
Table of Contents
Introduction
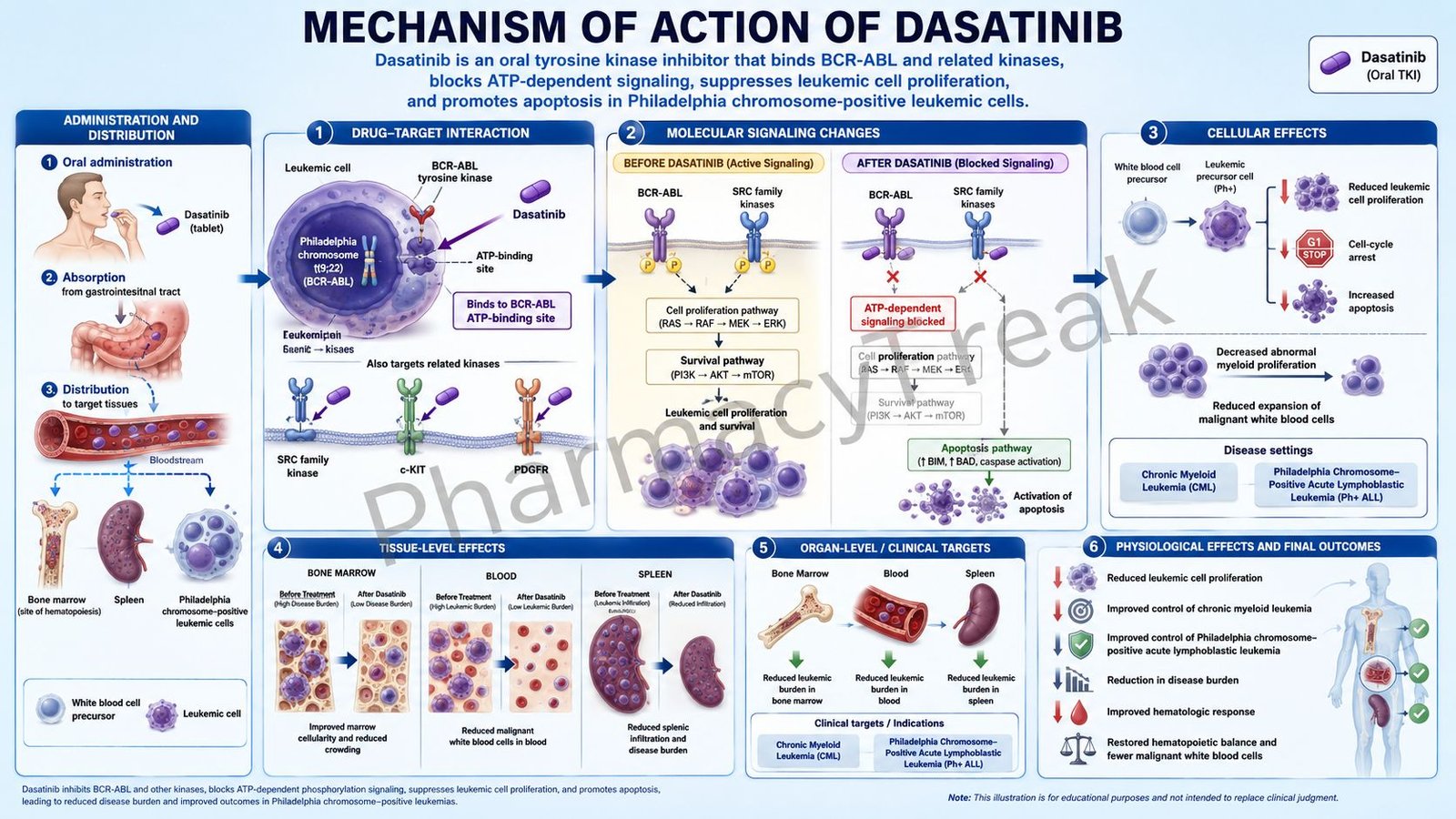
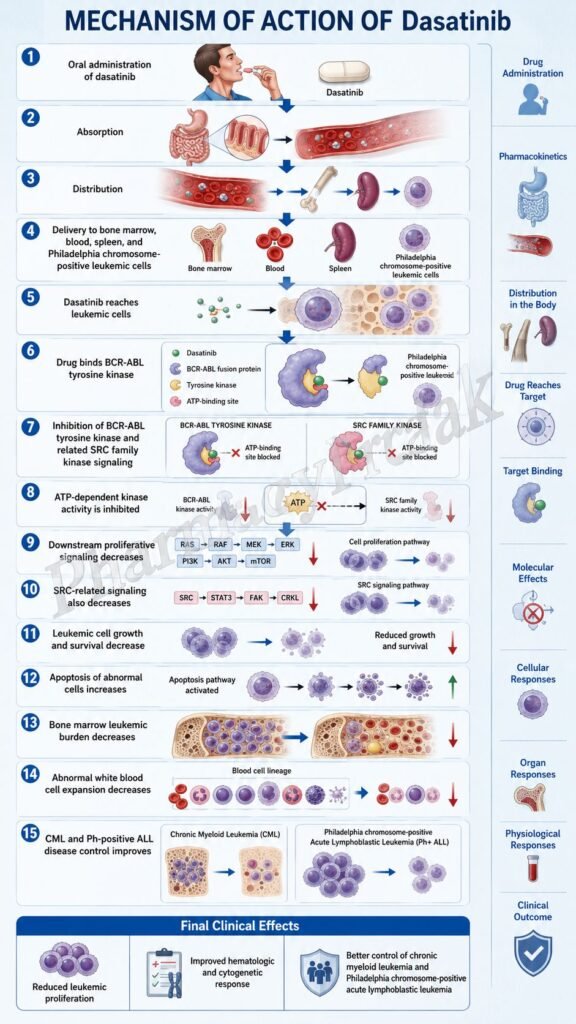
Dasatinib is an oral targeted anticancer drug belonging to the class of tyrosine kinase inhibitors. It is best known by the brand name Sprycel and is mainly used in Philadelphia chromosome-positive leukemias, especially chronic myeloid leukemia and Philadelphia chromosome-positive acute lymphoblastic leukemia.
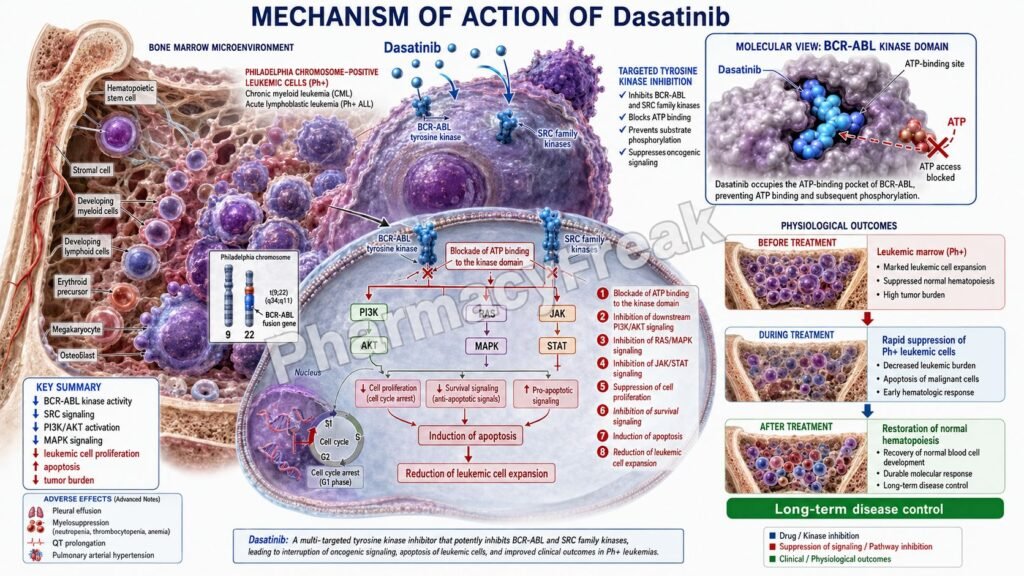
The Philadelphia chromosome results from a translocation between chromosomes 9 and 22, creating the BCR-ABL fusion gene. This gene produces an abnormal BCR-ABL tyrosine kinase that remains continuously active. The abnormal kinase drives uncontrolled proliferation, reduced apoptosis, and survival of leukemic cells.
Dasatinib is important in pharmacology because it inhibits BCR-ABL and several other kinases, including Src family kinases. It is more potent than imatinib against many BCR-ABL-dependent leukemic cells and can act against several imatinib-resistant BCR-ABL kinase domain mutations. Current labeling describes dasatinib as inhibiting BCR-ABL, SRC family kinases, c-KIT, EPHA2, and PDGFRβ at nanomolar concentrations. It is indicated in adults with newly diagnosed Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase, adults with Ph+ CML resistant or intolerant to prior therapy including imatinib, and adults with Ph+ acute lymphoblastic leukemia resistant or intolerant to prior therapy.
