
Table of Contents
Introduction
Brilinta is the brand name of ticagrelor, an oral antiplatelet drug used mainly to prevent thrombotic cardiovascular and cerebrovascular events. It belongs to the P2Y12 platelet receptor inhibitor class and is commonly used in patients with acute coronary syndrome, history of myocardial infarction, coronary artery disease at high risk of thrombotic events, and selected patients with acute ischemic stroke or high-risk transient ischemic attack.
Ticagrelor is clinically important because it reduces platelet aggregation without requiring metabolic activation. This makes it different from clopidogrel and prasugrel, which are thienopyridine prodrugs. Ticagrelor is a direct-acting, reversible P2Y12 receptor antagonist. For exam purposes, Brilinta is remembered as a reversible P2Y12 inhibitor that blocks ADP-mediated platelet activation and reduces the risk of myocardial infarction, stroke, cardiovascular death, and stent thrombosis.
Ticagrelor is usually used with low-dose aspirin unless contraindicated. However, maintenance aspirin doses above 100 mg daily should generally be avoided because higher aspirin maintenance doses may reduce the effectiveness of ticagrelor.
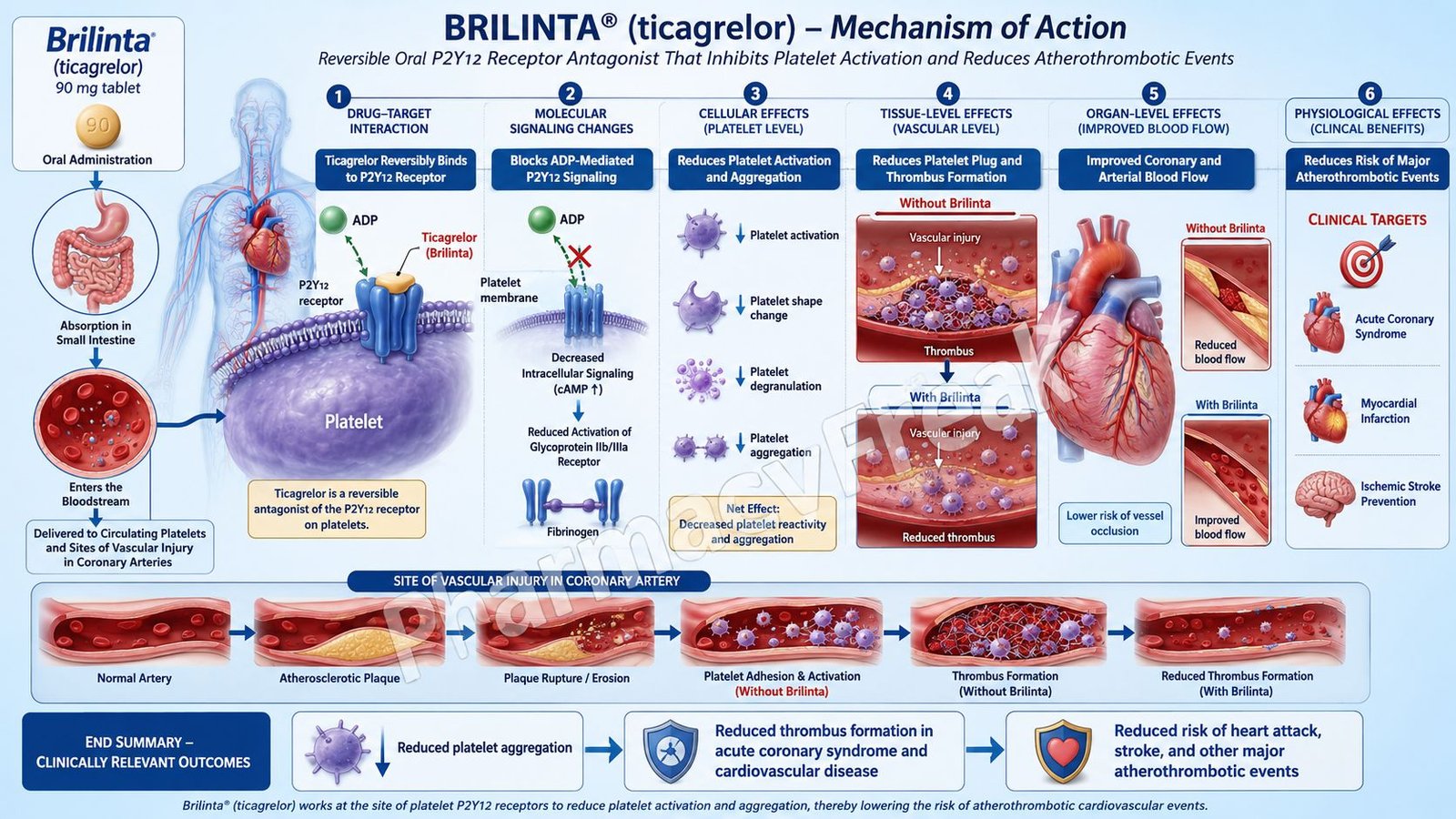
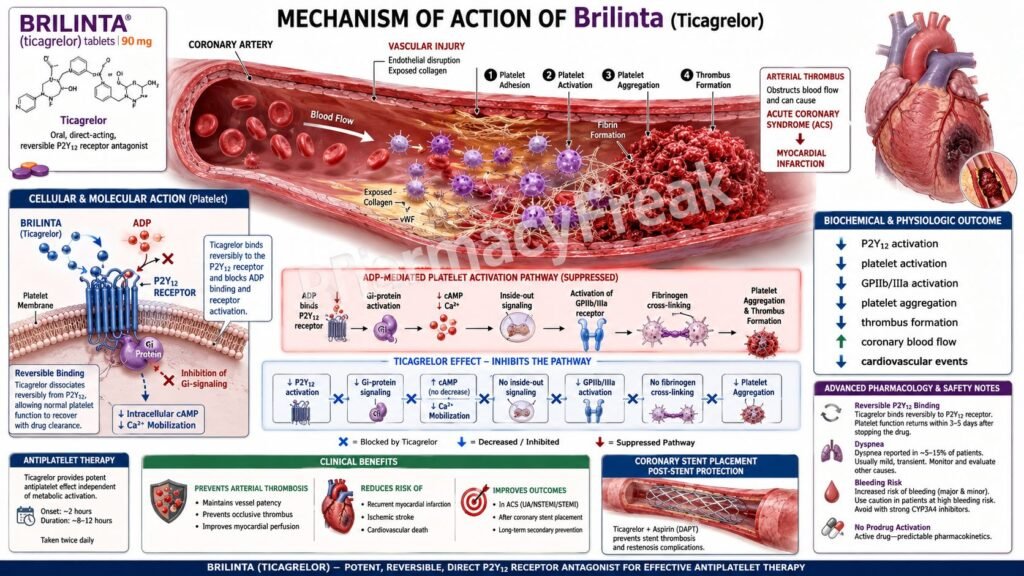
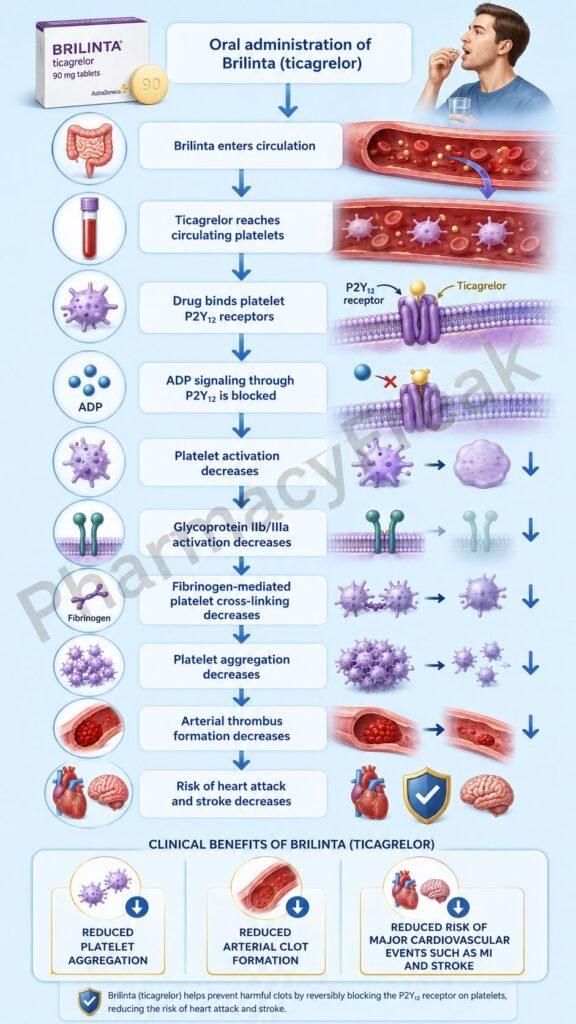
Mechanism of Action (Step-wise)
Step 1: Platelet activation begins after vascular injury
When a blood vessel is injured, platelets adhere to the damaged endothelium and become activated. Activated platelets release adenosine diphosphate, commonly called ADP. ADP is a key mediator that amplifies platelet activation and recruits more platelets to the site of injury.
