
Table of Contents
Introduction
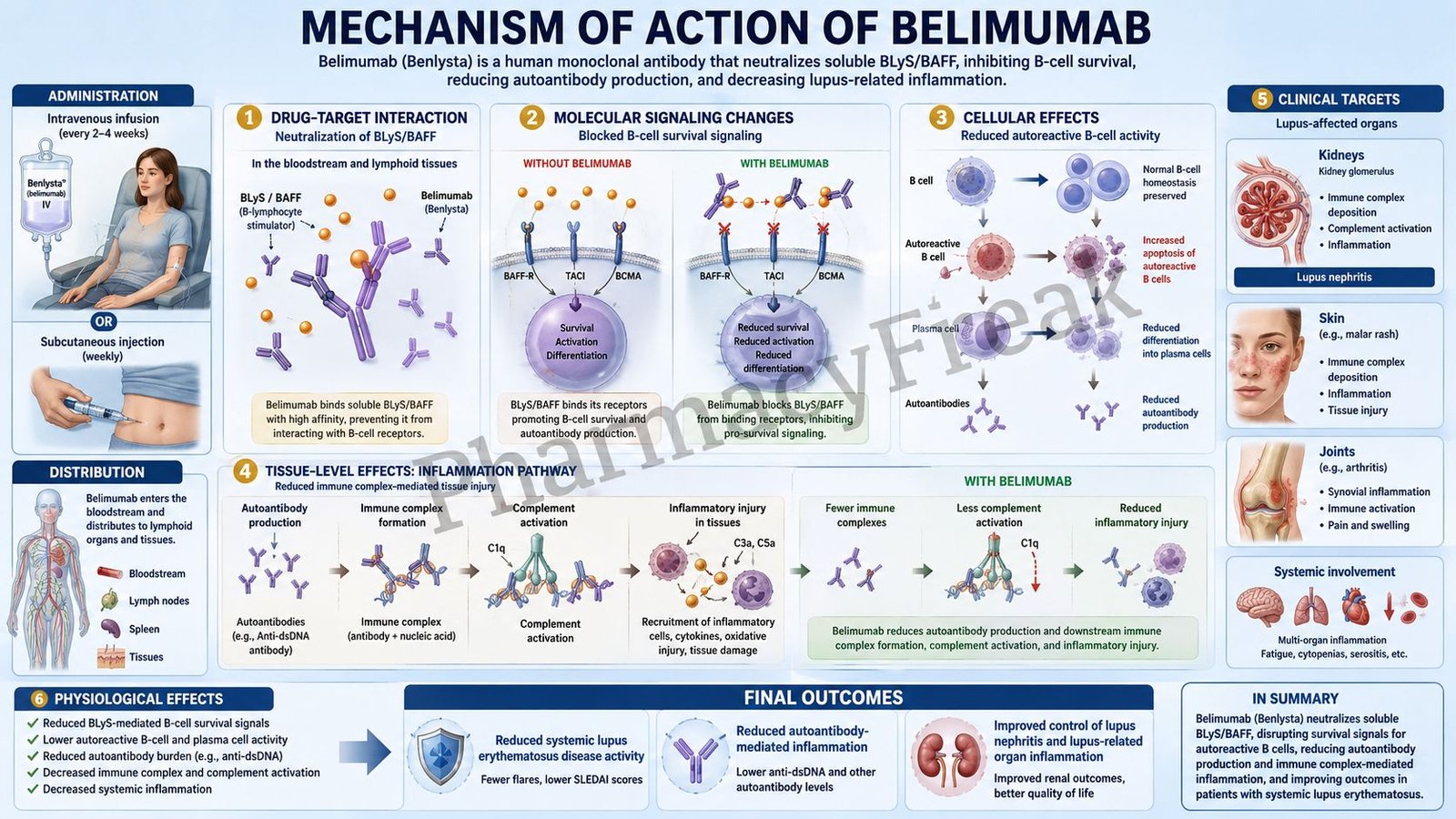
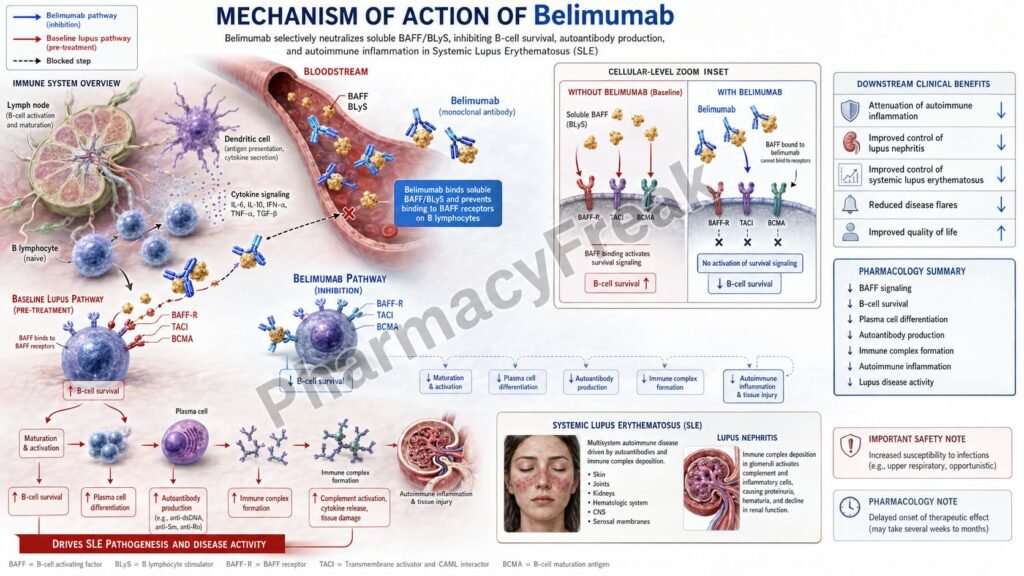
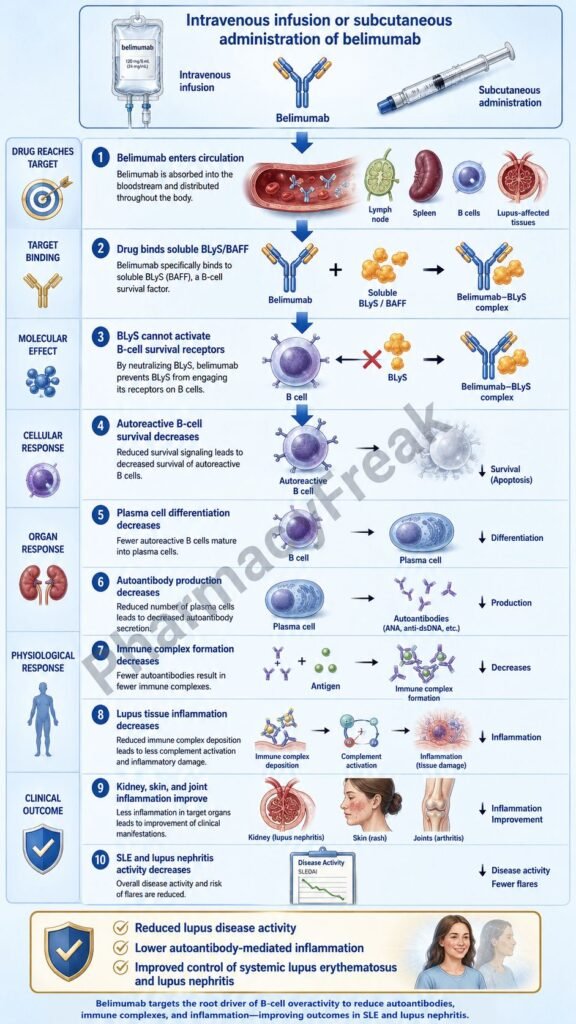
Belimumab is a human IgG1λ monoclonal antibody used in the treatment of autoimmune lupus disorders. It is marketed under the brand name Benlysta and is classified as a B-lymphocyte stimulator-specific inhibitor, also called a BLyS inhibitor or BAFF inhibitor.
Belimumab is used in patients 5 years of age and older with active systemic lupus erythematosus who are receiving standard therapy. It is also used in patients 5 years of age and older with active lupus nephritis who are receiving standard therapy. Current prescribing information states that belimumab is not recommended in patients with severe active central nervous system lupus because its efficacy has not been evaluated in that situation.
Systemic lupus erythematosus is an autoimmune disease characterized by abnormal B-cell activation, autoantibody production, immune complex formation, complement activation, and inflammation affecting multiple organs. Lupus nephritis is a serious renal manifestation of lupus in which immune-mediated inflammation damages the kidneys.
For pharmacy, medical, nursing, and competitive exam students, belimumab is important because it is a targeted biologic therapy. Unlike corticosteroids or broad immunosuppressants, belimumab specifically interferes with B-cell survival signaling by neutralizing soluble BLyS, also known as BAFF. This reduces survival of autoreactive B cells and decreases differentiation into antibody-producing plasma cells.
