
Table of Contents
Introduction
Cladribine is a purine nucleoside analogue used as an immunosuppressive and antineoplastic drug. It is available under important brand names such as Mavenclad for relapsing forms of multiple sclerosis and Leustatin for hairy cell leukemia. Pharmacologically, cladribine is an adenosine analogue that is resistant to degradation by adenosine deaminase, allowing it to persist inside susceptible cells and produce cytotoxic effects.
Cladribine is especially important in pharmacology because it selectively affects lymphocytes and monocytes more than many other cells. This selective toxicity is useful in diseases where abnormal lymphocytes are involved, such as hairy cell leukemia, and in autoimmune diseases such as multiple sclerosis, where autoreactive lymphocytes contribute to inflammation and tissue damage.
For exam purposes, cladribine should be remembered as a chlorinated purine nucleoside analogue that is taken up into lymphocytes, converted intracellularly into active nucleotide metabolites, incorporated into DNA, and causes DNA strand breaks, impaired DNA repair, mitochondrial dysfunction, and apoptosis. In multiple sclerosis, its therapeutic benefit is mainly due to depletion and later immune reconstitution of lymphocyte populations, reducing autoimmune attack on the central nervous system.
Mechanism of Action (Step-wise)
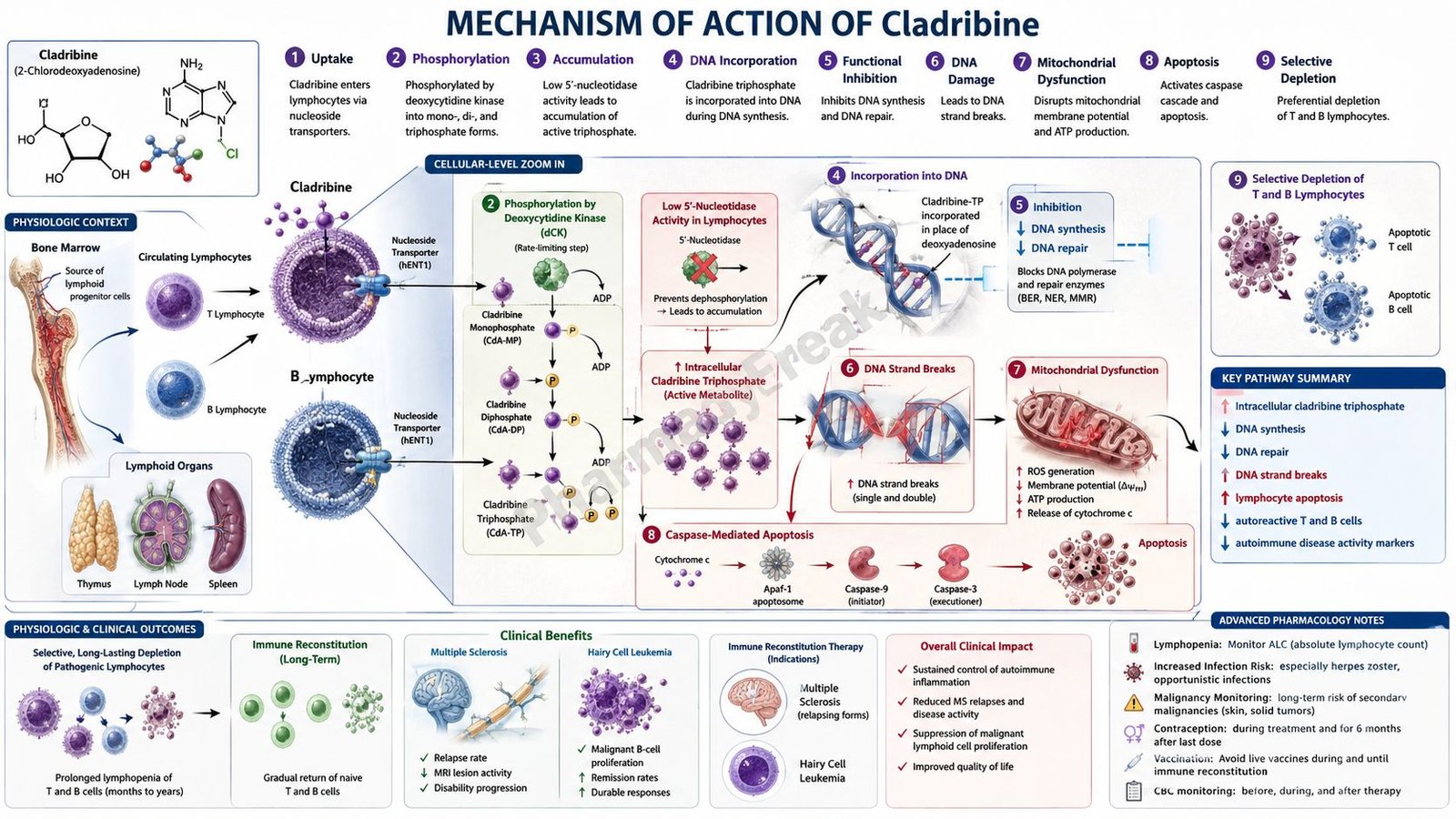
Step 1: Cladribine enters target cells
Cladribine enters cells mainly through nucleoside transporters. It is taken up especially by lymphocytes and monocytes, which are highly sensitive to its effects. This selective accumulation is a major reason why cladribine is useful in lymphocyte-driven disorders.
Step 2: It resists degradation by adenosine deaminase
Normal deoxyadenosine can be metabolized by adenosine deaminase. Cladribine is structurally modified by chlorination, making it resistant to adenosine deaminase breakdown. Because of this resistance, cladribine remains available for intracellular activation.
Step 3: Cladribine is phosphorylated by deoxycytidine kinase