Step 2: ADP normally stimulates the P2Y12 receptor
The P2Y12 receptor is a G protein-coupled receptor located on the platelet surface. Under normal conditions, ADP binds to this receptor and activates Gi protein signaling. This inhibits adenylyl cyclase, reduces cyclic AMP levels inside platelets, and promotes platelet activation.
Step 3: Reduced cAMP promotes glycoprotein IIb/IIIa activation
When intracellular cAMP falls, platelets become more reactive. This leads to activation of the glycoprotein IIb/IIIa receptor complex. Activated glycoprotein IIb/IIIa binds fibrinogen and creates bridges between adjacent platelets, producing platelet aggregation.
Step 4: Ticagrelor reversibly blocks the P2Y12 receptor
Ticagrelor binds reversibly to the platelet P2Y12 receptor at a site different from the ADP binding site. By blocking P2Y12 signaling, ticagrelor prevents ADP from fully activating platelets. Since its binding is reversible, platelet function gradually recovers after the drug is stopped.
Step 5: cAMP levels remain relatively preserved
Because P2Y12-mediated Gi signaling is inhibited, adenylyl cyclase activity is not suppressed to the same extent. This helps maintain intracellular cAMP, which keeps platelets in a less activated state.
Step 6: Glycoprotein IIb/IIIa activation is reduced
By preventing ADP-driven platelet activation, ticagrelor indirectly reduces glycoprotein IIb/IIIa activation. As a result, fibrinogen-mediated platelet cross-linking decreases.
Step 7: Platelet aggregation and thrombus formation are reduced
The final therapeutic effect is inhibition of platelet aggregation. This reduces formation of arterial platelet-rich thrombi, which are central to acute coronary syndrome, myocardial infarction, ischemic stroke, and stent thrombosis.
Step 8: Additional adenosine-related effects may occur
Ticagrelor may inhibit cellular uptake of adenosine through equilibrative nucleoside transporter-1. Increased extracellular adenosine may contribute to some effects such as dyspnea and ventricular pauses. However, the main antiplatelet action is due to P2Y12 receptor inhibition.
Pharmacokinetics
Ticagrelor is administered orally and is absorbed rapidly. It can be taken with or without food. Unlike clopidogrel and prasugrel, ticagrelor does not require metabolic activation to produce antiplatelet activity. This is an important exam point because it explains its faster and more predictable platelet inhibition.
Ticagrelor undergoes hepatic metabolism mainly through CYP3A4 and CYP3A5. It forms an active metabolite that also contributes to P2Y12 inhibition. Because of CYP3A metabolism, strong CYP3A inhibitors such as ketoconazole, clarithromycin, ritonavir, and some azole antifungals may increase ticagrelor exposure and bleeding risk. Strong CYP3A inducers such as rifampin, carbamazepine, phenytoin, and St. John’s wort may reduce ticagrelor levels and decrease efficacy.
Ticagrelor and its active metabolite are highly protein bound. The drug is eliminated mainly through hepatic and biliary pathways, with minor renal elimination. It is usually given twice daily because of its pharmacokinetic profile and reversible receptor binding.
Renal dose adjustment is generally not the major issue with ticagrelor, but caution is required in patients at high bleeding risk. Severe hepatic impairment should be avoided because impaired hepatic metabolism may increase drug exposure and bleeding risk.
Clinical Uses
Brilinta is used to reduce the risk of cardiovascular death, myocardial infarction, and stroke in patients with acute coronary syndrome. Acute coronary syndrome includes unstable angina, non-ST elevation myocardial infarction, and ST elevation myocardial infarction.
It is also used in patients with a history of myocardial infarction to reduce future thrombotic cardiovascular events. In patients who undergo stent placement for acute coronary syndrome, ticagrelor reduces the risk of stent thrombosis.
Ticagrelor is also used to reduce the risk of first myocardial infarction or stroke in selected patients with coronary artery disease who are at high risk for such events. Clinical evidence for this use is especially associated with patients having coronary artery disease and type 2 diabetes mellitus.
