

Table of Contents
Introduction
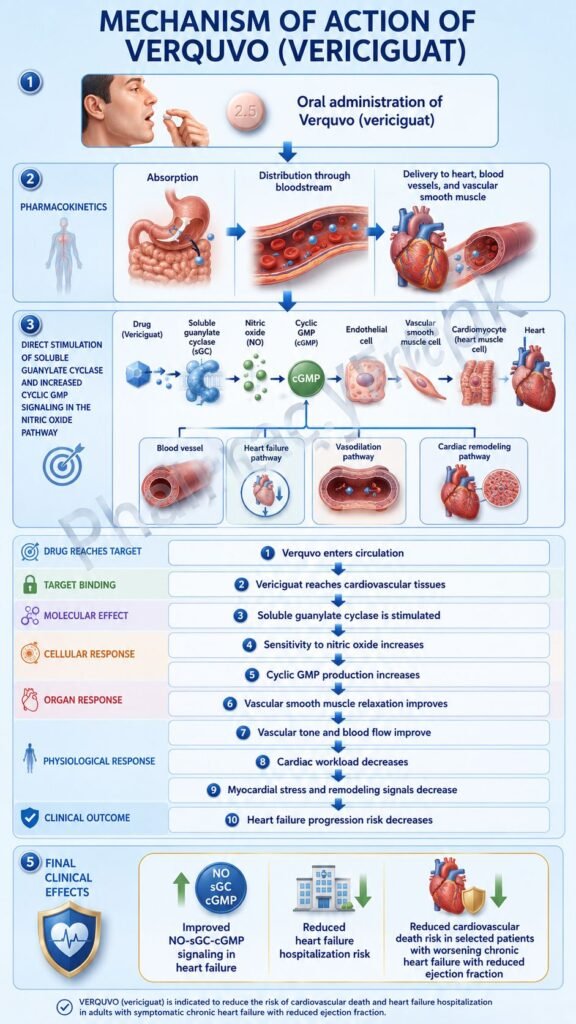
Verquvo is the brand name of vericiguat, an oral soluble guanylate cyclase stimulator used in selected adults with symptomatic chronic heart failure. It is mainly used in patients with heart failure and ejection fraction less than 45% who have recently had worsening heart failure requiring hospitalization or outpatient intravenous diuretic therapy. Its clinical role is to reduce the risk of cardiovascular death and heart failure hospitalization.
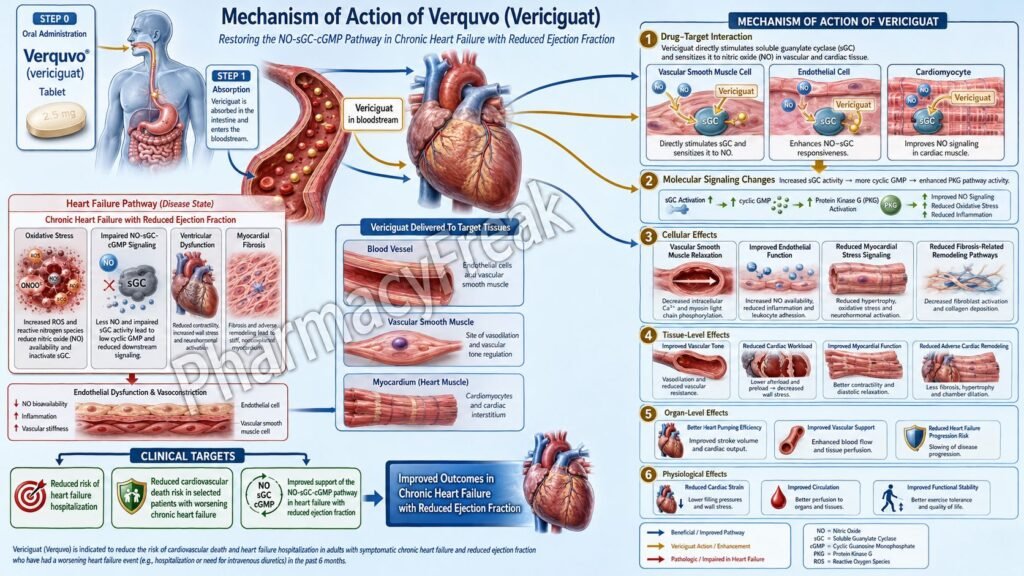
Verquvo is important in pharmacology because it targets the nitric oxide–soluble guanylate cyclase–cyclic guanosine monophosphate pathway, commonly written as the NO–sGC–cGMP pathway. This pathway is involved in vascular tone, cardiac function, myocardial remodeling, and smooth muscle relaxation.
