
Table of Contents
Introduction
Ibrance is the brand name of palbociclib, an oral targeted anticancer drug belonging to the class of cyclin-dependent kinase 4 and 6 inhibitors, commonly called CDK4/6 inhibitors. It is mainly used in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced or metastatic breast cancer.
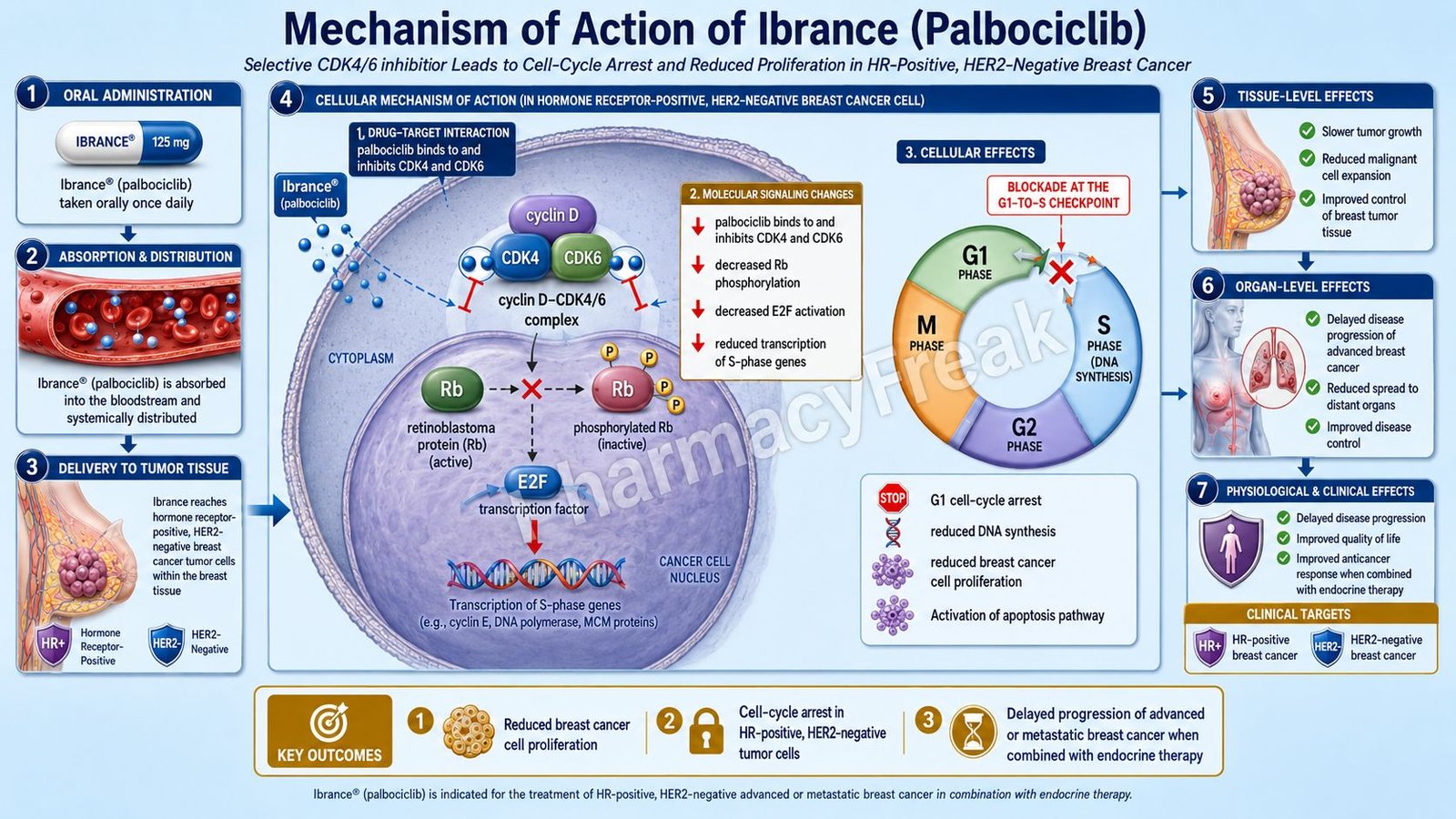
Ibrance is pharmacologically important because it targets a key cell-cycle checkpoint. Cancer cells must pass from the G1 phase into the S phase to replicate DNA and divide. In many hormone receptor-positive breast cancers, cyclin D-CDK4/6 signaling is overactive, allowing tumor cells to keep proliferating. Palbociclib inhibits CDK4 and CDK6, reduces retinoblastoma protein phosphorylation, suppresses E2F-dependent transcription, and arrests cells in the G1 phase.