Mechanism of Action (Step-wise)
- Primary target: Soluble BLyS/BAFF
Belimumab specifically binds soluble B-lymphocyte stimulator, known as BLyS. BLyS is also called B-cell activating factor, BAFF, or TNFSF13B. BLyS is an important survival factor for B cells.
In lupus, increased BLyS activity supports survival of autoreactive B cells. These abnormal B cells can produce autoantibodies against nuclear and cellular antigens, contributing to immune complex formation and tissue inflammation.
- Prevention of BLyS binding to B-cell receptors
Normally, soluble BLyS binds to receptors on B cells, including BAFF-R, TACI, and BCMA. These receptors support B-cell maturation, survival, differentiation, and antibody production.
Belimumab binds soluble BLyS and prevents it from interacting with its receptors on B cells. Importantly, belimumab does not directly bind B cells. Instead, it neutralizes soluble BLyS before BLyS can activate B-cell survival pathways.
- Reduced survival of autoreactive B cells
Autoreactive B cells are B cells that react against the body’s own tissues. In systemic lupus erythematosus, these cells contribute to autoantibody formation and chronic immune activation.
By blocking BLyS signaling, belimumab reduces survival of B cells, including autoreactive B cells. This helps decrease the pool of immune cells that can continue driving lupus activity.
- Reduced differentiation into plasma cells
B cells can differentiate into plasma cells, which produce antibodies. In lupus, plasma cells produce autoantibodies such as anti-double-stranded DNA antibodies.
Belimumab reduces B-cell differentiation into immunoglobulin-producing plasma cells. This lowers autoantibody production and decreases immune complex-mediated inflammation.
- Reduction in circulating B-cell subsets
Treatment with belimumab reduces circulating CD19-positive, CD20-positive, naïve, activated, and SLE-associated B-cell subsets. These pharmacodynamic effects are consistent with its role as a B-cell survival inhibitor.
- Reduction in autoantibodies and improvement in complement levels
Belimumab can reduce immunoglobulin G and anti-double-stranded DNA antibody levels. In patients with low complement levels at baseline, treatment may increase complement C3 and C4 levels over time. These changes reflect reduced autoimmune activity, although clinical response must always be assessed by symptoms, organ involvement, and disease activity scores.
- Effect in systemic lupus erythematosus
In systemic lupus erythematosus, belimumab reduces B-cell-driven immune activation. This helps reduce disease activity, flares, autoantibody production, and inflammatory manifestations in suitable patients receiving standard therapy.
- Effect in lupus nephritis
In lupus nephritis, autoantibodies and immune complexes contribute to kidney inflammation and proteinuria. By decreasing autoreactive B-cell survival and autoantibody production, belimumab helps reduce immune-mediated renal inflammation when used with standard lupus nephritis therapy.
- Final therapeutic effect
The final therapeutic effect of belimumab is reduced BLyS-mediated B-cell survival, decreased autoreactive B-cell activity, reduced autoantibody production, improved immunologic markers, and better control of active systemic lupus erythematosus and active lupus nephritis in selected patients.
Pharmacokinetics
Belimumab is administered either by intravenous infusion or subcutaneous injection. The intravenous formulation is given as a weight-based infusion, while the subcutaneous formulation is given as a fixed or weight-based dose depending on age, body weight, and indication.
Absorption:
After subcutaneous administration, belimumab is absorbed slowly. In adults with active systemic lupus erythematosus receiving 200 mg subcutaneously once weekly, the time to maximum serum concentration at steady state is about 2.6 days. The subcutaneous bioavailability is approximately 74%.
Distribution:
Belimumab is a monoclonal antibody and mainly distributes within vascular and interstitial spaces. The volume of distribution at steady state is approximately 5 L after intravenous or subcutaneous administration, which is consistent with limited distribution outside extracellular fluid compartments.
Metabolism:
Belimumab is not metabolized by cytochrome P450 enzymes. Like other IgG monoclonal antibodies, it is expected to be degraded by proteolytic catabolism into small peptides and amino acids.
Excretion:
Belimumab is not primarily eliminated unchanged through the kidneys like many small-molecule drugs. It is cleared mainly through normal protein catabolic pathways.
Half-life and duration:
Belimumab has a long terminal half-life. The terminal half-life is approximately 19.4 days after intravenous administration and approximately 18.3 days after subcutaneous administration in adults with active SLE. This long half-life supports intermittent intravenous dosing or weekly subcutaneous dosing.