In heart failure, oxidative stress and endothelial dysfunction reduce nitric oxide availability. This weakens sGC activation and lowers cGMP production. Reduced cGMP signaling contributes to vasoconstriction, vascular stiffness, myocardial dysfunction, and adverse cardiac remodeling. Verquvo helps restore this pathway by directly stimulating soluble guanylate cyclase.
For pharmacy, medical, nursing, and competitive exam students, Verquvo is an important heart failure drug because it is different from beta-blockers, ACE inhibitors, ARBs, ARNIs, mineralocorticoid receptor antagonists, and SGLT2 inhibitors. It does not primarily block neurohormonal activation or increase diuresis. Instead, it improves defective NO–sGC–cGMP signaling.
Mechanism of Action (Step-wise)
- Primary target: Soluble guanylate cyclase
Verquvo contains vericiguat, which stimulates soluble guanylate cyclase. Soluble guanylate cyclase is an intracellular enzyme and a major receptor for nitric oxide in vascular smooth muscle and other cardiovascular tissues.
- Normal NO–sGC–cGMP pathway
Under normal conditions, nitric oxide binds to soluble guanylate cyclase. This activates sGC and increases conversion of guanosine triphosphate into cyclic guanosine monophosphate.
cGMP is an important second messenger that regulates vascular tone, smooth muscle relaxation, cardiac contractility, and cardiac remodeling.
- Impaired pathway in heart failure
In heart failure, nitric oxide synthesis is reduced and soluble guanylate cyclase activity becomes impaired. This leads to reduced cGMP generation. Low cGMP signaling contributes to vascular dysfunction, myocardial stiffness, inflammation, fibrosis, and worsening cardiac performance.
- Direct stimulation of sGC
Vericiguat directly stimulates soluble guanylate cyclase. It can increase sGC activity independently of nitric oxide and also works synergistically with available endogenous nitric oxide.
- Increase in intracellular cGMP
By stimulating sGC, Verquvo increases intracellular cGMP levels. Increased cGMP activates protein kinase G and other downstream pathways involved in vascular and myocardial regulation.
- Smooth muscle relaxation and vasodilation
Increased cGMP promotes vascular smooth muscle relaxation. This causes vasodilation, which may reduce vascular resistance and improve hemodynamic stress on the failing heart.
- Effect on cardiac remodeling
cGMP signaling may help oppose pathological myocardial remodeling, fibrosis, hypertrophy, and vascular dysfunction. This is important because adverse remodeling is a major contributor to chronic heart failure progression.
- Final therapeutic effect
The final therapeutic effect of Verquvo is improved NO–sGC–cGMP signaling, vasodilation, reduced cardiovascular stress, and lower risk of heart failure hospitalization and cardiovascular death in appropriate high-risk patients with symptomatic chronic heart failure.
Pharmacokinetics
Verquvo is administered orally as vericiguat tablets. It is taken once daily with food. The recommended starting dose is 2.5 mg once daily with food, and the dose is doubled approximately every 2 weeks to reach a target maintenance dose of 10 mg once daily as tolerated.
Absorption:
Vericiguat is absorbed after oral administration. Its absolute bioavailability is approximately 93% when taken with food. Food increases exposure and reduces pharmacokinetic variability, which is why Verquvo should be taken with food. Tablets may be swallowed whole or crushed and mixed with water for patients who have difficulty swallowing.
Distribution:
Vericiguat is highly protein-bound, mainly to serum albumin. Its steady-state volume of distribution is approximately 44 L in healthy subjects.
Metabolism:
Vericiguat is metabolized mainly by glucuronidation through UGT1A9 and, to a lesser extent, UGT1A1. It forms an inactive N-glucuronide metabolite. CYP-mediated metabolism is a minor pathway.
Excretion:
After oral administration, vericiguat-related material is eliminated through both urine and feces. About 53% of the dose is excreted in urine, mainly as inactive metabolite, and about 45% is excreted in feces, mainly as unchanged drug.
Half-life and duration:
The half-life of vericiguat is approximately 30 hours in patients with heart failure. Steady state is reached after about 6 days, supporting once-daily dosing.
Special pharmacokinetic point:
Verquvo should be taken with food because food improves exposure. Drugs that alter gastric pH have less clinical effect when Verquvo is taken properly with food.