For pharmacy, medical, nursing, and competitive exam students, dasatinib is an important example of targeted oncology therapy. It does not act like conventional chemotherapy. Instead, it blocks abnormal kinase signaling that is essential for leukemic cell growth and survival.
Mechanism of Action (Step-wise)
- Primary target: BCR-ABL tyrosine kinase
Dasatinib primarily inhibits BCR-ABL, the abnormal tyrosine kinase produced by the Philadelphia chromosome. BCR-ABL activates multiple intracellular signaling pathways that promote leukemic cell proliferation and survival.
- ATP-competitive kinase inhibition
Dasatinib binds to the ATP-binding site of BCR-ABL kinase. By competing with ATP, it prevents phosphorylation of downstream substrate proteins.
Phosphorylation is essential for transmitting growth and survival signals inside leukemic cells. When dasatinib blocks this process, BCR-ABL-driven signaling is suppressed.
- Inhibition of downstream signaling pathways
BCR-ABL activates several pathways, including RAS/MAPK, PI3K/AKT, and JAK/STAT signaling. These pathways promote cell-cycle progression, survival, resistance to apoptosis, and abnormal myeloid proliferation.
Dasatinib reduces activation of these pathways by blocking the upstream kinase activity of BCR-ABL.
- Inhibition of Src family kinases
Dasatinib also inhibits Src family kinases, including SRC, LCK, YES, and FYN. Src family kinases can contribute to leukemic cell signaling, disease progression, and resistance mechanisms. The label notes that dasatinib can overcome some imatinib resistance mechanisms involving Src family kinases such as LYN and HCK.
- Activity against imatinib-sensitive and some imatinib-resistant disease
Dasatinib is active against leukemic cell lines representing both imatinib-sensitive and imatinib-resistant disease. It can inhibit many BCR-ABL kinase domain mutations that reduce response to imatinib. However, it is not effective against all resistance mutations, and the T315I mutation is a classic example of resistance to several earlier BCR-ABL inhibitors.
- Inhibition of other kinases
Dasatinib also inhibits c-KIT, EPHA2, and PDGFRβ. These kinases may contribute to signaling in some malignant cells, although BCR-ABL inhibition is the central therapeutic mechanism in Ph-positive leukemias.
- Effect on leukemic cells
By blocking BCR-ABL and related kinase signaling, dasatinib reduces proliferation of leukemic cells, promotes apoptosis, and decreases survival of malignant hematopoietic cells.
- Final therapeutic effect
The final therapeutic effect of dasatinib is inhibition of abnormal BCR-ABL-driven signaling, reduced leukemic cell proliferation, increased apoptosis of leukemic cells, hematologic response, cytogenetic response, and molecular response in suitable patients with Ph-positive CML or Ph-positive ALL.
Pharmacokinetics
Dasatinib is administered orally as tablets. It is usually taken once daily, with or without food. Tablets should be swallowed whole and should not be crushed, cut, or chewed. The adult starting dose is commonly 100 mg once daily for chronic phase CML and 140 mg once daily for accelerated phase CML, blast phase CML, or Ph+ ALL.
Absorption:
Dasatinib is rapidly absorbed after oral administration. Maximum plasma concentrations are generally observed between 0.5 and 6 hours after dosing. A high-fat meal increases mean exposure modestly, but dasatinib can be taken with or without food.
Distribution:
Dasatinib has extensive tissue distribution. It is approximately 96% bound to human plasma proteins, and its active metabolite is approximately 93% protein-bound. Dasatinib is also a P-glycoprotein substrate in vitro.
Metabolism:
Dasatinib is metabolized mainly by CYP3A4. Other pathways, including flavin-containing monooxygenase 3 and UGT enzymes, also contribute to metabolite formation. Strong CYP3A4 inhibitors can increase dasatinib exposure, while strong CYP3A4 inducers can reduce exposure.
Excretion:
Dasatinib is eliminated mainly through feces. After a radiolabeled oral dose, about 85% of radioactivity is recovered in feces and about 4% in urine within 10 days. Unchanged dasatinib accounts for about 19% of the dose in feces and only about 0.1% in urine.
Half-life and duration:
The mean terminal half-life of dasatinib is approximately 3 to 5 hours. Despite this short plasma half-life, its strong kinase inhibition supports once-daily dosing in approved regimens.
Special pharmacokinetic point:
Gastric acid-reducing agents can significantly reduce dasatinib exposure. Proton pump inhibitors and H2 blockers may reduce absorption, and antacids should be separated from dasatinib dosing. Grapefruit juice should be avoided because it can increase dasatinib levels through CYP3A4 inhibition.