Special pharmacokinetic point:
In lupus nephritis, heavy proteinuria can initially increase belimumab clearance and lower exposure, but available data do not support dose adjustment solely because of high proteinuria.
Clinical Uses
- Active systemic lupus erythematosus:
Belimumab is used in patients 5 years of age and older with active SLE who are receiving standard therapy. It helps reduce B-cell-mediated autoimmune activity and disease flares. - Active lupus nephritis:
Belimumab is used in patients 5 years of age and older with active lupus nephritis who are receiving standard therapy. It is used as an add-on treatment to reduce immune-mediated renal inflammation. - Autoantibody-positive lupus disease activity:
Belimumab is especially relevant in patients with active serologic disease, such as positive autoantibodies, because its mechanism directly targets B-cell survival and autoantibody production pathways. - Steroid-sparing strategy:
In selected patients, improved disease control with belimumab may help reduce long-term reliance on corticosteroids, although steroid tapering must be done carefully under medical supervision. - Add-on biologic therapy:
Belimumab is generally used with standard lupus therapies such as hydroxychloroquine, corticosteroids, mycophenolate mofetil, azathioprine, or other immunosuppressants depending on disease manifestation. - Not recommended in severe active CNS lupus:
Belimumab is not recommended in severe active central nervous system lupus because efficacy has not been evaluated in this group.
Adverse Effects
Common adverse effects of belimumab include:
- Nausea
- Diarrhea
- Fever
- Nasopharyngitis
- Bronchitis
- Pharyngitis
- Insomnia
- Headache
- Migraine
- Pain in extremity
- Depression
- Injection site reactions with subcutaneous use
- Infusion-related reactions with intravenous use
Important serious or clinically significant adverse effects include:
- Serious infections
- Opportunistic infections
- Progressive multifocal leukoencephalopathy
- Hypersensitivity reactions
- Anaphylaxis
- Depression and suicidal ideation
- Malignancy risk
- Infusion reactions
- Immunization concerns with live vaccines
Belimumab can increase infection risk because it suppresses B-cell survival and immune activity. Serious and sometimes fatal infections have been reported in patients receiving immunosuppressive agents, including belimumab. Therapy may need to be interrupted if a patient develops a new serious infection.
Hypersensitivity reactions, including anaphylaxis, are important safety concerns. Intravenous belimumab should be administered by healthcare professionals prepared to manage serious hypersensitivity reactions.
Depression and suicidal thoughts have been reported with belimumab. Patients should be assessed for depression and monitored for new or worsening mood changes during treatment. Live vaccines should not be given concurrently with belimumab.
Comparative Analysis
| Feature | Belimumab | Rituximab | Anifrolumab | Mycophenolate Mofetil |
|---|---|---|---|---|
| Drug class | BLyS/BAFF inhibitor monoclonal antibody | Anti-CD20 monoclonal antibody | Type I interferon receptor antagonist | Antimetabolite immunosuppressant |
| Main target | Soluble BLyS/BAFF | CD20 on B cells | Type I interferon receptor subunit 1 | Inosine monophosphate dehydrogenase |
| Main action | Reduces B-cell survival and plasma cell differentiation | Depletes CD20-positive B cells | Blocks type I interferon signaling | Reduces lymphocyte proliferation |
| Main lupus use | Active SLE and active lupus nephritis | Off-label or selected refractory autoimmune use | Moderate to severe SLE in selected adults | Lupus nephritis and systemic autoimmune control |
| Effect on B cells | Indirect reduction by blocking survival factor | Direct B-cell depletion | Indirect immune pathway modulation | Reduces lymphocyte proliferation |
| Route | Intravenous or subcutaneous | Intravenous | Intravenous | Oral |
| Major concerns | Infection, hypersensitivity, depression/suicidality | Infusion reaction, infection, hepatitis B reactivation | Infection, herpes zoster | GI toxicity, myelosuppression, teratogenicity |
Belimumab differs from rituximab because it does not directly deplete B cells by binding CD20. Instead, it neutralizes soluble BLyS and reduces B-cell survival. Anifrolumab targets the type I interferon pathway, which is another important pathway in lupus inflammation. Mycophenolate mofetil is a small-molecule immunosuppressant that reduces lymphocyte proliferation and is commonly used in lupus nephritis.