Clinical Uses
- Symptomatic chronic heart failure:
Verquvo is used in adults with symptomatic chronic heart failure and ejection fraction less than 45%. - Recent worsening heart failure:
It is especially used after recent heart failure hospitalization or need for outpatient intravenous diuretics. - Reduction of cardiovascular death risk:
Verquvo helps reduce the risk of cardiovascular death in selected high-risk heart failure patients. - Reduction of heart failure hospitalization:
It reduces the risk of hospitalization due to worsening heart failure. - Add-on heart failure therapy:
Verquvo is generally used along with standard heart failure therapy, not as a replacement for core treatments such as beta-blockers, ACE inhibitors, ARBs, ARNIs, mineralocorticoid receptor antagonists, or SGLT2 inhibitors. - High-risk HFrEF or mildly reduced EF group:
Since its labeled population includes ejection fraction less than 45%, Verquvo is relevant in patients with reduced or mildly reduced systolic function after a worsening heart failure event.
Adverse Effects
Common and clinically important adverse effects of Verquvo include:
- Hypotension
- Symptomatic low blood pressure
- Dizziness
- Light-headedness
- Anemia
- Nausea
- Headache
- Dyspepsia
- Risk of syncope in susceptible patients
The most common adverse reactions reported in at least 5% of patients are hypotension and anemia.
Important precautions include:
- Embryo-fetal toxicity:
Verquvo may cause fetal harm and is contraindicated during pregnancy. Females of reproductive potential require pregnancy testing before treatment and effective contraception during therapy and for 1 month after stopping treatment. - Concomitant sGC stimulators:
Verquvo is contraindicated with other soluble guanylate cyclase stimulators because of excessive cGMP-mediated vasodilation and hypotension risk. - PDE-5 inhibitors:
Concomitant use with phosphodiesterase-5 inhibitors is not recommended because both can increase cGMP signaling and may increase the risk of hypotension. - Low blood pressure risk:
Patients with baseline hypotension, volume depletion, or excessive vasodilator exposure require careful assessment before and during treatment.
Verquvo is not used for emergency treatment of acute pulmonary edema or unstable decompensated heart failure. It is used after stabilization in selected chronic heart failure patients.
Comparative Analysis
| Feature | Verquvo | Sacubitril/Valsartan | Dapagliflozin | Carvedilol |
|---|---|---|---|---|
| Generic name | Vericiguat | Sacubitril + valsartan | Dapagliflozin | Carvedilol |
| Drug class | Soluble guanylate cyclase stimulator | ARNI | SGLT2 inhibitor | Beta-blocker |
| Main target | NO–sGC–cGMP pathway | Neprilysin and angiotensin II receptor | Sodium-glucose cotransporter 2 | Beta and alpha receptors |
| Main action | Increases cGMP signaling and vasodilation | Increases natriuretic peptides and blocks RAAS | Promotes glucosuria, natriuresis, and HF benefit | Reduces sympathetic overactivity |
| Main HF role | Reduces CV death/HF hospitalization after worsening HF | Core HFrEF therapy | Core HF therapy in many patients | Core HFrEF therapy |
| Route | Oral | Oral | Oral | Oral |
| Major adverse effect | Hypotension, anemia | Hypotension, hyperkalemia, renal effects, angioedema | Genital infections, volume depletion | Bradycardia, fatigue, hypotension |
| Pregnancy | Contraindicated | Contraindicated | Usually avoided | Use depends on clinical situation |
Verquvo differs from standard neurohormonal drugs because it works through the NO–sGC–cGMP pathway. Sacubitril/valsartan modifies natriuretic peptide and renin-angiotensin signaling. Dapagliflozin acts through renal SGLT2 inhibition and has metabolic and hemodynamic benefits. Carvedilol reduces sympathetic stimulation of the heart. Verquvo is especially useful as an add-on option in patients with recent worsening heart failure despite background therapy.
MCQs
- Verquvo contains which active drug?
a) Sacubitril
b) Vericiguat
c) Ivabradine
d) Digoxin
Answer: b) Vericiguat
- Verquvo belongs to which drug class?
a) Beta-blocker
b) ACE inhibitor
c) Soluble guanylate cyclase stimulator
d) Calcium channel blocker
Answer: c) Soluble guanylate cyclase stimulator
- The main intracellular second messenger increased by Verquvo is:
a) cAMP
b) IP3
c) cGMP
d) DAG
Answer: c) cGMP
- Verquvo acts mainly on which signaling pathway?
