
Table of Contents
Introduction
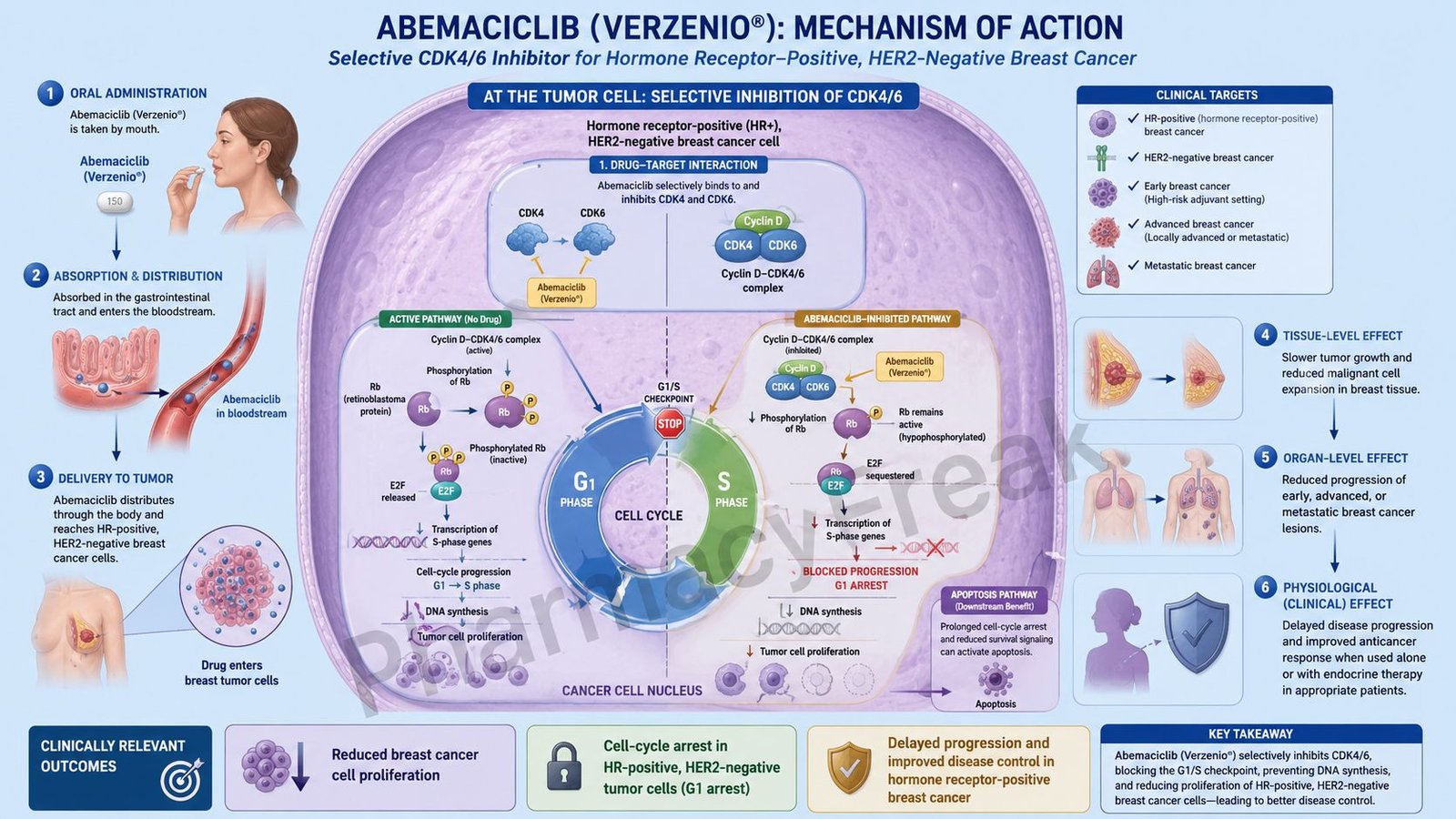
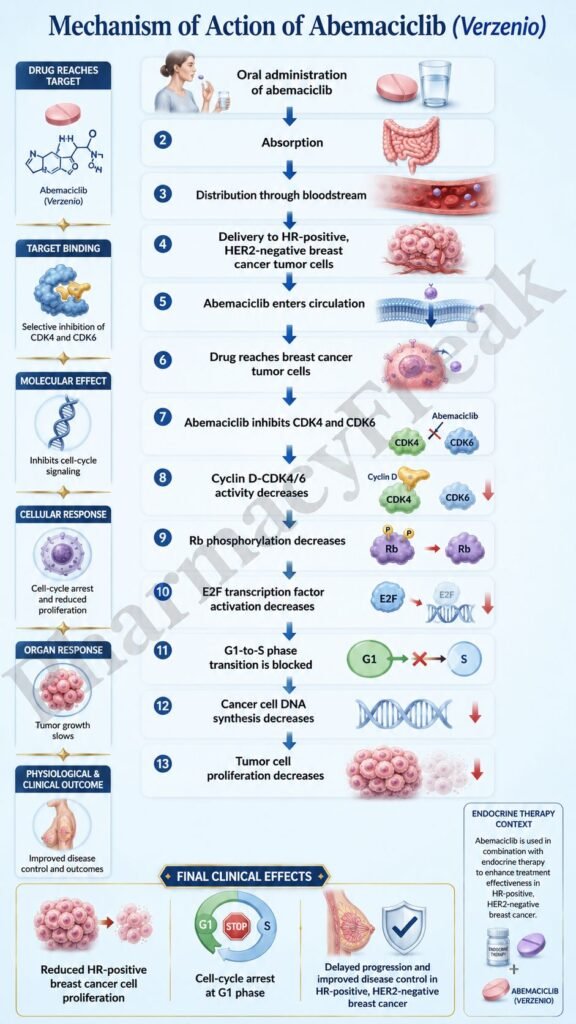
Abemaciclib is an oral targeted anticancer drug used mainly in hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer. It is marketed under the brand name Verzenio. Pharmacologically, abemaciclib belongs to the cyclin-dependent kinase 4 and 6 inhibitor class, commonly abbreviated as CDK4/6 inhibitors.
CDK4 and CDK6 are important enzymes involved in cell-cycle progression. In many hormone receptor-positive breast cancers, estrogen signaling increases cyclin D activity, which activates CDK4 and CDK6. These kinases phosphorylate the retinoblastoma protein, allowing cancer cells to move from the G1 phase into the S phase of the cell cycle. Once cells enter S phase, DNA synthesis begins and cancer cells continue proliferating.
Abemaciclib works by inhibiting CDK4 and CDK6, thereby reducing retinoblastoma protein phosphorylation, blocking G1-to-S phase progression, and slowing tumor cell proliferation. It is especially useful in HR-positive, HER2-negative breast cancer because this cancer subtype often depends strongly on the cyclin D-CDK4/6-retinoblastoma pathway.
For exam purposes, abemaciclib should be remembered as an oral CDK4/6 inhibitor used in HR-positive, HER2-negative breast cancer, commonly in combination with endocrine therapy. Current labeling includes use in selected high-risk early breast cancer and advanced or metastatic breast cancer settings.
Mechanism of Action (Step-wise)
Step 1: Cell-cycle progression is controlled by cyclins and CDKs
Normal cells divide through a regulated cell cycle. Important phases include G1 phase, S phase, G2 phase, and M phase. Progression from G1 phase to S phase is a major checkpoint because S phase is where DNA replication occurs.