Inside the cell, cladribine is phosphorylated by the enzyme deoxycytidine kinase. It is converted first to cladribine monophosphate and then to active phosphorylated metabolites, especially cladribine triphosphate.
Step 4: Active metabolites accumulate in lymphocytes
Lymphocytes have relatively high deoxycytidine kinase activity and relatively low 5′-nucleotidase activity. Deoxycytidine kinase activates cladribine, while 5′-nucleotidase would normally remove phosphate groups and inactivate nucleotide metabolites. This enzyme balance causes active cladribine metabolites to accumulate preferentially in lymphocytes.
Step 5: Cladribine triphosphate interferes with DNA synthesis
The active triphosphate metabolite interferes with DNA synthesis by being incorporated into DNA and by inhibiting normal DNA polymerase activity. This disrupts DNA chain elongation and prevents proper DNA replication.
Step 6: DNA strand breaks and defective DNA repair occur
Cladribine causes DNA strand breaks and impairs DNA repair mechanisms. This is especially damaging to lymphocytes because they are highly dependent on controlled DNA metabolism for survival, activation, and proliferation.
Step 7: Ribonucleotide reductase inhibition contributes to cytotoxicity
Cladribine metabolites may also inhibit ribonucleotide reductase, an enzyme needed for deoxyribonucleotide production. Reduced deoxyribonucleotide availability further impairs DNA synthesis and repair.
Step 8: Mitochondrial injury and energy depletion occur
Accumulation of toxic nucleotide metabolites can damage mitochondrial function. DNA damage activates repair pathways that consume cellular energy stores such as NAD and ATP. This energy depletion contributes to cell death.
Step 9: Apoptosis of lymphocytes and malignant cells occurs
The final cellular effect is apoptosis, or programmed cell death. Cladribine is toxic to both dividing and resting lymphocytes, which makes it effective in indolent lymphoid malignancies such as hairy cell leukemia and in immune-mediated diseases such as multiple sclerosis.
