useful when rapid improvement in bone mineral density and fracture protection is desired. Because of its strong anabolic effect, romosozumab is often considered in patients with severe osteoporosis or very high fracture risk.
Romosozumab is not used as a first choice for every patient with low bone density. In patients with mild osteoporosis or lower fracture risk, other drugs such as bisphosphonates may be used first. Romosozumab is usually selected when the expected fracture benefit justifies its risks.
After 12 months of romosozumab, therapy should generally be followed by an antiresorptive osteoporosis drug. This is important because bone mineral density gains may decline after stopping anabolic therapy if maintenance treatment is not used.
Romosozumab is not approved for pediatric osteoporosis and is not used for routine osteoporosis prevention in healthy postmenopausal women without high fracture risk. It is also not a treatment for osteoarthritis, rheumatoid arthritis, bone pain unrelated to osteoporosis, or acute fractures.
Adverse Effects
The most important safety issue with romosozumab is the potential risk of major adverse cardiovascular events, including myocardial infarction, stroke, and cardiovascular death. It should not be initiated in patients who have had myocardial infarction or stroke within the preceding year. If myocardial infarction or stroke occurs during treatment, romosozumab should be discontinued.
Hypocalcemia is another important adverse effect. Romosozumab is contraindicated in patients with hypocalcemia until it is corrected. Patients with severe renal impairment or those receiving dialysis are at greater risk and need careful calcium monitoring.
Common adverse effects include arthralgia and headache. Injection-site reactions may also occur and can include pain, redness, swelling, or irritation at the injection site.
Hypersensitivity reactions may occur, including rash, urticaria, dermatitis, angioedema, and erythema multiforme. Serious allergic reactions require discontinuation and appropriate treatment.
Osteonecrosis of the jaw has been reported with romosozumab. The risk may be higher in patients with poor oral hygiene, invasive dental procedures, cancer, chemotherapy, corticosteroid use, or previous exposure to antiresorptive drugs. A routine oral examination is recommended before starting therapy.
Atypical femoral fractures have also been reported with drugs affecting bone remodeling, including romosozumab. New or unusual thigh, hip, or groin pain should be evaluated.
Other possible adverse effects include muscle spasms, neck pain, insomnia, paresthesia, and mild injection-related discomfort. Overall monitoring should focus on cardiovascular history, calcium status, renal impairment, oral health, and signs of unusual bone pain.
Comparative Analysis
Romosozumab differs from bisphosphonates such as alendronate, risedronate, ibandronate, and zoledronic acid. Bisphosphonates mainly inhibit osteoclast-mediated bone resorption by binding to bone mineral and impairing osteoclast function. Romosozumab mainly increases bone formation by inhibiting sclerostin and activating Wnt signaling, while also reducing resorption.
Compared with denosumab, romosozumab has a stronger anabolic bone-forming action. Denosumab is a monoclonal antibody against RANKL and primarily decreases osteoclast formation, function, and survival. Romosozumab targets sclerostin and has a dual effect of increased formation and decreased resorption.
Compared with teriparatide, romosozumab has a different anabolic mechanism. Teriparatide is recombinant parathyroid hormone 1-34 and stimulates bone formation when given intermittently. Romosozumab works through sclerostin inhibition and Wnt pathway activation. Teriparatide may increase bone remodeling overall, while romosozumab increases formation and decreases resorption.
Compared with abaloparatide, romosozumab again differs by target. Abaloparatide is a parathyroid hormone-related peptide analog acting on PTH1 receptors, while romosozumab is an anti-sclerostin monoclonal antibody.
Compared with calcitonin, romosozumab is much more potent for improving bone mineral density and reducing fracture risk in high-risk postmenopausal osteoporosis. Calcitonin has weak antiresorptive activity and is rarely preferred for long-term osteoporosis management.
A key clinical difference is cardiovascular warning. Bisphosphonates, denosumab, teriparatide, and abaloparatide do not carry the same boxed warning for myocardial infarction, stroke, and cardiovascular death that is associated with romosozumab. This makes cardiovascular risk assessment an important part of romosozumab selection.