Another important approved use is prevention of stroke in patients with acute ischemic stroke of mild severity or high-risk transient ischemic attack. In this setting, ticagrelor is used for a short duration with aspirin according to clinical protocols.
The major therapeutic goal of ticagrelor is prevention of arterial thrombosis. Therefore, it is mainly useful in platelet-rich clot formation, especially in coronary and cerebral arteries.
Adverse Effects
The most important adverse effect of ticagrelor is bleeding. Like other antiplatelet drugs, it can cause serious and sometimes fatal bleeding. It is contraindicated in patients with active pathological bleeding, such as active peptic ulcer bleeding or intracranial hemorrhage, and in patients with a history of intracranial hemorrhage.
Dyspnea is another characteristic adverse effect. It is usually mild to moderate but may be troublesome in some patients. The mechanism is thought to be related partly to increased extracellular adenosine.
Ticagrelor may cause bradyarrhythmias, including ventricular pauses and atrioventricular block. Caution is needed in patients with sick sinus syndrome, second- or third-degree AV block, or bradycardia-related syncope unless protected by a pacemaker.
Other adverse effects include epistaxis, gastrointestinal bleeding, bruising, headache, dizziness, nausea, and increased uric acid levels. Rarely, hypersensitivity reactions such as angioedema may occur.
Important safety warnings include avoiding unnecessary discontinuation because stopping ticagrelor too early may increase the risk of myocardial infarction, stroke, stent thrombosis, or cardiovascular death. If surgery with major bleeding risk is planned, ticagrelor is commonly interrupted several days before the procedure under medical supervision.
Maintenance aspirin doses above 100 mg daily should generally be avoided with ticagrelor because higher aspirin doses may reduce ticagrelor effectiveness.
Comparative Analysis
Ticagrelor, clopidogrel, and prasugrel all inhibit the platelet P2Y12 receptor, but they differ in reversibility, activation, potency, and clinical use.
Ticagrelor is a direct-acting reversible P2Y12 inhibitor. It does not require metabolic activation and has a relatively rapid onset of platelet inhibition. This makes it more predictable than clopidogrel in many patients.
Clopidogrel is an irreversible P2Y12 inhibitor and a prodrug. It requires hepatic activation mainly through CYP2C19. Genetic polymorphisms or drug interactions affecting CYP2C19 can reduce clopidogrel activation and clinical response. This is a common exam comparison.
Prasugrel is also an irreversible P2Y12 inhibitor and a prodrug, but it produces more potent and consistent platelet inhibition than clopidogrel. However, prasugrel has a higher bleeding risk and is generally avoided in patients with prior stroke or TIA.
Cangrelor is an intravenous reversible P2Y12 inhibitor. It has a very rapid onset and offset and is mainly used in procedural settings such as percutaneous coronary intervention when immediate platelet inhibition is needed.
Compared with aspirin, ticagrelor acts at a different point in platelet activation. Aspirin irreversibly inhibits cyclooxygenase-1, reducing thromboxane A2 formation. Ticagrelor blocks ADP-mediated P2Y12 signaling. Because these pathways are different, aspirin and ticagrelor are often combined for dual antiplatelet therapy in appropriate patients.
MCQs
- Brilinta contains which active drug?
a) Clopidogrel
b) Ticagrelor
c) Prasugrel
d) Cangrelor
Answer: b) Ticagrelor
- Ticagrelor mainly acts by blocking which platelet receptor?
a) P2Y12 receptor
b) Thromboxane receptor
c) Glycoprotein IIb/IIIa receptor directly
d) PAR-1 receptor
Answer: a) P2Y12 receptor
- Which statement best describes ticagrelor?
a) Irreversible COX-1 inhibitor
b) Reversible P2Y12 receptor antagonist
c) Direct thrombin inhibitor
d) Vitamin K antagonist
Answer: b) Reversible P2Y12 receptor antagonist
- ADP activation of the P2Y12 receptor normally causes which intracellular effect in platelets?
a) Increased cAMP
b) Reduced cAMP
c) Increased nitric oxide synthesis
d) Direct fibrinolysis
Answer: b) Reduced cAMP
- Ticagrelor reduces platelet aggregation mainly by preventing activation of which final platelet aggregation receptor complex?
a) Beta-1 receptor
b) H1 receptor
c) Glycoprotein IIb/IIIa complex
d) NMDA receptor
Answer: c) Glycoprotein IIb/IIIa complex
- Which feature differentiates ticagrelor from clopidogrel?
