
Table of Contents
Introduction
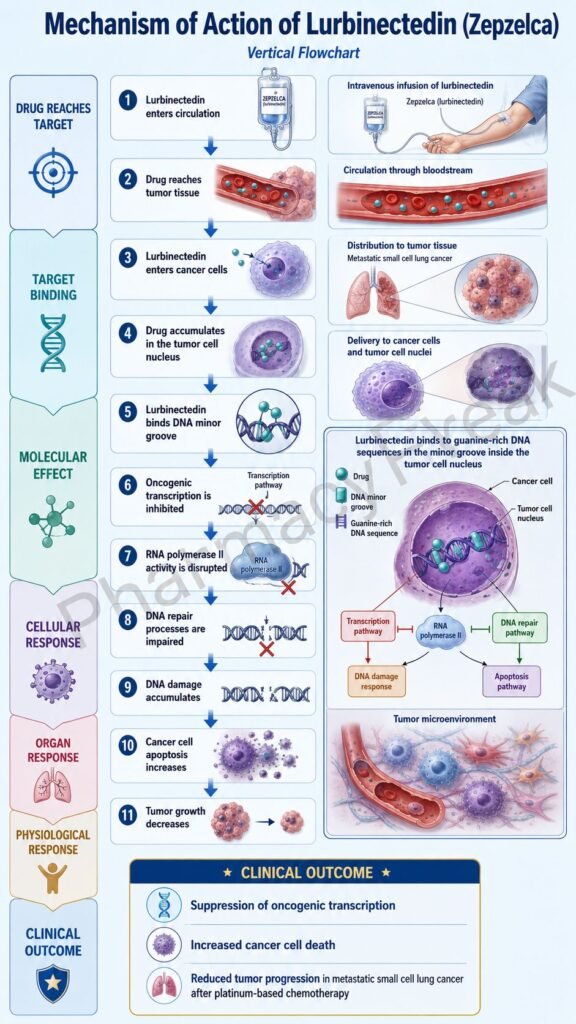
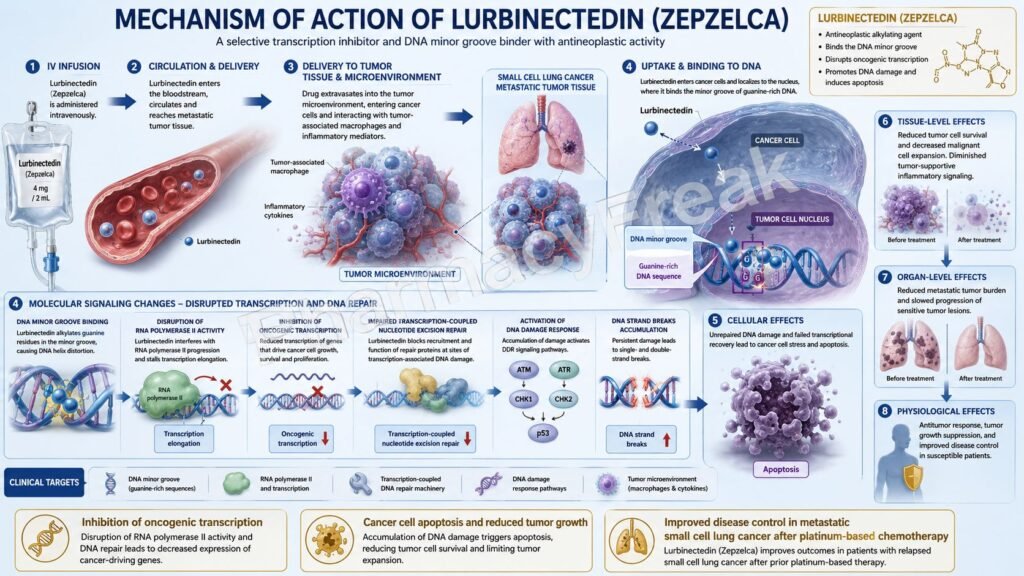
Lurbinectedin is an intravenous anticancer drug marketed under the brand name Zepzelca. It belongs to the class of alkylating antineoplastic agents and is mainly used in small cell lung cancer, a highly aggressive neuroendocrine lung cancer that often responds initially to platinum-based chemotherapy but commonly relapses.