Current prescribing information states that Ibrance is indicated in adults with HR-positive, HER2-negative advanced or metastatic breast cancer in combination with an aromatase inhibitor as initial endocrine-based therapy, or with fulvestrant after disease progression following endocrine therapy. The label also includes use with inavolisib and fulvestrant for adults with endocrine-resistant, PIK3CA-mutated, HR-positive, HER2-negative locally advanced or metastatic breast cancer after recurrence on or after adjuvant endocrine therapy.
For pharmacy, medical, nursing, and competitive exam students, Ibrance is important because it represents a classic targeted oncology drug. It is not traditional cytotoxic chemotherapy. Its key mechanism is cell-cycle blockade through selective inhibition of CDK4/6.
Mechanism of Action (Step-wise)
- Primary target: CDK4 and CDK6
Ibrance contains palbociclib, which inhibits cyclin-dependent kinases 4 and 6. CDK4 and CDK6 are enzymes that regulate progression through the G1 phase of the cell cycle.
These kinases become active after binding with cyclin D proteins, especially cyclin D1.
- Cyclin D-CDK4/6 normally drives cell-cycle progression
In normal cell-cycle signaling, cyclin D binds CDK4 and CDK6. This complex helps push the cell from the G1 phase into the S phase.
The S phase is the DNA synthesis phase. Once a cell enters S phase, it begins preparing for cell division.
- Role of retinoblastoma protein
Retinoblastoma protein, commonly called Rb protein, is a tumor suppressor that controls cell-cycle progression.
When Rb is active and not phosphorylated, it binds E2F transcription factors and prevents the cell from entering S phase.
- CDK4/6 phosphorylates Rb
The cyclin D-CDK4/6 complex phosphorylates Rb protein. Once Rb is phosphorylated, it releases E2F transcription factors.
Free E2F then activates transcription of genes needed for DNA synthesis and S-phase entry.
- Palbociclib blocks Rb phosphorylation
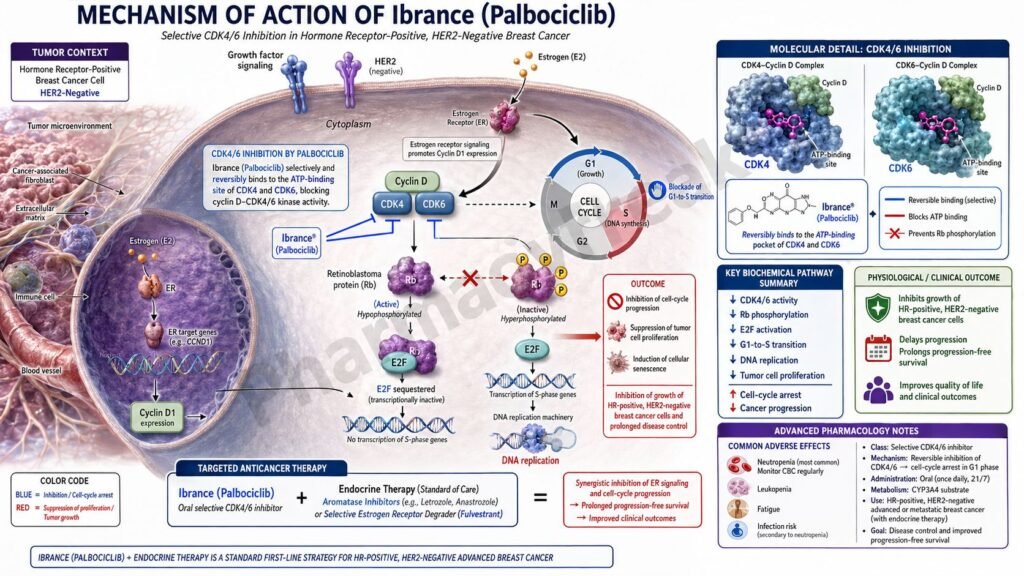
Palbociclib inhibits CDK4/6 activity and decreases phosphorylation of Rb protein. The official label states that palbociclib inhibits CDK4 and CDK6, blocks progression from G1 to S phase in ER-positive breast cancer cell lines, and in combination with antiestrogens decreases Rb phosphorylation, reduces E2F expression and signaling, and increases growth arrest.