a) Ticagrelor is a prodrug requiring CYP2C19 activation
b) Ticagrelor is a direct-acting reversible P2Y12 inhibitor
c) Ticagrelor is used only intravenously
d) Ticagrelor directly dissolves fibrin clots
Answer: b) Ticagrelor is a direct-acting reversible P2Y12 inhibitor
- The most important serious adverse effect of ticagrelor is:
a) Hyperkalemia
b) Severe bleeding
c) Ototoxicity
d) Hypoglycemia
Answer: b) Severe bleeding
- Which condition is a contraindication to ticagrelor?
a) History of intracranial hemorrhage
b) Controlled hypertension
c) Stable angina without bleeding
d) Mild renal impairment
Answer: a) History of intracranial hemorrhage
- Which adverse effect is characteristically associated with ticagrelor and may be related to adenosine?
a) Dyspnea
b) Gingival hyperplasia
c) Tendon rupture
d) Nephrolithiasis
Answer: a) Dyspnea
- Ticagrelor is metabolized mainly by which enzyme system?
a) CYP3A4 and CYP3A5
b) CYP2D6 only
c) Monoamine oxidase
d) Alcohol dehydrogenase
Answer: a) CYP3A4 and CYP3A5
- Which aspirin maintenance dose issue is important with ticagrelor?
a) Aspirin must always be above 300 mg daily
b) Aspirin doses above 100 mg daily may reduce ticagrelor effectiveness
c) Aspirin completely blocks ticagrelor absorption
d) Aspirin is absolutely contraindicated with ticagrelor in all patients
Answer: b) Aspirin doses above 100 mg daily may reduce ticagrelor effectiveness
- Which drug is an intravenous reversible P2Y12 inhibitor used mainly in procedural settings?
a) Cangrelor
b) Warfarin
c) Alteplase
d) Aspirin
Answer: a) Cangrelor
- In acute coronary syndrome, ticagrelor reduces the risk of:
a) Bacterial endocarditis only
b) Cardiovascular death, myocardial infarction, and stroke
c) Bronchial asthma attacks
d) Migraine aura only
Answer: b) Cardiovascular death, myocardial infarction, and stroke
- Which statement about stopping ticagrelor is correct?
a) It can be stopped abruptly in all stented patients without risk
b) Early discontinuation may increase risk of thrombotic cardiovascular events
c) It should never be stopped before any surgery
d) It has no effect on stent thrombosis
Answer: b) Early discontinuation may increase risk of thrombotic cardiovascular events
- Ticagrelor is generally avoided in severe hepatic impairment because:
a) It is exclusively excreted unchanged by the kidney
b) Severe hepatic impairment may increase ticagrelor exposure and bleeding risk
c) It causes insulin resistance only in liver disease
d) It becomes inactive in the intestine
Answer: b) Severe hepatic impairment may increase ticagrelor exposure and bleeding risk
FAQs
What is the mechanism of action of Brilinta?
Brilinta, or ticagrelor, reversibly blocks the platelet P2Y12 receptor. This prevents ADP-mediated platelet activation, reduces glycoprotein IIb/IIIa activation, and decreases platelet aggregation.
Is ticagrelor reversible or irreversible?
Ticagrelor is a reversible P2Y12 receptor inhibitor. This is different from clopidogrel and prasugrel, which inhibit P2Y12 irreversibly.
Does ticagrelor require metabolic activation?
No. Ticagrelor is direct acting and does not require metabolic activation. However, it is metabolized by CYP3A4 and CYP3A5 and has an active metabolite.
Why is ticagrelor used with aspirin?
Ticagrelor and aspirin inhibit platelet activation through different pathways. Aspirin blocks thromboxane A2 formation, while ticagrelor blocks ADP-mediated P2Y12 signaling. Their combination provides dual antiplatelet therapy in appropriate patients.
What is the most important adverse effect of ticagrelor?
The most important adverse effect is bleeding, including serious and sometimes fatal bleeding. It should not be used in patients with active pathological bleeding or a history of intracranial hemorrhage.
Why does ticagrelor cause dyspnea?
Dyspnea with ticagrelor may be related partly to increased extracellular adenosine due to inhibition of adenosine uptake. It is often mild to moderate but may require switching therapy if intolerable.
How is ticagrelor different from clopidogrel?
Ticagrelor is reversible and direct acting, while clopidogrel is irreversible and requires CYP2C19 activation. Ticagrelor generally produces faster and more predictable platelet inhibition.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