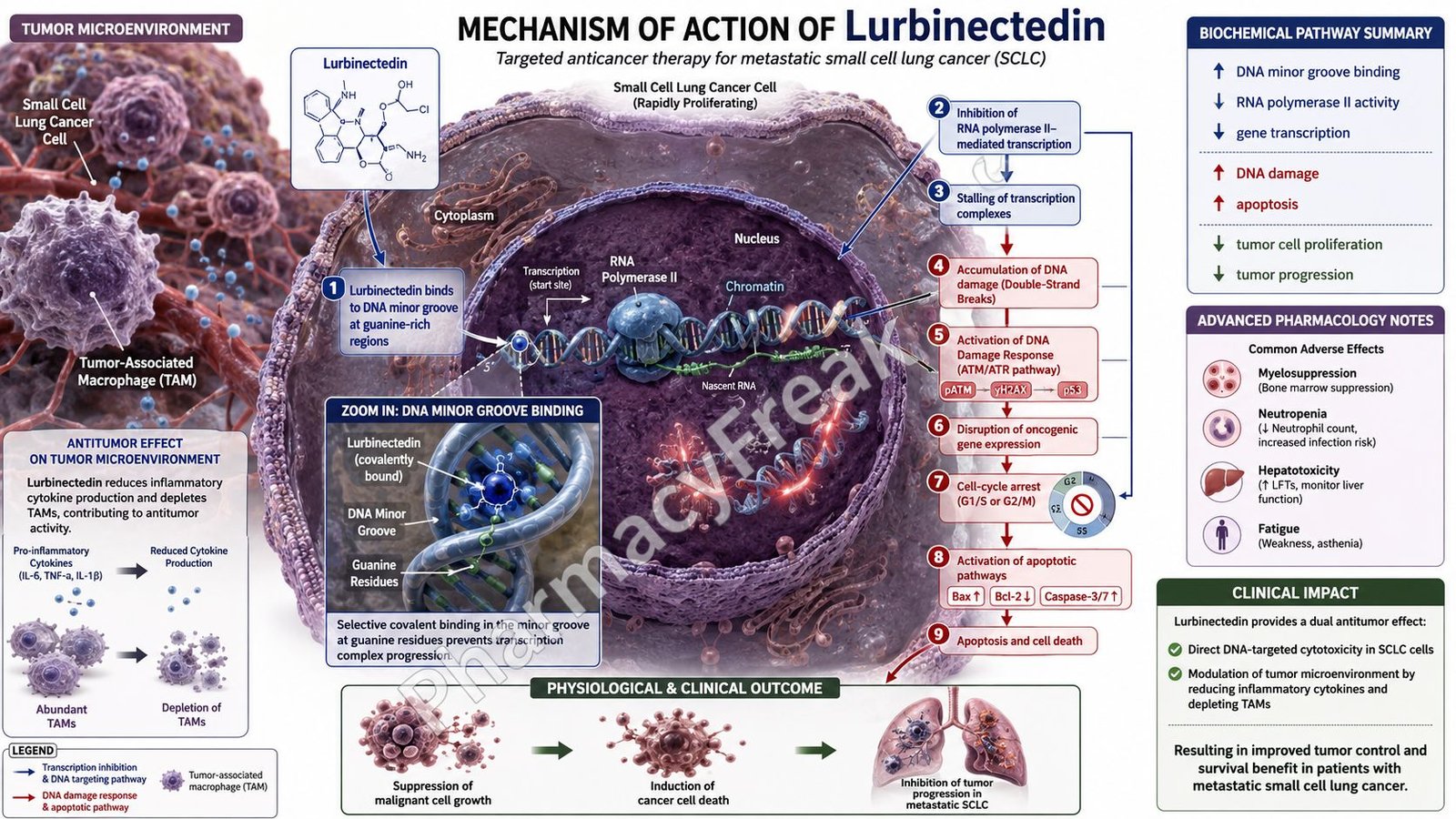
Lurbinectedin is pharmacologically important because it targets DNA structure and transcription. It binds guanine residues in the minor groove of DNA, forms DNA adducts, bends the DNA helix, interferes with DNA-binding proteins and transcription factors, disrupts DNA repair pathways, perturbs the cell cycle, and leads to cancer cell death. The official prescribing information describes lurbinectedin as an alkylating drug that binds guanine residues in the DNA minor groove and causes cell-cycle perturbation and eventual cell death.