- Reduced E2F signaling
When Rb remains unphosphorylated, E2F remains suppressed. This reduces transcription of genes required for DNA replication.
As a result, breast cancer cells cannot efficiently move from the G1 phase into the S phase.
- G1 phase cell-cycle arrest
The main cellular effect of Ibrance is G1 arrest. Tumor cells remain blocked before DNA synthesis.
This slows cancer cell proliferation and delays tumor progression in suitable HR-positive, HER2-negative breast cancers.
- Synergy with endocrine therapy
Hormone receptor-positive breast cancer often depends on estrogen receptor signaling. Endocrine therapies such as aromatase inhibitors and fulvestrant reduce estrogen-driven growth signals.
When palbociclib is combined with endocrine therapy, the combination reduces both hormone-driven signaling and cell-cycle progression. In preclinical models, palbociclib plus antiestrogens produced stronger growth arrest and reduced Rb phosphorylation more than either treatment alone.
- Effect in PIK3CA-mutated endocrine-resistant disease
In some HR-positive, HER2-negative breast cancers, PIK3CA mutations activate PI3K pathway signaling and contribute to endocrine resistance. In the newer combination setting with inavolisib and fulvestrant, Ibrance contributes cell-cycle blockade while the other agents target PI3K-alpha signaling and estrogen receptor signaling.
- Final therapeutic effect
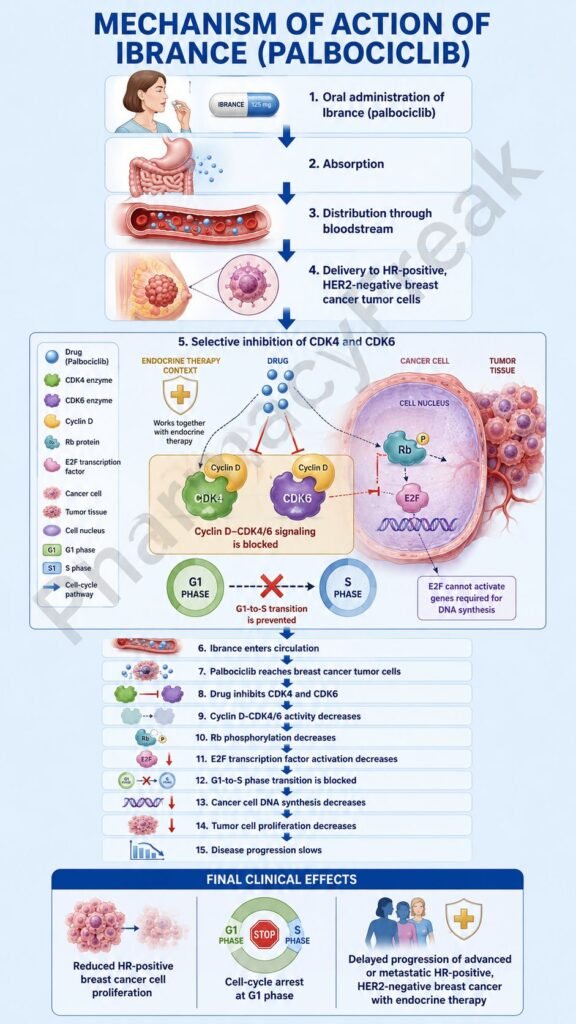
The final therapeutic effect of Ibrance is inhibition of CDK4/6, reduced Rb phosphorylation, reduced E2F-mediated transcription, G1 cell-cycle arrest, decreased tumor cell proliferation, and improved disease control when used with appropriate endocrine or targeted therapy combinations.