Step 2: Cyclin D activates CDK4 and CDK6
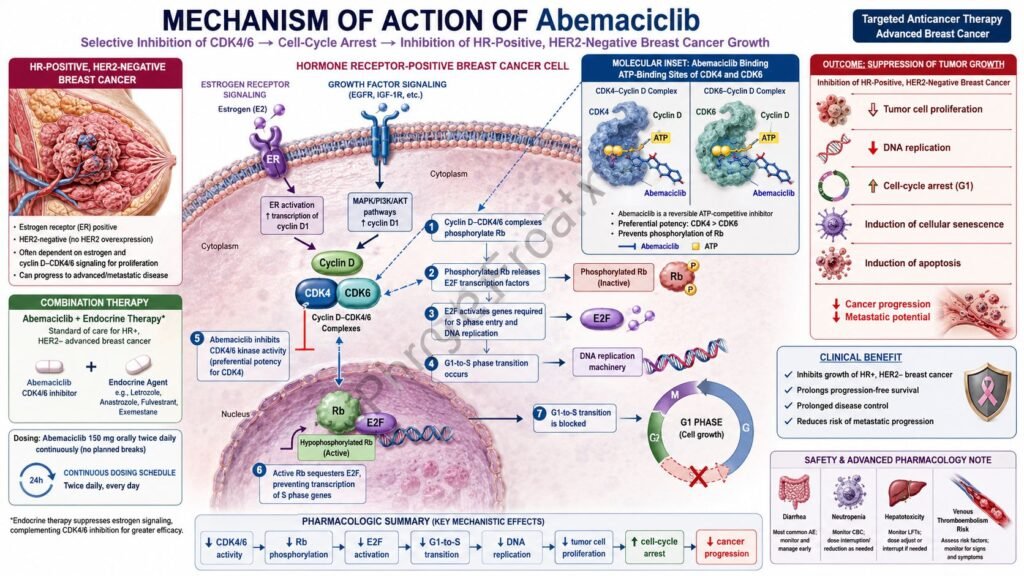
Cyclin D binds to and activates CDK4 and CDK6. This cyclin D-CDK4/6 complex is especially important in early cell-cycle progression. In hormone receptor-positive breast cancer, estrogen receptor signaling can increase cyclin D expression, making this pathway highly active.
Step 3: CDK4/6 phosphorylates retinoblastoma protein
The retinoblastoma protein, commonly called Rb, is a tumor suppressor protein. In its active, hypophosphorylated state, Rb binds E2F transcription factors and prevents transcription of genes required for DNA synthesis.
Step 4: Rb phosphorylation releases E2F
When CDK4 and CDK6 phosphorylate Rb, Rb becomes functionally inactive. This releases E2F transcription factors. Free E2F then activates genes required for DNA replication and S-phase entry.
Step 5: Cancer cells enter S phase and proliferate
After E2F activation, cells move from G1 phase into S phase. DNA synthesis begins, and cancer cells continue dividing. In HR-positive breast cancer, this pathway contributes significantly to tumor growth.
Step 6: Abemaciclib inhibits CDK4 and CDK6
Abemaciclib selectively inhibits cyclin-dependent kinases 4 and 6. By blocking these enzymes, it prevents phosphorylation of the retinoblastoma protein. This is the central molecular action of abemaciclib.
Step 7: Rb remains active in its growth-suppressive form
When Rb is not phosphorylated, it continues to bind E2F transcription factors. This prevents transcription of genes needed for DNA synthesis and cell-cycle progression.
Step 8: G1-to-S phase transition is blocked
Because E2F remains inhibited, cancer cells cannot efficiently move from G1 phase to S phase. This produces cell-cycle arrest, mainly at the G1 checkpoint.
Step 9: Tumor cell proliferation decreases
The final therapeutic effect is reduced proliferation of cancer cells. In sensitive tumors, prolonged CDK4/6 inhibition may also promote cellular senescence and, in some settings, apoptosis.
Step 10: Endocrine therapy enhances the effect
In HR-positive breast cancer, estrogen receptor signaling drives cyclin D production. Endocrine therapies such as aromatase inhibitors, tamoxifen, or fulvestrant reduce estrogen receptor signaling. When abemaciclib is combined with endocrine therapy, both upstream estrogen signaling and downstream CDK4/6 cell-cycle signaling are suppressed.