Current labeling includes two major small cell lung cancer settings. Zepzelca is used with atezolizumab or atezolizumab/hyaluronidase-tqjs as maintenance treatment for adults with extensive-stage small cell lung cancer whose disease has not progressed after first-line induction therapy with atezolizumab or atezolizumab/hyaluronidase, carboplatin, and etoposide. It is also used as a single agent for adults with metastatic small cell lung cancer whose disease has progressed on or after platinum-based chemotherapy.
For pharmacy, medical, nursing, and competitive exam students, lurbinectedin is important because it connects DNA alkylation, transcription inhibition, DNA repair interference, tumor microenvironment effects, and small cell lung cancer pharmacotherapy. Its key mechanism is DNA minor-groove binding with transcriptional disruption and cell death.
Mechanism of Action (Step-wise)
- Primary target: DNA minor groove
Lurbinectedin targets DNA, especially guanine residues located in the minor groove of DNA. The minor groove is one of the structural grooves of the DNA double helix where some DNA-binding drugs and proteins interact.
By binding in this groove, lurbinectedin changes the normal structure and function of DNA.
- Formation of DNA adducts
Lurbinectedin forms covalent adducts with guanine residues. These DNA adducts distort the DNA helix and interfere with normal DNA processing.
DNA adduct formation is central to the drug’s cytotoxic action because cancer cells depend heavily on DNA replication, transcription, and repair.
- Bending of DNA toward the major groove
After binding to guanine residues, lurbinectedin causes bending of the DNA helix toward the major groove. This conformational distortion affects how proteins interact with DNA.
The label states that lurbinectedin binding forms adducts and bends the DNA helix toward the major groove.
- Interference with DNA-binding proteins
DNA-binding proteins, including transcription factors and repair proteins, need proper DNA structure to recognize and bind specific sequences.
Lurbinectedin-induced DNA adducts disturb this process. As a result, transcription factors and DNA repair proteins cannot function normally.
- Inhibition of oncogenic transcription
Small cell lung cancer cells often depend on high transcriptional activity to maintain rapid growth, survival, and neuroendocrine tumor identity.
Lurbinectedin disrupts transcription by interfering with DNA-protein interactions. This reduces expression of genes required for cancer cell survival and proliferation.
- Interference with DNA repair pathways
DNA repair systems attempt to correct DNA damage and maintain genome stability. Lurbinectedin can perturb DNA repair pathways by creating DNA lesions and interfering with DNA repair protein activity.
When DNA damage cannot be repaired properly, cancer cells accumulate lethal genomic injury.
- Cell-cycle perturbation
DNA damage and transcriptional stress activate cell-cycle checkpoints. Lurbinectedin disrupts normal cell-cycle progression, especially in rapidly dividing tumor cells.
This contributes to growth arrest and prevents cancer cells from completing successful replication and division.
- Induction of cancer cell death
When DNA damage, transcriptional inhibition, and failed repair exceed the cell’s ability to recover, apoptotic and other cell-death pathways are activated.
The final result is death of sensitive tumor cells.
- Effect on tumor microenvironment
Lurbinectedin also has effects beyond direct tumor cell DNA damage. The label notes that lurbinectedin inhibited human monocyte activity in vitro and reduced macrophage infiltration in implanted tumors in mice.
This is important because tumor-associated macrophages can support tumor growth, angiogenesis, immune evasion, and metastatic behavior.
- Final therapeutic effect
The final therapeutic effect of lurbinectedin is DNA minor-groove binding, DNA adduct formation, transcriptional disruption, DNA repair interference, cell-cycle perturbation, tumor cell death, and possible modulation of tumor-associated inflammatory cells.
Pharmacokinetics
Lurbinectedin is administered intravenously as a lyophilized powder for reconstitution. The recommended dosage is 3.2 mg/m² given by intravenous infusion over 60 minutes every 21 days until disease progression or unacceptable toxicity.