Pharmacokinetics
Ibrance is administered orally as palbociclib tablets or capsules. The current tablet dosing schedule is usually 125 mg once daily for 21 consecutive days followed by 7 days off treatment, forming a 28-day cycle. Tablets may be taken with or without food and should be swallowed whole without chewing, crushing, or splitting.
Absorption:
After oral administration of Ibrance tablets, maximum plasma concentration is generally reached within 4 to 12 hours. The mean absolute bioavailability after a 125 mg oral dose is about 46%. Steady state is usually achieved within 8 days of repeated once-daily dosing.
Distribution:
Palbociclib is approximately 85% bound to human plasma proteins. It has a large apparent volume of distribution, showing extensive tissue distribution.
Metabolism:
Palbociclib undergoes hepatic metabolism. CYP3A and sulfotransferase enzyme SULT2A1 are mainly involved in its metabolism. Palbociclib is also a weak time-dependent inhibitor of CYP3A at steady state.
Excretion:
Palbociclib is eliminated mainly through feces. In a radiolabeled dose study, about 74.1% of the dose was recovered in feces and about 17.5% in urine. Most of the recovered material was in the form of metabolites.
Half-life and duration:
The mean plasma elimination half-life of palbociclib is approximately 29 hours in patients with advanced breast cancer. This supports once-daily dosing during the 21-days-on, 7-days-off cycle.
Special pharmacokinetic point:
Strong CYP3A inhibitors can increase palbociclib exposure, while strong CYP3A inducers can significantly reduce exposure. The label recommends avoiding strong CYP3A inhibitors when possible and avoiding strong CYP3A inducers. If a strong CYP3A inhibitor cannot be avoided, dose reduction is recommended.
Clinical Uses
- HR-positive, HER2-negative advanced or metastatic breast cancer:
Ibrance is used in adults with HR-positive, HER2-negative advanced or metastatic breast cancer. - Combination with aromatase inhibitor:
It is used with an aromatase inhibitor as initial endocrine-based therapy in advanced or metastatic disease. - Combination with fulvestrant:
It is used with fulvestrant in patients whose disease has progressed after endocrine therapy. - Combination with inavolisib and fulvestrant:
Ibrance is used with inavolisib and fulvestrant for endocrine-resistant, PIK3CA-mutated, HR-positive, HER2-negative locally advanced or metastatic breast cancer after recurrence on or after adjuvant endocrine therapy, as detected by an FDA-approved test. - Cell-cycle targeted therapy:
Ibrance is used to slow tumor growth by blocking the CDK4/6-Rb-E2F cell-cycle pathway. - Endocrine therapy partner drug:
It is not usually used alone in breast cancer. It is used in combination with endocrine therapy, and in selected patients, with additional targeted therapy.
Adverse Effects
Common adverse effects of Ibrance include:
- Neutropenia
- Leukopenia
- Anemia
- Thrombocytopenia
- Infections
- Fatigue
- Nausea
- Stomatitis
- Diarrhea
- Alopecia
- Rash
- Vomiting
- Decreased appetite
- Dysgeusia
- Increased liver enzymes
- Blood creatinine increased
The label lists common adverse reactions and laboratory abnormalities with Ibrance plus letrozole or fulvestrant, including decreased white blood cell count, decreased neutrophils, decreased hemoglobin, decreased platelets, infections, fatigue, nausea, stomatitis, diarrhea, and alopecia.