Step 10: In multiple sclerosis, immune reconstitution reduces inflammation
In relapsing multiple sclerosis, cladribine reduces numbers of lymphocytes, especially B cells and T cells involved in autoimmune inflammation. After depletion, the immune system gradually reconstitutes with a less inflammatory profile. This reduces immune-mediated attack on myelin and axons in the central nervous system, lowering relapse activity and disability progression risk in appropriate patients.
Step 11: In hairy cell leukemia, malignant B-cell burden decreases
Hairy cell leukemia is a chronic B-cell malignancy. Cladribine accumulates in these abnormal lymphoid cells, damages DNA, and induces apoptosis. This reduces malignant cell burden in the bone marrow, spleen, and blood, improving cytopenias such as anemia, neutropenia, and thrombocytopenia.
Pharmacokinetics
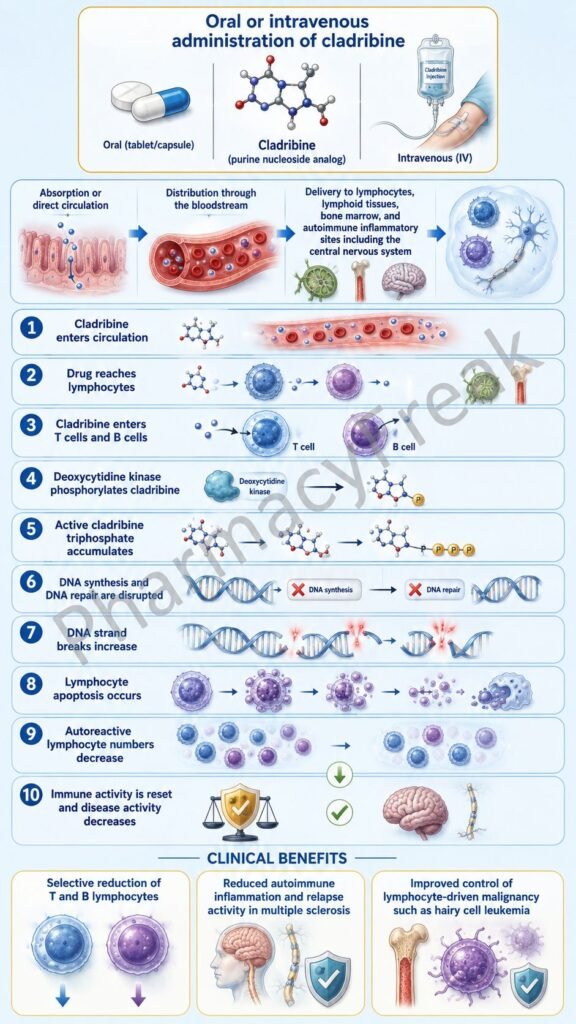
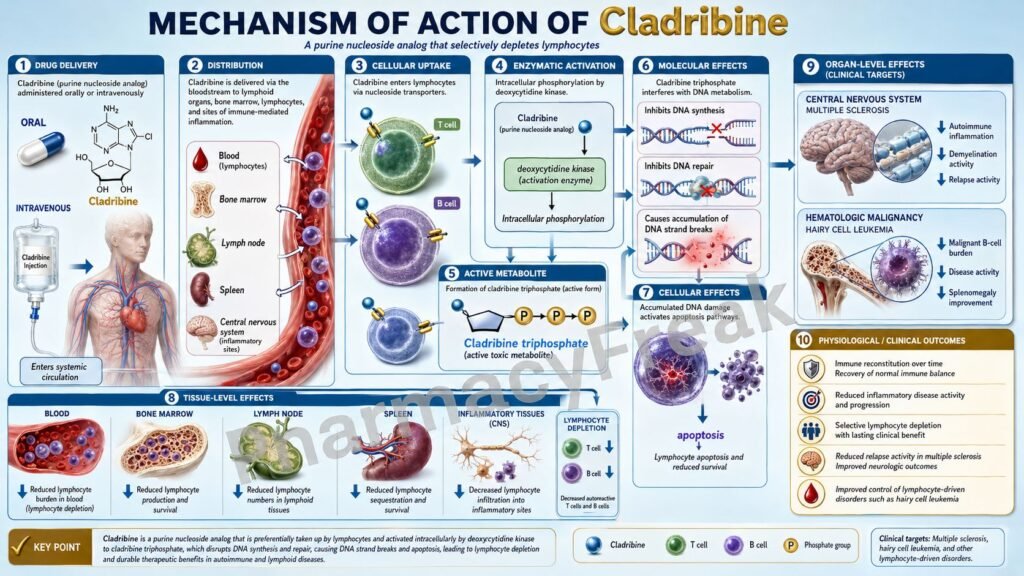
Cladribine is available in different formulations depending on indication. Oral cladribine tablets are used for relapsing forms of multiple sclerosis under the brand name Mavenclad. Intravenous cladribine injection has been used for hairy cell leukemia under the brand name Leustatin or as generic cladribine injection.