a) NO–sGC–cGMP pathway
b) JAK–STAT pathway
c) COX-prostaglandin pathway
d) GABA chloride channel pathway
Answer: a) NO–sGC–cGMP pathway
- Verquvo is mainly used in selected adults with:
a) Symptomatic chronic heart failure
b) Acute bacterial pneumonia
c) Type 1 diabetes mellitus
d) Bronchial asthma attack
Answer: a) Symptomatic chronic heart failure
- The final vascular effect of increased cGMP signaling is:
a) Vasoconstriction
b) Smooth muscle relaxation and vasodilation
c) Increased platelet aggregation only
d) Increased bronchial secretion
Answer: b) Smooth muscle relaxation and vasodilation
- Verquvo is contraindicated with:
a) Other soluble guanylate cyclase stimulators
b) Iron tablets
c) Vitamin D
d) Antacids only
Answer: a) Other soluble guanylate cyclase stimulators
- Which adverse effect is commonly associated with Verquvo?
a) Hypotension
b) Severe neutropenia
c) Ototoxicity
d) Gingival hyperplasia
Answer: a) Hypotension
- Verquvo should be taken:
a) Once daily with food
b) Only at bedtime without water
c) Once weekly by injection
d) By inhalation during acute dyspnea
Answer: a) Once daily with food
- Which enzyme primarily metabolizes vericiguat through glucuronidation?
a) UGT1A9
b) CYP2D6
c) MAO-B
d) Acetylcholinesterase
Answer: a) UGT1A9
- Verquvo is contraindicated during pregnancy because of:
a) Embryo-fetal toxicity risk
b) Severe ototoxicity in adults only
c) Insulin resistance only
d) Thyroid C-cell tumor warning only
Answer: a) Embryo-fetal toxicity risk
- Verquvo is different from PDE-5 inhibitors because Verquvo:
a) Stimulates soluble guanylate cyclase
b) Blocks bacterial ribosomes
c) Inhibits sodium-glucose cotransporter 2
d) Blocks beta receptors
Answer: a) Stimulates soluble guanylate cyclase
- The half-life of vericiguat in heart failure patients is approximately:
a) 2 hours
b) 8 hours
c) 30 hours
d) 7 days
Answer: c) 30 hours
- Verquvo is used after which clinical situation in heart failure?
a) Recent heart failure hospitalization or need for outpatient IV diuretics
b) Simple seasonal allergy
c) Acute migraine without cardiac disease
d) Mild fever only
Answer: a) Recent heart failure hospitalization or need for outpatient IV diuretics
- Which statement about Verquvo is correct?
a) It increases cGMP by stimulating soluble guanylate cyclase
b) It directly replaces insulin
c) It is an antibiotic
d) It is used as a rescue inhaler
Answer: a) It increases cGMP by stimulating soluble guanylate cyclase
FAQs
- What is Verquvo used for?
Verquvo is used in selected adults with symptomatic chronic heart failure and ejection fraction less than 45% who have recently had heart failure hospitalization or required outpatient intravenous diuretics. It reduces the risk of cardiovascular death and heart failure hospitalization.
- What is the mechanism of action of Verquvo?
Verquvo stimulates soluble guanylate cyclase, an enzyme in the nitric oxide signaling pathway. This increases cGMP levels, causing smooth muscle relaxation, vasodilation, and improved cardiovascular signaling.
- Is Verquvo a beta-blocker?
No. Verquvo is not a beta-blocker. It is a soluble guanylate cyclase stimulator that acts through the NO–sGC–cGMP pathway.
- Does Verquvo increase nitric oxide?
Verquvo does not primarily increase nitric oxide production. It directly stimulates soluble guanylate cyclase and also enhances its response to available endogenous nitric oxide.
- Why is cGMP important in heart failure?
cGMP helps regulate vascular tone, myocardial function, and cardiac remodeling. Reduced cGMP signaling contributes to vascular and myocardial dysfunction in heart failure.
- What are the common side effects of Verquvo?
The most common side effects are hypotension and anemia. Some patients may also experience dizziness, light-headedness, nausea, or headache.
- Why should Verquvo be taken with food?
Food improves vericiguat exposure and reduces pharmacokinetic variability. Therefore, Verquvo should be taken once daily with food.
- Can Verquvo be used during pregnancy?
No. Verquvo is contraindicated during pregnancy because it may cause fetal harm.
- Can Verquvo be used with PDE-5 inhibitors?
Concomitant use with PDE-5 inhibitors is not recommended because both can increase cGMP-related vasodilatory effects and increase the risk of hypotension.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