Important serious or clinically significant adverse effects include:
- Severe neutropenia
- Febrile neutropenia
- Serious infections
- Interstitial lung disease
- Pneumonitis
- Embryo-fetal toxicity
- Severe myelosuppression
- Dose-limiting hematologic toxicity
Neutropenia is the most important exam point. It was the most frequently reported adverse reaction in PALOMA-2 and PALOMA-3, with grade 3 or higher decreased neutrophil counts reported in 66% of patients receiving Ibrance plus letrozole and 66% receiving Ibrance plus fulvestrant. CBC monitoring is required before starting therapy, at the beginning of each cycle, on day 15 of the first 2 cycles, and as clinically indicated.
Interstitial lung disease and pneumonitis are rare but serious. Severe, life-threatening, or fatal ILD/pneumonitis can occur with CDK4/6 inhibitors, including Ibrance. Patients with new or worsening cough, dyspnea, or hypoxia should be evaluated, and Ibrance should be interrupted if pneumonitis is suspected.
Comparative Analysis
| Feature | Ibrance | Kisqali | Verzenio | Afinitor |
|---|---|---|---|---|
| Generic name | Palbociclib | Ribociclib | Abemaciclib | Everolimus |
| Drug class | CDK4/6 inhibitor | CDK4/6 inhibitor | CDK4/6 inhibitor | mTOR inhibitor |
| Main target | CDK4 and CDK6 | CDK4 and CDK6 | CDK4 and CDK6, relatively more CDK4 activity | mTORC1 |
| Main pathway | Cell-cycle control | Cell-cycle control | Cell-cycle control | PI3K/AKT/mTOR signaling |
| Main breast cancer use | HR+/HER2− advanced or metastatic breast cancer combinations | HR+/HER2− breast cancer combinations | HR+/HER2− breast cancer, including some adjuvant settings | HR+/HER2− breast cancer after endocrine therapy failure with exemestane |
| Key cell-cycle effect | G1 arrest | G1 arrest | G1 arrest | Reduced protein synthesis and growth signaling |
| Major adverse effect | Neutropenia | Neutropenia, QT prolongation, hepatotoxicity | Diarrhea, neutropenia, hepatotoxicity | Stomatitis, hyperglycemia, pneumonitis |
| Dosing style | 21 days on, 7 days off | 21 days on, 7 days off | Continuous dosing in many regimens | Continuous dosing |
Ibrance, Kisqali, and Verzenio are all CDK4/6 inhibitors, but their toxicity profiles differ. Ibrance is especially remembered for neutropenia and the 21-days-on, 7-days-off schedule. Kisqali has important QT prolongation and liver toxicity monitoring. Verzenio is commonly associated with diarrhea and may be dosed continuously. Afinitor is not a CDK4/6 inhibitor; it blocks mTOR signaling downstream in the PI3K/AKT/mTOR pathway.
MCQs
- Ibrance contains which active drug?
a) Ribociclib
b) Palbociclib
c) Abemaciclib
d) Everolimus
Answer: b) Palbociclib
- Ibrance belongs to which drug class?
a) CDK4/6 inhibitor
b) EGFR inhibitor
c) VEGF inhibitor
d) Proteasome inhibitor
Answer: a) CDK4/6 inhibitor
- The main enzymes inhibited by palbociclib are:
a) CDK4 and CDK6
b) COX-1 and COX-2
c) JAK1 and JAK2
d) ACE and renin
Answer: a) CDK4 and CDK6
- Palbociclib blocks progression from:
a) G1 phase to S phase
b) M phase to G1 phase only
c) S phase to G2 phase only
d) G2 phase to M phase only
Answer: a) G1 phase to S phase
- CDK4/6 normally phosphorylates which tumor suppressor protein?
a) Retinoblastoma protein
b) p53 only
c) BRCA1 only
d) HER2 receptor
Answer: a) Retinoblastoma protein
- Reduced Rb phosphorylation leads to reduced activity of:
a) E2F transcription factors
b) Histamine receptors
c) Acetylcholine receptors
d) Beta receptors
Answer: a) E2F transcription factors
- Ibrance is mainly used in which breast cancer subtype?