After oral administration, cladribine is absorbed systemically and distributed into tissues, including lymphoid cells. Food may affect absorption to some extent, so administration instructions should be followed according to the prescribed product.
Cladribine is not extensively metabolized by cytochrome P450 enzymes. Its most important activation step occurs intracellularly through phosphorylation by deoxycytidine kinase. This is why enzyme activity inside lymphocytes is central to both its pharmacokinetics and pharmacodynamics.
Elimination occurs through both renal and non-renal pathways. Because renal clearance contributes to elimination, impaired kidney function can increase exposure. For oral cladribine used in multiple sclerosis, significant renal impairment is an important safety concern, and use is generally avoided or not recommended in moderate to severe renal impairment.
The pharmacodynamic effect lasts longer than the plasma presence of the drug because lymphocyte depletion and immune reconstitution occur over weeks to months. This explains why oral cladribine for multiple sclerosis is given in short treatment courses rather than as continuous daily therapy.
Clinical Uses
Cladribine is used in relapsing forms of multiple sclerosis in adults, including relapsing-remitting multiple sclerosis and active secondary progressive multiple sclerosis. Because of its safety profile, it is generally reserved for patients who have had an inadequate response to, or cannot tolerate, another drug used for multiple sclerosis.
Cladribine is also used in active hairy cell leukemia. In this disease, it helps reduce malignant B lymphocytes and improves bone marrow function, leading to recovery of blood counts in many patients.
In multiple sclerosis, cladribine is not used as a general first-line drug for every patient. It is selected carefully because it can cause prolonged lymphopenia, infections, malignancy risk concerns, and fetal harm. Before treatment, clinicians evaluate infection status, pregnancy status, blood counts, liver function, kidney function, and immunization history.
In oncology practice, cladribine may also be considered in specialist-managed hematologic conditions beyond classic hairy cell leukemia, but its core approved and exam-relevant uses are relapsing multiple sclerosis and hairy cell leukemia.
Adverse Effects
The most important adverse effect of cladribine is lymphopenia. Since the drug selectively reduces lymphocytes, patients become more vulnerable to infections. Serious infections can occur, including herpes zoster and other opportunistic infections in susceptible patients.
Bone marrow suppression is an important adverse effect, especially with injectable cladribine used in hematologic malignancy. Neutropenia, anemia, thrombocytopenia, and pancytopenia may occur. Regular blood count monitoring is essential.
Cladribine carries an important malignancy warning, especially for oral cladribine used in multiple sclerosis. It should not be used in patients with current malignancy, and patients require appropriate cancer screening before and after treatment.
Fetal harm is a major safety warning. Cladribine is contraindicated in pregnancy. Both females and males of reproductive potential must follow effective contraception guidance during treatment and for the recommended period after the last dose.