Absorption:
Because lurbinectedin is given intravenously, it does not require gastrointestinal absorption. Systemic bioavailability is complete after infusion.
Distribution:
Lurbinectedin distributes extensively into tissues. The steady-state volume of distribution is approximately 504 L. It is highly protein-bound, with about 99% binding to albumin and alpha-1-acid glycoprotein.
Metabolism:
Lurbinectedin is metabolized mainly by CYP3A in vitro. This makes drug interactions clinically important. Strong or moderate CYP3A inhibitors may increase exposure and toxicity, while strong CYP3A inducers may reduce drug exposure and effectiveness. The label recommends avoiding strong or moderate CYP3A inhibitors and strong CYP3A inducers.
Excretion:
After a radiolabeled dose, about 89% of radioactivity is recovered in feces and about 6% in urine. Very little unchanged drug is recovered, showing that metabolism is important before elimination.
Half-life and duration:
The terminal half-life of lurbinectedin is approximately 51 hours. This pharmacokinetic profile supports dosing every 21 days.
Special pharmacokinetic point:
No accumulation of lurbinectedin in plasma is observed with administration every 3 weeks at the approved recommended dosage. Exposure-related increases in grade 4 neutropenia and grade 3 or higher thrombocytopenia have been observed, making dose adjustment and blood count monitoring important.
Clinical Uses
- Extensive-stage small cell lung cancer maintenance therapy:
Lurbinectedin is used with atezolizumab or atezolizumab/hyaluronidase-tqjs for maintenance treatment of adults with extensive-stage small cell lung cancer whose disease has not progressed after first-line induction therapy with atezolizumab or atezolizumab/hyaluronidase, carboplatin, and etoposide. - Metastatic small cell lung cancer after platinum therapy:
Lurbinectedin is used as a single agent for adults with metastatic small cell lung cancer whose disease has progressed on or after platinum-based chemotherapy. This indication was approved under accelerated approval based on overall response rate and duration of response. - DNA-damaging antitumor therapy:
It is used in cancer cells that are sensitive to transcriptional disruption and DNA damage. - Relapsed small cell lung cancer option:
Lurbinectedin is clinically important in relapsed metastatic SCLC because treatment options after platinum-based chemotherapy are limited. - Combination maintenance strategy:
In extensive-stage SCLC, lurbinectedin can be combined with PD-L1 immune checkpoint therapy after induction chemoimmunotherapy when disease has not progressed. - Tumor microenvironment-related effect:
Its potential to reduce monocyte activity and macrophage infiltration may add to its antitumor pharmacology, although the main clinical mechanism remains DNA binding and transcriptional disruption.
Adverse Effects
Common adverse effects and laboratory abnormalities of lurbinectedin include:
- Leukopenia
- Lymphopenia
- Neutropenia
- Anemia
- Thrombocytopenia
- Fatigue
- Nausea
- Vomiting
- Constipation
- Diarrhea
- Decreased appetite
- Musculoskeletal pain
- Dyspnea
- Cough
- Increased creatinine
- Increased ALT
- Increased AST
- Increased glucose
- Decreased albumin
- Decreased sodium
- Decreased magnesium
The label lists the most common adverse reactions and laboratory abnormalities for single-agent Zepzelca as leukopenia, lymphopenia, fatigue, anemia, neutropenia, increased creatinine, increased ALT, increased glucose, thrombocytopenia, nausea, decreased appetite, musculoskeletal pain, decreased albumin, constipation, dyspnea, decreased sodium, increased AST, vomiting, cough, decreased magnesium, and diarrhea.
Important serious or clinically significant adverse effects include:
- Severe myelosuppression
- Febrile neutropenia
- Sepsis
- Thrombocytopenia
- Severe anemia
- Hepatotoxicity
- Extravasation causing tissue necrosis
- Rhabdomyolysis
- Embryo-fetal toxicity
- Serious infections
- Pneumonia
- Dose-limiting neutropenia
Myelosuppression is one of the most important exam points. Zepzelca can cause severe and fatal myelosuppression, including febrile neutropenia, sepsis, thrombocytopenia, and anemia. The label recommends blood count monitoring before each dose and starting therapy only when baseline neutrophils are at least 1,500 cells/mm³ and platelets are at least 100,000/mm³.