Step 11: Functional Rb is important for response
CDK4/6 inhibitors depend on an intact retinoblastoma pathway. If tumor cells have complete loss of functional Rb, blocking CDK4/6 may be less effective because the main downstream checkpoint is already absent.
Step 12: Abemaciclib differs slightly from other CDK4/6 inhibitors
Abemaciclib is pharmacologically related to palbociclib and ribociclib, but it is often described as having relatively greater continuous dosing potential and clinically prominent gastrointestinal toxicity, especially diarrhea. Like the other drugs in the class, its major anticancer mechanism remains CDK4/6 inhibition.
Pharmacokinetics
Abemaciclib is administered orally as tablets. It may be taken with or without food. In combination regimens, the commonly used dose is 150 mg twice daily. As monotherapy in metastatic breast cancer after prior endocrine therapy and chemotherapy, the recommended dose is higher, commonly 200 mg twice daily, depending on clinical context and tolerability.
After oral administration, abemaciclib is absorbed systemically. Its absolute bioavailability is approximately 45%, and peak plasma concentrations occur several hours after dosing. Abemaciclib is highly protein bound.
Abemaciclib is metabolized mainly by CYP3A4. It forms active metabolites, including N-desethylabemaciclib and hydroxy metabolites, which contribute to overall pharmacological activity. Because of CYP3A metabolism, drug interactions are clinically important.
Strong CYP3A inhibitors can increase abemaciclib exposure and raise the risk of toxicity. Examples include clarithromycin, itraconazole, ketoconazole, ritonavir, and some other azole antifungals or antiviral drugs. Strong CYP3A inducers such as rifampin, carbamazepine, phenytoin, and St. John’s wort can reduce abemaciclib exposure and may reduce effectiveness.
Abemaciclib is eliminated mainly through feces, with minor renal elimination. The terminal elimination half-life is approximately 18 hours, which supports twice-daily dosing. Dose modification may be needed for significant toxicity, severe hepatic impairment, or important drug interactions.
Clinical Uses
Abemaciclib is used in adult patients with HR-positive, HER2-negative breast cancer. Its major clinical uses include both early breast cancer and advanced or metastatic breast cancer settings.
In early breast cancer, abemaciclib is used in combination with endocrine therapy, such as tamoxifen or an aromatase inhibitor, for adults with HR-positive, HER2-negative, node-positive early breast cancer who are at high risk of recurrence. High-risk features are based on nodal involvement, tumor size, tumor grade, and related clinical criteria.
In advanced or metastatic breast cancer, abemaciclib may be used with an aromatase inhibitor as initial endocrine-based therapy in adults with HR-positive, HER2-negative disease.
It may also be used with fulvestrant in adults with HR-positive, HER2-negative advanced or metastatic breast cancer whose disease has progressed after endocrine therapy.
Abemaciclib can also be used as monotherapy in adults with HR-positive, HER2-negative advanced or metastatic breast cancer whose disease has progressed after endocrine therapy and prior chemotherapy in the metastatic setting.
Abemaciclib is not used for all breast cancers. It is specifically relevant to HR-positive, HER2-negative disease. It is not a general treatment for HER2-positive breast cancer, triple-negative breast cancer, or non-breast cancers unless used in a clinical trial or specialist-directed setting.
Adverse Effects
The most characteristic adverse effect of abemaciclib is diarrhea. Diarrhea can occur early during treatment and may become severe if not managed promptly. Patients are usually advised to start antidiarrheal therapy such as loperamide at the first sign of loose stools, increase oral fluids, and contact their healthcare provider if symptoms persist.
Neutropenia is another important adverse effect, although abemaciclib generally causes less severe neutropenia than palbociclib and ribociclib in many clinical comparisons. Complete blood counts should be monitored before and during therapy.
Other hematological adverse effects include leukopenia, anemia, lymphopenia, and thrombocytopenia. Infection risk may increase, especially when neutropenia is present.
Hepatotoxicity can occur. Liver function tests should be monitored before treatment and periodically during therapy. Elevations in ALT, AST, and bilirubin may require dose interruption, dose reduction, or discontinuation depending on severity.