Clinical Uses
- Newly diagnosed Ph-positive chronic phase CML:
Dasatinib is used in adults with newly diagnosed Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase. It helps suppress BCR-ABL-driven leukemic cell growth. - Imatinib-resistant or imatinib-intolerant CML:
Dasatinib is used in adults with chronic, accelerated, myeloid blast, or lymphoid blast phase Ph+ CML who are resistant or intolerant to prior therapy including imatinib. - Philadelphia chromosome-positive acute lymphoblastic leukemia:
Dasatinib is used in adults with Ph+ ALL who are resistant or intolerant to prior therapy. - Pediatric Ph-positive CML:
Pediatric use information for Sprycel includes Ph+ CML in chronic phase in patients 1 year of age and older, although some generic labels may not include pediatric details because of marketing exclusivity language. - Pediatric Ph-positive ALL with chemotherapy:
Dasatinib has pediatric use in newly diagnosed Ph+ ALL in combination with chemotherapy under Sprycel labeling. - Targeted therapy for BCR-ABL-positive leukemias:
Dasatinib is clinically useful because it directly targets the oncogenic kinase driver in Philadelphia chromosome-positive leukemias.
Adverse Effects
Common adverse effects of dasatinib include:
- Diarrhea
- Fatigue
- Headache
- Nausea
- Rash
- Myalgia
- Dyspnea
- Edema
- Abdominal pain
- Musculoskeletal pain
- Fever
- Cough
- Vomiting
- Infection
- Anorexia
Important serious adverse effects include:
- Myelosuppression
- Neutropenia
- Thrombocytopenia
- Anemia
- Serious bleeding
- Fluid retention
- Pleural effusion
- Pericardial effusion
- Pulmonary edema
- Pulmonary arterial hypertension
- QT prolongation
- Congestive heart failure or cardiac dysfunction
- Severe skin reactions
- Tumor lysis syndrome
- Hepatotoxicity
- Embryo-fetal toxicity
- Growth and development effects in children
Myelosuppression is one of the most important exam points. Dasatinib can cause anemia, neutropenia, and thrombocytopenia, so complete blood count monitoring is required. The patient information section specifically warns that low blood cell counts are common and can be severe.
Pleural effusion is another highly important adverse effect. Dasatinib can cause fluid retention, including pleural effusion, pericardial effusion, pulmonary edema, and generalized edema. Serious pleural effusion has been reported in clinical studies.
Pulmonary arterial hypertension is a distinctive serious toxicity of dasatinib. It can occur at any time during treatment and requires evaluation if patients develop unexplained dyspnea, fatigue, or fluid retention.
Comparative Analysis
| Feature | Dasatinib | Imatinib | Nilotinib | Ponatinib |
|---|---|---|---|---|
| Drug class | BCR-ABL/Src tyrosine kinase inhibitor | BCR-ABL tyrosine kinase inhibitor | BCR-ABL tyrosine kinase inhibitor | BCR-ABL tyrosine kinase inhibitor |
| Generation | Second-generation TKI | First-generation TKI | Second-generation TKI | Third-generation TKI |
| Main target | BCR-ABL, Src family kinases, c-KIT, PDGFRβ | BCR-ABL, c-KIT, PDGFR | BCR-ABL | BCR-ABL including T315I |
| Main use | Ph+ CML, Ph+ ALL | Ph+ CML, GIST, others | Ph+ CML | Resistant Ph+ leukemias, especially T315I mutation |
| Activity in imatinib resistance | Active against many resistant mutations | Limited | Active against many mutations | Active against T315I |
| Route | Oral | Oral | Oral | Oral |
| Key adverse effect | Pleural effusion, myelosuppression | Edema, muscle cramps, GI upset | QT prolongation, metabolic effects | Arterial thrombosis, hypertension |
| Food issue | Can be taken with or without food | Usually with food and water | Empty stomach dosing | With or without food |
Dasatinib differs from imatinib because it is more potent against BCR-ABL and also inhibits Src family kinases. Nilotinib is another second-generation BCR-ABL inhibitor but has a stronger QT and metabolic monitoring focus. Ponatinib is important for resistant disease involving the T315I mutation, but it has a major arterial occlusive event risk. Dasatinib is especially remembered for pleural effusion and pulmonary arterial hypertension.