MCQs
- Belimumab is best classified as:
a) TNF-alpha inhibitor
b) BLyS-specific inhibitor
c) Calcineurin inhibitor
d) JAK inhibitor
Answer: b) BLyS-specific inhibitor
- Belimumab is marketed under which brand name?
a) Benlysta
b) Humira
c) Rituxan
d) Xeljanz
Answer: a) Benlysta
- The main molecular target of belimumab is:
a) CD20 receptor
b) Soluble BLyS/BAFF
c) TNF-alpha
d) IL-17A
Answer: b) Soluble BLyS/BAFF
- BLyS is important because it promotes:
a) B-cell survival
b) Platelet aggregation
c) Gastric acid secretion
d) Insulin release
Answer: a) B-cell survival
- Belimumab reduces lupus activity mainly by:
a) Increasing autoantibody production
b) Stimulating T-cell proliferation
c) Reducing survival of autoreactive B cells
d) Activating complement excessively
Answer: c) Reducing survival of autoreactive B cells
- Belimumab does not directly bind:
a) Soluble BLyS
b) B cells
c) BAFF
d) B-cell survival factor
Answer: b) B cells
- Which antibody level may decrease during belimumab therapy?
a) Anti-double-stranded DNA antibody
b) Anti-insulin antibody only
c) Anti-rabies antibody only
d) Anti-thyroglobulin only
Answer: a) Anti-double-stranded DNA antibody
- Belimumab is used in:
a) Active systemic lupus erythematosus
b) Acute bacterial meningitis
c) Type 1 diabetes ketoacidosis
d) Malaria
Answer: a) Active systemic lupus erythematosus
- Belimumab is also approved for:
a) Active lupus nephritis
b) Acute myocardial infarction
c) Asthma attack
d) Hyperthyroid crisis
Answer: a) Active lupus nephritis
- Which route can be used for belimumab administration?
a) Intravenous or subcutaneous
b) Inhalational only
c) Intrathecal only
d) Sublingual only
Answer: a) Intravenous or subcutaneous
- Which serious adverse effect is associated with belimumab?
a) Serious infection
b) Severe hypoglycemia
c) Ototoxicity
d) Gingival hyperplasia
Answer: a) Serious infection
- Live vaccines during belimumab therapy are generally:
a) Avoided
b) Required weekly
c) Used to increase drug absorption
d) Given with every infusion
Answer: a) Avoided
- Belimumab differs from rituximab because rituximab targets:
a) CD20 on B cells
b) Soluble BLyS
c) IL-5 receptor alpha
d) SGLT2
Answer: a) CD20 on B cells
- The final therapeutic effect of belimumab includes:
a) Reduced autoantibody production and reduced B-cell survival
b) Increased bacterial cell wall synthesis
c) Direct bronchodilation
d) Increased platelet aggregation
Answer: a) Reduced autoantibody production and reduced B-cell survival
- Which statement about belimumab is correct?
a) It neutralizes soluble BLyS and reduces autoreactive B-cell survival
b) It directly blocks beta receptors
c) It is an insulin analog
d) It is a rescue medicine for acute bronchospasm
Answer: a) It neutralizes soluble BLyS and reduces autoreactive B-cell survival
FAQs
- What is belimumab used for?
Belimumab is used for active systemic lupus erythematosus and active lupus nephritis in patients 5 years of age and older who are receiving standard therapy.
- What is the mechanism of action of belimumab?
Belimumab binds soluble BLyS, also called BAFF, and prevents it from binding to receptors on B cells. This reduces survival of autoreactive B cells and decreases differentiation into antibody-producing plasma cells.
- Is belimumab a steroid?
No. Belimumab is not a steroid. It is a targeted monoclonal antibody that inhibits BLyS-mediated B-cell survival.
- Does belimumab directly kill B cells?
No. Belimumab does not directly bind or kill B cells like an anti-CD20 antibody. It blocks soluble BLyS, a survival factor needed by many B cells.
- Why is belimumab useful in lupus?
Lupus involves abnormal B-cell activation and autoantibody production. Belimumab reduces survival of autoreactive B cells, which can reduce autoantibody production and immune-mediated inflammation.
- Can belimumab be used in lupus nephritis?
Yes. Belimumab is used as add-on therapy in active lupus nephritis along with standard therapy.
- What are common side effects of belimumab?
Common side effects include nausea, diarrhea, fever, nasopharyngitis, bronchitis, insomnia, headache, migraine, depression, and injection site reactions.
- What serious adverse effects can occur with belimumab?
Serious adverse effects include serious infections, hypersensitivity reactions, anaphylaxis, progressive multifocal leukoencephalopathy, depression, suicidal ideation, and possible malignancy risk.
- Can live vaccines be given with belimumab?
Live vaccines should generally be avoided during belimumab therapy because belimumab affects immune function.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