Venous thromboembolism is an important warning, especially when abemaciclib is used with endocrine therapy. Patients should be monitored for symptoms such as leg swelling, chest pain, shortness of breath, or sudden unexplained respiratory symptoms.
Interstitial lung disease and pneumonitis have been reported with CDK4/6 inhibitors, including abemaciclib. New or worsening cough, dyspnea, fever, or hypoxia should be evaluated carefully.
Other common adverse effects include nausea, vomiting, fatigue, abdominal pain, decreased appetite, headache, alopecia, dizziness, stomatitis, rash, increased serum creatinine due to inhibition of renal tubular secretion, and weight loss.
Abemaciclib can cause embryo-fetal toxicity. Females of reproductive potential should use effective contraception during treatment and for the recommended period after the last dose. It should generally be avoided during pregnancy unless the potential benefit clearly justifies the risk.
Comparative Analysis
Abemaciclib is commonly compared with palbociclib and ribociclib, the other major CDK4/6 inhibitors used in HR-positive, HER2-negative breast cancer.
All three drugs inhibit CDK4 and CDK6, reduce Rb phosphorylation, block G1-to-S phase transition, and slow cancer cell proliferation. They are commonly combined with endocrine therapy because estrogen receptor signaling and CDK4/6 signaling are closely connected in HR-positive breast cancer.
Compared with palbociclib, abemaciclib is given continuously in many regimens, while palbociclib is commonly given on a 3-weeks-on, 1-week-off schedule. Palbociclib is strongly associated with neutropenia. Abemaciclib is more strongly associated with diarrhea.
Compared with ribociclib, abemaciclib has less emphasis on QT prolongation monitoring, while ribociclib has important QT interval and liver monitoring requirements. However, abemaciclib still requires monitoring for diarrhea, blood counts, liver toxicity, thromboembolism, and lung toxicity.
Compared with endocrine therapy alone, abemaciclib plus endocrine therapy provides stronger blockade of tumor growth signaling in selected HR-positive, HER2-negative breast cancer. Endocrine therapy reduces estrogen receptor-driven signaling, while abemaciclib blocks downstream cell-cycle progression.
Compared with cytotoxic chemotherapy, abemaciclib is a targeted therapy. It does not directly damage DNA like anthracyclines, alkylating agents, or platinum drugs. Instead, it blocks cell-cycle progression through CDK4/6 inhibition. However, targeted therapy does not mean toxicity-free; abemaciclib can still cause serious adverse effects.
Compared with HER2-targeted drugs such as trastuzumab, abemaciclib is used in HER2-negative breast cancer. Trastuzumab targets HER2 receptor signaling, while abemaciclib targets CDK4/6-mediated cell-cycle progression.
MCQs
- Abemaciclib belongs to which pharmacological class?
a) CDK4/6 inhibitor
b) PARP inhibitor
c) EGFR inhibitor
d) VEGF inhibitor
Answer: a) CDK4/6 inhibitor
- The brand name of abemaciclib is:
a) Verzenio
b) Ibrance
c) Kisqali
d) Lynparza
Answer: a) Verzenio
- Abemaciclib is mainly used in which breast cancer subtype?
a) HR-positive, HER2-negative breast cancer
b) HER2-positive breast cancer only
c) Triple-negative breast cancer only
d) Medullary thyroid cancer
Answer: a) HR-positive, HER2-negative breast cancer
- Abemaciclib inhibits which enzymes?
a) CDK4 and CDK6
b) COX-1 and COX-2
c) ACE and renin
d) PARP1 and PARP2
Answer: a) CDK4 and CDK6
- CDK4/6 normally promotes cell-cycle progression by phosphorylating:
a) Retinoblastoma protein
b) Hemoglobin
c) Acetylcholine receptor
d) Albumin
Answer: a) Retinoblastoma protein
- When Rb is phosphorylated, which transcription factor is released?