MCQs
- Romosozumab belongs to which pharmacological class?
a) Sclerostin inhibitor
b) Bisphosphonate
c) Calcitonin receptor agonist
d) Selective estrogen receptor modulator
Answer: a) Sclerostin inhibitor
- The brand name of romosozumab is:
a) Evenity
b) Prolia
c) Forteo
d) Fosamax
Answer: a) Evenity
- Romosozumab is mainly used for:
a) Postmenopausal osteoporosis at high fracture risk
b) Acute gout attack
c) Rheumatoid arthritis flare
d) Osteomyelitis
Answer: a) Postmenopausal osteoporosis at high fracture risk
- The main molecular target of romosozumab is:
a) Sclerostin
b) RANKL
c) TNF-alpha
d) COX-2
Answer: a) Sclerostin
- Sclerostin is produced mainly by:
a) Osteocytes
b) Chondrocytes only
c) Erythrocytes
d) Pancreatic beta cells
Answer: a) Osteocytes
- Sclerostin normally inhibits which pathway involved in bone formation?
a) Wnt/β-catenin pathway
b) Renin-angiotensin pathway
c) Dopamine pathway
d) Coagulation cascade
Answer: a) Wnt/β-catenin pathway
- Romosozumab increases bone formation mainly by:
a) Neutralizing sclerostin and increasing osteoblast activity
b) Destroying osteoblasts
c) Blocking calcium absorption from intestine
d) Inhibiting vitamin D activation
Answer: a) Neutralizing sclerostin and increasing osteoblast activity
- Which additional effect does romosozumab have on bone remodeling?
a) Decreases bone resorption
b) Increases bone resorption only
c) Completely stops mineralization
d) Causes immediate bone dissolution
Answer: a) Decreases bone resorption
- The recommended duration of romosozumab therapy is limited to:
a) 12 monthly doses
b) Lifelong daily tablets
c) One dose only
d) Five years continuously
Answer: a) 12 monthly doses
- A full monthly romosozumab dose is usually given as:
a) Two subcutaneous injections totaling 210 mg
b) One oral tablet of 70 mg
c) Continuous intravenous infusion
d) Intranasal spray daily
Answer: a) Two subcutaneous injections totaling 210 mg
- Which boxed warning is associated with romosozumab?
a) Myocardial infarction, stroke, and cardiovascular death
b) Severe neutropenia only
c) Pulmonary fibrosis in every patient
d) Irreversible hearing loss
Answer: a) Myocardial infarction, stroke, and cardiovascular death
- Romosozumab should not be initiated in patients who had myocardial infarction or stroke within:
a) The preceding year
b) The preceding 24 hours only
c) Childhood only
d) The preceding 10 years in all cases
Answer: a) The preceding year
- Which condition must be corrected before starting romosozumab?
a) Hypocalcemia
b) Mild headache
c) Seasonal allergy
d) Hyperuricemia only
Answer: a) Hypocalcemia
- Which adverse effect is commonly reported with romosozumab?
a) Arthralgia
b) Severe hypoglycemia
c) Gingival hyperplasia
d) Ototoxicity
Answer: a) Arthralgia
- Which drug primarily inhibits RANKL and is commonly compared with romosozumab?
a) Denosumab
b) Teriparatide
c) Alendronate
d) Calcitonin
Answer: a) Denosumab
FAQs
What is the mechanism of action of romosozumab?
Romosozumab is a monoclonal antibody that binds to and inhibits sclerostin. This increases Wnt/β-catenin signaling, stimulates osteoblast activity, increases bone formation, and also decreases bone resorption.
What is the brand name of romosozumab?
The brand name of romosozumab is Evenity.
Why does romosozumab increase bone formation?
Romosozumab blocks sclerostin, which normally suppresses osteoblast activity. When sclerostin is inhibited, osteoblast differentiation and bone matrix production increase.
Is romosozumab anabolic or antiresorptive?
Romosozumab has a dual effect. It is mainly anabolic because it increases bone formation, but it also decreases bone resorption to some extent.
How long is romosozumab given?
Romosozumab is given once monthly for 12 doses. Treatment is usually followed by an antiresorptive drug to maintain bone density gains.
What is the most important warning for romosozumab?
The most important warning is the potential risk of myocardial infarction, stroke, and cardiovascular death. It should not be started in patients who had myocardial infarction or stroke within the previous year.
Why is calcium important during romosozumab therapy?
Romosozumab can cause hypocalcemia. Pre-existing hypocalcemia must be corrected before therapy, and patients should receive adequate calcium and vitamin D during treatment.
How is romosozumab different from denosumab?
Romosozumab inhibits sclerostin and increases bone formation, while denosumab inhibits RANKL and mainly decreases osteoclast-mediated bone resorption.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