Hepatotoxicity is another key safety concern. Liver function tests should be monitored before treatment and periodically during therapy. Dose interruption, reduction, or discontinuation may be needed based on severity.
Extravasation is clinically important because lurbinectedin can cause skin and soft tissue injury, including tissue necrosis requiring debridement. Central venous administration is recommended to reduce this risk, especially in patients with limited venous access.
Rhabdomyolysis has been reported. Creatine phosphokinase should be monitored before starting therapy and periodically during treatment as clinically indicated.
Comparative Analysis
| Feature | Lurbinectedin | Topotecan | Platinum Agents | Etoposide |
|---|---|---|---|---|
| Brand example | Zepzelca | Hycamtin | Cisplatin, carboplatin | Etopophos, generic etoposide |
| Drug class | Alkylating antineoplastic / DNA minor-groove binder | Topoisomerase I inhibitor | Platinum DNA crosslinking agents | Topoisomerase II inhibitor |
| Main target | Guanine residues in DNA minor groove | Topoisomerase I-DNA complex | DNA crosslinks | Topoisomerase II-DNA complex |
| Main action | DNA adducts, transcription disruption, cell-cycle perturbation | Prevents repair of single-strand DNA breaks | Causes DNA crosslinks and apoptosis | Causes double-strand DNA breaks |
| Important SCLC role | ES-SCLC maintenance combination; metastatic SCLC after platinum progression | Relapsed SCLC option | First-line backbone in SCLC | First-line chemotherapy partner |
| Route | Intravenous | Oral or intravenous depending on product | Intravenous | Oral or intravenous depending on product |
| Major toxicity | Myelosuppression, hepatotoxicity, extravasation necrosis, rhabdomyolysis | Myelosuppression, diarrhea | Nephrotoxicity, neuropathy, ototoxicity, myelosuppression | Myelosuppression, hypotension, secondary leukemia |
| Exam point | Binds DNA minor groove and inhibits transcription | Topoisomerase I inhibitor | DNA crosslinking | Topoisomerase II inhibitor |
Lurbinectedin differs from topotecan because it does not primarily inhibit topoisomerase I. It binds DNA in the minor groove and disrupts transcription and DNA repair processes. Platinum agents form DNA crosslinks and are a major first-line backbone in small cell lung cancer. Etoposide inhibits topoisomerase II and is commonly combined with platinum agents in first-line SCLC treatment.
MCQs
- Lurbinectedin is marketed under which brand name?
a) Zepzelca
b) Keytruda
c) Opdivo
d) Taxol
Answer: a) Zepzelca
- Lurbinectedin belongs mainly to which anticancer drug class?
a) Alkylating antineoplastic agent
b) EGFR inhibitor
c) Anti-HER2 monoclonal antibody
d) Aromatase inhibitor
Answer: a) Alkylating antineoplastic agent
- Lurbinectedin primarily binds to:
a) Guanine residues in the minor groove of DNA
b) HER2 receptors on breast cancer cells
c) PD-1 receptors on T cells
d) VEGF in plasma
Answer: a) Guanine residues in the minor groove of DNA
- DNA adduct formation by lurbinectedin causes:
a) Bending of the DNA helix
b) Direct bronchodilation
c) Increased insulin secretion
d) Histamine receptor activation
Answer: a) Bending of the DNA helix
- Lurbinectedin disrupts cancer cell survival mainly by interfering with:
a) DNA binding proteins, transcription factors, and DNA repair pathways
b) Acetylcholine receptors only
c) Gastric acid secretion
d) Sodium-glucose transport only
Answer: a) DNA binding proteins, transcription factors, and DNA repair pathways
- Lurbinectedin is used as a single agent in metastatic SCLC after progression on or after:
a) Platinum-based chemotherapy
b) Insulin therapy
c) Antihistamine therapy
d) Anticoagulant therapy only
Answer: a) Platinum-based chemotherapy
- Lurbinectedin is used in maintenance treatment of ES-SCLC with:
a) Atezolizumab or atezolizumab/hyaluronidase-tqjs
b) Amoxicillin
c) Salbutamol
d) Metformin
Answer: a) Atezolizumab or atezolizumab/hyaluronidase-tqjs
- Lurbinectedin is administered by which route?