a) E2F
b) NFAT
c) HIF-1 alpha
d) STAT5 only
Answer: a) E2F
- The main cell-cycle effect of abemaciclib is:
a) G1 phase arrest
b) M phase acceleration
c) Immediate DNA cross-linking
d) Complete ribosome destruction
Answer: a) G1 phase arrest
- Which adverse effect is most characteristic of abemaciclib?
a) Diarrhea
b) Ototoxicity
c) Gingival hyperplasia
d) Severe hypoglycemia
Answer: a) Diarrhea
- Abemaciclib is metabolized mainly by:
a) CYP3A4
b) CYP2C19 only
c) Monoamine oxidase
d) Acetylcholinesterase
Answer: a) CYP3A4
- Which drug interaction may reduce abemaciclib effectiveness?
a) Strong CYP3A inducer
b) Mild antacid use only
c) Topical moisturizer
d) Oral rehydration solution
Answer: a) Strong CYP3A inducer
- Which monitoring is important during abemaciclib therapy?
a) Complete blood counts and liver function tests
b) Only hearing test every 10 years
c) No monitoring is needed
d) Serum uric acid only
Answer: a) Complete blood counts and liver function tests
- Which serious pulmonary adverse effect has been reported with abemaciclib?
a) Interstitial lung disease or pneumonitis
b) Asthma cure
c) Mandatory pulmonary embolism in all patients
d) Acute bacterial pneumonia in every patient
Answer: a) Interstitial lung disease or pneumonitis
- Which adverse event is an important warning with abemaciclib, especially with endocrine therapy?
a) Venous thromboembolism
b) Irreversible cataract
c) Severe ototoxicity
d) Acute opioid withdrawal
Answer: a) Venous thromboembolism
- Which drug is another CDK4/6 inhibitor?
a) Palbociclib
b) Olaparib
c) Trastuzumab
d) Cisplatin
Answer: a) Palbociclib
- Which statement best describes abemaciclib?
a) It blocks CDK4/6, prevents Rb phosphorylation, and inhibits G1-to-S phase progression
b) It directly blocks HER2 receptors in HER2-positive breast cancer
c) It irreversibly inhibits cyclooxygenase
d) It activates dopamine receptors in the basal ganglia
Answer: a) It blocks CDK4/6, prevents Rb phosphorylation, and inhibits G1-to-S phase progression
FAQs
What is the mechanism of action of abemaciclib?
Abemaciclib inhibits CDK4 and CDK6. This prevents phosphorylation of retinoblastoma protein, keeps E2F transcription factors suppressed, blocks G1-to-S phase cell-cycle progression, and reduces cancer cell proliferation.
What is the brand name of abemaciclib?
The brand name of abemaciclib is Verzenio.
Which cancer is abemaciclib used for?
Abemaciclib is used in selected adults with HR-positive, HER2-negative breast cancer, including high-risk early breast cancer and advanced or metastatic breast cancer settings.
Why is abemaciclib combined with endocrine therapy?
HR-positive breast cancer depends on estrogen receptor signaling, which can increase cyclin D and activate CDK4/6. Endocrine therapy reduces estrogen signaling, while abemaciclib blocks downstream CDK4/6-mediated cell-cycle progression.
What is the most characteristic adverse effect of abemaciclib?
Diarrhea is the most characteristic adverse effect. It may occur early and should be treated promptly with antidiarrheal therapy, hydration, and dose adjustment if needed.
Does abemaciclib cause neutropenia?
Yes. Abemaciclib can cause neutropenia, leukopenia, anemia, and thrombocytopenia. Complete blood count monitoring is required during therapy.
How is abemaciclib different from palbociclib?
Both are CDK4/6 inhibitors, but abemaciclib is commonly given continuously and is strongly associated with diarrhea. Palbociclib is commonly given in cycles and is strongly associated with neutropenia.
Can abemaciclib be used during pregnancy?
Abemaciclib can cause fetal harm and should generally be avoided during pregnancy. Females of reproductive potential should use effective contraception according to product guidance.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