a) HR-positive, HER2-negative breast cancer
b) HER2-positive breast cancer only
c) Triple-negative breast cancer only
d) Small-cell lung cancer only
Answer: a) HR-positive, HER2-negative breast cancer
- Ibrance is commonly combined with:
a) Aromatase inhibitors or fulvestrant
b) Insulin only
c) Penicillin only
d) Salbutamol only
Answer: a) Aromatase inhibitors or fulvestrant
- Which adverse effect is most exam-important with Ibrance?
a) Neutropenia
b) Ototoxicity
c) Gingival hyperplasia
d) Severe hypoglycemia
Answer: a) Neutropenia
- Which monitoring is especially important during Ibrance therapy?
a) Complete blood count
b) Visual acuity only
c) Serum calcium only
d) Audiometry only
Answer: a) Complete blood count
- Ibrance is mainly metabolized by:
a) CYP3A and SULT2A1
b) CYP2D6 only
c) Acetylcholinesterase
d) Monoamine oxidase-B
Answer: a) CYP3A and SULT2A1
- Strong CYP3A inducers may:
a) Decrease palbociclib exposure
b) Increase insulin secretion
c) Cause direct bronchodilation
d) Increase calcium absorption only
Answer: a) Decrease palbociclib exposure
- Which serious lung toxicity can occur with Ibrance?
a) ILD/pneumonitis
b) Asthma cure
c) Pulmonary surfactant excess
d) Acute pneumothorax from inhalation
Answer: a) ILD/pneumonitis
- Ibrance differs from everolimus because everolimus targets:
a) mTORC1
b) CDK4 only
c) CDK6 only
d) Rb protein directly
Answer: a) mTORC1
- Which statement about Ibrance is correct?
a) It inhibits CDK4/6, reduces Rb phosphorylation, and causes G1 cell-cycle arrest
b) It directly blocks HER2 receptor signaling
c) It is a monoclonal antibody against VEGF
d) It is a rescue medicine for acute bronchospasm
Answer: a) It inhibits CDK4/6, reduces Rb phosphorylation, and causes G1 cell-cycle arrest
FAQs
- What is Ibrance used for?
Ibrance is used in adults with HR-positive, HER2-negative advanced or metastatic breast cancer. It is used in combination with an aromatase inhibitor, fulvestrant, or in selected PIK3CA-mutated endocrine-resistant disease with inavolisib and fulvestrant.
- What is the mechanism of action of Ibrance?
Ibrance contains palbociclib, which inhibits CDK4 and CDK6. This reduces Rb phosphorylation, suppresses E2F signaling, blocks G1-to-S phase transition, and slows breast cancer cell proliferation.
- Is Ibrance chemotherapy?
Ibrance is not traditional cytotoxic chemotherapy. It is a targeted oral CDK4/6 inhibitor that blocks cell-cycle progression.
- Why is Ibrance combined with endocrine therapy?
Hormone receptor-positive breast cancer depends partly on estrogen receptor signaling. Endocrine therapy reduces hormone-driven growth signals, while Ibrance blocks the CDK4/6 cell-cycle pathway. Together, they provide stronger control of tumor proliferation.
- What is the most important side effect of Ibrance?
Neutropenia is the most important and common exam-relevant adverse effect. CBC monitoring is required during therapy.
- Can Ibrance cause lung toxicity?
Yes. Severe, life-threatening, or fatal ILD/pneumonitis can occur with CDK4/6 inhibitors, including Ibrance. New or worsening cough, shortness of breath, or hypoxia requires evaluation.
- How is Ibrance usually taken?
Ibrance is commonly taken once daily for 21 consecutive days followed by 7 days off treatment, making a 28-day cycle.
- Which enzymes metabolize Ibrance?
Palbociclib is mainly metabolized by CYP3A and SULT2A1. Strong CYP3A inhibitors and inducers can significantly affect drug exposure.
- Why does Ibrance cause neutropenia?
CDK4/6 inhibition can affect proliferation of bone marrow precursor cells. This reduces neutrophil production and can lead to neutropenia, although it is often managed with dose interruption or reduction.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