a) Intravenous infusion
b) Oral tablet
c) Inhalation
d) Sublingual tablet
Answer: a) Intravenous infusion
- The usual dosing interval for lurbinectedin is:
a) Every 21 days
b) Every 6 hours
c) Once yearly
d) Every morning indefinitely without cycles
Answer: a) Every 21 days
- Which adverse effect is highly important with lurbinectedin?
a) Myelosuppression
b) Gingival hyperplasia
c) Severe ototoxicity as the classic toxicity
d) Hypoglycemia only
Answer: a) Myelosuppression
- Which laboratory monitoring is important before each lurbinectedin dose?
a) Blood counts
b) Visual acuity only
c) Serum amylase only
d) Audiometry only
Answer: a) Blood counts
- Lurbinectedin is mainly metabolized by:
a) CYP3A
b) CYP2D6 only
c) Monoamine oxidase-B
d) Acetylcholinesterase
Answer: a) CYP3A
- Which serious local complication may occur if lurbinectedin extravasates?
a) Tissue necrosis
b) Hair growth
c) Bronchodilation
d) Cataract formation
Answer: a) Tissue necrosis
- Which serious muscle toxicity has been reported with lurbinectedin?
a) Rhabdomyolysis
b) Myasthenia gravis cure
c) Tendon reflex enhancement only
d) Muscle hypertrophy
Answer: a) Rhabdomyolysis
- Which statement about lurbinectedin is correct?
a) It binds DNA minor groove guanine residues, forms adducts, disrupts transcription and DNA repair, and causes cell death
b) It blocks TNF-alpha in rheumatoid arthritis
c) It directly stimulates beta-2 receptors
d) It is a topical corticosteroid
Answer: a) It binds DNA minor groove guanine residues, forms adducts, disrupts transcription and DNA repair, and causes cell death
FAQs
- What is lurbinectedin used for?
Lurbinectedin is used in small cell lung cancer. It is used with atezolizumab or atezolizumab/hyaluronidase-tqjs as maintenance therapy for extensive-stage SCLC after induction therapy when disease has not progressed. It is also used as a single agent in metastatic SCLC that has progressed on or after platinum-based chemotherapy.
- What is the mechanism of action of lurbinectedin?
Lurbinectedin binds guanine residues in the minor groove of DNA, forms DNA adducts, bends the DNA helix, interferes with DNA-binding proteins and transcription factors, disrupts DNA repair pathways, perturbs the cell cycle, and causes cancer cell death.
- Is lurbinectedin chemotherapy?
Yes. Lurbinectedin is an anticancer chemotherapy drug with alkylating-like DNA-binding activity. It is also considered a targeted transcription-disrupting DNA minor-groove binder.
- Why is lurbinectedin useful in small cell lung cancer?
Small cell lung cancer is rapidly proliferative and highly dependent on transcriptional and DNA repair processes. Lurbinectedin damages DNA and disrupts transcription, leading to cancer cell death in sensitive tumors.
- How is lurbinectedin administered?
Lurbinectedin is given as an intravenous infusion over 60 minutes, usually every 21 days, until disease progression or unacceptable toxicity.
- What is the most important toxicity of lurbinectedin?
Myelosuppression is one of the most important toxicities. It can cause neutropenia, thrombocytopenia, anemia, febrile neutropenia, and serious infections.
- Can lurbinectedin cause liver toxicity?
Yes. Lurbinectedin can cause hepatotoxicity. Liver function tests should be monitored before and during treatment.
- Why is central venous administration recommended?
Central venous administration is recommended to reduce the risk of extravasation, which can cause severe skin and soft tissue injury, including tissue necrosis.
- Which drug interactions are important with lurbinectedin?
CYP3A interactions are important. Strong or moderate CYP3A inhibitors can increase lurbinectedin exposure and toxicity, while strong CYP3A inducers can reduce exposure and effectiveness.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