MCQs
- Dasatinib belongs to which drug class?
a) Alkylating agent
b) Tyrosine kinase inhibitor
c) Antimetabolite
d) Proteasome inhibitor
Answer: b) Tyrosine kinase inhibitor
- The main oncogenic kinase inhibited by dasatinib in CML is:
a) BCR-ABL
b) EGFR
c) HER2
d) ALK
Answer: a) BCR-ABL
- Dasatinib is especially used in leukemias associated with:
a) Philadelphia chromosome
b) Philadelphia negative karyotype only
c) BRCA mutation only
d) KRAS mutation only
Answer: a) Philadelphia chromosome
- The Philadelphia chromosome creates which fusion gene?
a) BCR-ABL
b) PML-RARA
c) EML4-ALK
d) TEL-AML1 only
Answer: a) BCR-ABL
- Dasatinib blocks kinase signaling by competing with:
a) ATP
b) DNA
c) Folate
d) Calcium
Answer: a) ATP
- Which Src family kinase is inhibited by dasatinib?
a) LCK
b) COX-2
c) ACE
d) Aromatase
Answer: a) LCK
- Which disease is commonly treated with dasatinib?
a) Philadelphia chromosome-positive CML
b) Type 1 diabetes mellitus
c) Acute bacterial pneumonia
d) Malaria
Answer: a) Philadelphia chromosome-positive CML
- Dasatinib is also used in:
a) Philadelphia chromosome-positive acute lymphoblastic leukemia
b) Acute appendicitis
c) Hypertensive emergency
d) Rheumatic fever
Answer: a) Philadelphia chromosome-positive acute lymphoblastic leukemia
- Which adverse effect is strongly associated with dasatinib?
a) Pleural effusion
b) Severe ototoxicity
c) Gingival hyperplasia
d) Hypoglycemia
Answer: a) Pleural effusion
- Which blood toxicity is important with dasatinib?
a) Myelosuppression
b) Polycythemia only
c) Thrombocytosis only
d) Eosinophilia only
Answer: a) Myelosuppression
- Dasatinib is mainly metabolized by:
a) CYP3A4
b) CYP2D6
c) Acetylcholinesterase
d) Monoamine oxidase-B
Answer: a) CYP3A4
- Which drug or food product should generally be avoided because it may increase dasatinib levels?
a) Grapefruit juice
b) Oral rehydration solution
c) Vitamin C
d) Lactulose
Answer: a) Grapefruit juice
- Which condition is a distinctive serious pulmonary adverse effect of dasatinib?
a) Pulmonary arterial hypertension
b) Asthma cure
c) Bronchodilation
d) Pneumothorax from inhalation
Answer: a) Pulmonary arterial hypertension
- Dasatinib differs from imatinib because dasatinib also inhibits:
a) Src family kinases
b) Beta receptors
c) Insulin receptors
d) Histamine H1 receptors
Answer: a) Src family kinases
- Which statement about dasatinib is correct?
a) It inhibits BCR-ABL and Src family kinases, reducing leukemic cell proliferation
b) It directly replaces insulin
c) It blocks bacterial cell wall synthesis
d) It is a rescue bronchodilator
Answer: a) It inhibits BCR-ABL and Src family kinases, reducing leukemic cell proliferation
FAQs
- What is dasatinib used for?
Dasatinib is used for Philadelphia chromosome-positive chronic myeloid leukemia and Philadelphia chromosome-positive acute lymphoblastic leukemia in selected adult and pediatric patients.
- What is the mechanism of action of dasatinib?
Dasatinib inhibits BCR-ABL tyrosine kinase and Src family kinases. This blocks abnormal phosphorylation signaling, reduces leukemic cell proliferation, and promotes apoptosis of Ph-positive leukemic cells.
- Is dasatinib chemotherapy?
Dasatinib is not traditional cytotoxic chemotherapy. It is a targeted tyrosine kinase inhibitor used in BCR-ABL-positive leukemias.
- Why is dasatinib useful in CML?
CML is commonly driven by the BCR-ABL fusion kinase. Dasatinib blocks this abnormal kinase and reduces the growth and survival of leukemic cells.
- Can dasatinib work after imatinib failure?
Yes. Dasatinib can work in many patients with imatinib resistance or intolerance. However, some mutations such as T315I may require other agents such as ponatinib.
- What are common side effects of dasatinib?
Common side effects include diarrhea, fatigue, headache, nausea, rash, muscle pain, dyspnea, edema, and abdominal discomfort.
- What is the most important pulmonary adverse effect of dasatinib?
Pleural effusion is a major adverse effect. Pulmonary arterial hypertension is another serious but less common pulmonary toxicity.
- Why should blood counts be monitored during dasatinib therapy?
Dasatinib can cause myelosuppression, including anemia, neutropenia, and thrombocytopenia. Regular complete blood count monitoring helps detect and manage these toxicities.
- Can dasatinib be taken with food?
Yes. Dasatinib may be taken with or without food, but tablets should be swallowed whole and not crushed, cut, or chewed.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