Other adverse effects include headache, nausea, fatigue, rash, fever, injection-related reactions with parenteral therapy, alopecia, liver enzyme abnormalities, and hypersensitivity reactions.
Cladribine should not be used in patients with active chronic infections such as active tuberculosis or hepatitis. It is also contraindicated in patients with HIV infection because of the risk of further immune suppression.
Live or live-attenuated vaccines should generally be avoided during and after cladribine treatment until immune recovery is adequate. Vaccination status should be reviewed before starting therapy.
Comparative Analysis
Cladribine is often compared with other disease-modifying therapies used in multiple sclerosis, such as interferon beta, glatiramer acetate, fingolimod, dimethyl fumarate, natalizumab, ocrelizumab, and alemtuzumab. Unlike continuous daily or weekly therapies, oral cladribine is given in short treatment courses and produces a longer-lasting immune reconstitution effect.
Compared with interferon beta and glatiramer acetate, cladribine has a stronger lymphocyte-depleting effect and greater immunosuppressive risk. Interferon beta and glatiramer acetate are generally considered less broadly immunosuppressive but may be less potent in highly active disease.
Compared with fingolimod, cladribine does not mainly trap lymphocytes in lymph nodes. Fingolimod is a sphingosine-1-phosphate receptor modulator that prevents lymphocyte egress from lymphoid tissue. Cladribine directly depletes lymphocytes through intracellular nucleotide toxicity and apoptosis.
Compared with ocrelizumab, cladribine affects both B cells and T cells, while ocrelizumab is a monoclonal antibody that selectively targets CD20-positive B cells. Both can reduce relapse activity in multiple sclerosis, but their mechanisms and monitoring requirements differ.
Compared with alemtuzumab, cladribine is generally considered a selective immune reconstitution therapy with important but different safety concerns. Alemtuzumab targets CD52 and causes profound lymphocyte depletion with risks of autoimmune thyroid disease, immune thrombocytopenia, nephropathy, and infusion reactions.
In hairy cell leukemia, cladribine is commonly compared with pentostatin. Both are purine analogue drugs used in hairy cell leukemia. Pentostatin inhibits adenosine deaminase, while cladribine is resistant to adenosine deaminase and acts after intracellular phosphorylation. Both can produce durable remissions, but dosing schedules, toxicity profiles, and institutional preferences differ.
MCQs
- Cladribine belongs to which pharmacological class?
a) Purine nucleoside analogue
b) Beta-lactam antibiotic
c) Direct thrombin inhibitor
d) Calcium channel blocker
Answer: a) Purine nucleoside analogue
- Mavenclad contains which active drug?
a) Fingolimod
b) Cladribine
c) Ocrelizumab
d) Dimethyl fumarate
Answer: b) Cladribine
- Cladribine is resistant to degradation by which enzyme?
a) Cyclooxygenase
b) Acetylcholinesterase
c) Adenosine deaminase
d) Xanthine oxidase
Answer: c) Adenosine deaminase
- Which enzyme phosphorylates cladribine inside cells?
a) Deoxycytidine kinase
b) Monoamine oxidase
c) Dihydrofolate reductase
d) Angiotensin-converting enzyme
Answer: a) Deoxycytidine kinase
- Cladribine selectively accumulates in lymphocytes mainly because lymphocytes have:
a) High deoxycytidine kinase and low 5′-nucleotidase activity
b) Low deoxycytidine kinase and high 5′-nucleotidase activity
c) High acetylcholinesterase activity
d) No nucleoside transporters
Answer: a) High deoxycytidine kinase and low 5′-nucleotidase activity
- The final major cellular effect of cladribine in lymphocytes is:
a) Increased platelet aggregation
b) Apoptosis
c) Increased histamine release
d) Bronchodilation
Answer: b) Apoptosis
- Cladribine is useful in multiple sclerosis mainly because it:
a) Blocks dopamine receptors
b) Depletes autoreactive lymphocytes and promotes immune reconstitution
c) Stimulates acetylcholine release
d) Directly dissolves myelin plaques
Answer: b) Depletes autoreactive lymphocytes and promotes immune reconstitution
- Which brand name is associated with oral cladribine for multiple sclerosis?
a) Leustatin
b) Mavenclad
c) Plavix
d) Rituxan
Answer: b) Mavenclad
- Which disease is an important oncologic use of cladribine?
a) Hairy cell leukemia
b) Chronic asthma
c) Peptic ulcer disease
d) Hypertension
Answer: a) Hairy cell leukemia
- The most important immune-related adverse effect of cladribine is:
a) Hyperkalemia
b) Lymphopenia
c) Ototoxicity
d) Gingival hyperplasia
Answer: b) Lymphopenia
- Which infection-related precaution is important before cladribine therapy?
a) Active chronic infections should be evaluated and treated before therapy
b) All patients must receive live vaccines during therapy
c) Infection screening is unnecessary
d) Antibiotics replace all monitoring requirements
Answer: a) Active chronic infections should be evaluated and treated before therapy
- Cladribine is contraindicated during pregnancy mainly because it can cause:
a) Fetal harm
b) Excessive calcium absorption
c) Severe constipation only
d) Reduced gastric acid secretion
Answer: a) Fetal harm
- Which drug is most closely related to cladribine as a purine analogue used in hairy cell leukemia?
a) Pentostatin
b) Metoprolol
c) Amlodipine
d) Omeprazole
Answer: a) Pentostatin
- Compared with fingolimod, cladribine primarily works by:
a) Blocking S1P receptors only
b) Direct intracellular lymphocyte toxicity and apoptosis
c) Inhibiting HMG-CoA reductase
d) Blocking bacterial cell wall synthesis
Answer: b) Direct intracellular lymphocyte toxicity and apoptosis
- Which laboratory parameter requires monitoring during cladribine therapy?
a) Lymphocyte count
b) Serum amylase only
c) Arterial oxygen saturation only
d) Visual acuity only
Answer: a) Lymphocyte count
FAQs
What is the mechanism of action of cladribine?
Cladribine is a purine nucleoside analogue that enters lymphocytes, is phosphorylated by deoxycytidine kinase, and forms active metabolites that damage DNA, impair DNA repair, disrupt mitochondrial function, and induce apoptosis.
Why is cladribine selective for lymphocytes?
Cladribine is selective for lymphocytes because these cells have relatively high deoxycytidine kinase activity and relatively low 5′-nucleotidase activity. This causes active cladribine metabolites to accumulate inside lymphocytes.
Is cladribine used in multiple sclerosis?
Yes. Oral cladribine, under the brand name Mavenclad, is used in adults with relapsing forms of multiple sclerosis, including relapsing-remitting disease and active secondary progressive disease, usually when another therapy has failed or is not tolerated.
Is cladribine used in cancer?
Yes. Injectable cladribine has an important role in active hairy cell leukemia, where it kills malignant B lymphocytes and helps improve bone marrow function and blood counts.
What is the most important adverse effect of cladribine?
The most important adverse effect is lymphopenia, which increases the risk of infections. Bone marrow suppression is also important, especially with injectable cladribine used in hematologic malignancies.
Why is cladribine contraindicated in pregnancy?
Cladribine can cause fetal harm because it interferes with DNA synthesis and cell survival. It is contraindicated during pregnancy, and effective contraception is required according to product-specific guidance.
Can live vaccines be given during cladribine therapy?
Live or live-attenuated vaccines are generally avoided during and after cladribine therapy until immune recovery is adequate. Vaccination status should be reviewed before starting treatment.
How is cladribine different from fingolimod?
Fingolimod traps lymphocytes in lymph nodes by modulating sphingosine-1-phosphate receptors. Cladribine directly depletes lymphocytes through intracellular activation, DNA damage, and apoptosis.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

