
Table of Contents
Introduction
Promacta is the brand name of eltrombopag, an orally active thrombopoietin receptor agonist used to increase platelet production in selected patients with thrombocytopenia. It is especially important in conditions where platelet counts are low enough to increase bleeding risk.
Promacta is used in persistent or chronic immune thrombocytopenia, thrombocytopenia associated with chronic hepatitis C when platelet counts limit interferon-based therapy, and severe aplastic anemia. Current prescribing information states that Promacta is indicated for thrombocytopenia in adult and pediatric patients 1 year and older with persistent or chronic immune thrombocytopenia after insufficient response to corticosteroids, immunoglobulins, or splenectomy; for thrombocytopenia in chronic hepatitis C to allow initiation and maintenance of interferon-based therapy; and for severe aplastic anemia in selected adult and pediatric patients.
For pharmacy, medical, nursing, and competitive exam students, Promacta is important because it represents a non-peptide oral thrombopoietin receptor agonist. Unlike platelet transfusion, it does not directly supply platelets. Instead, it stimulates bone marrow megakaryocyte proliferation and differentiation, leading to increased platelet production.
Promacta should not be used simply to normalize platelet count. Its goal is to raise platelet count enough to reduce bleeding risk while avoiding excessive platelet elevation, which may increase thrombotic risk.
Mechanism of Action (Step-wise)
- Primary target: Thrombopoietin receptor
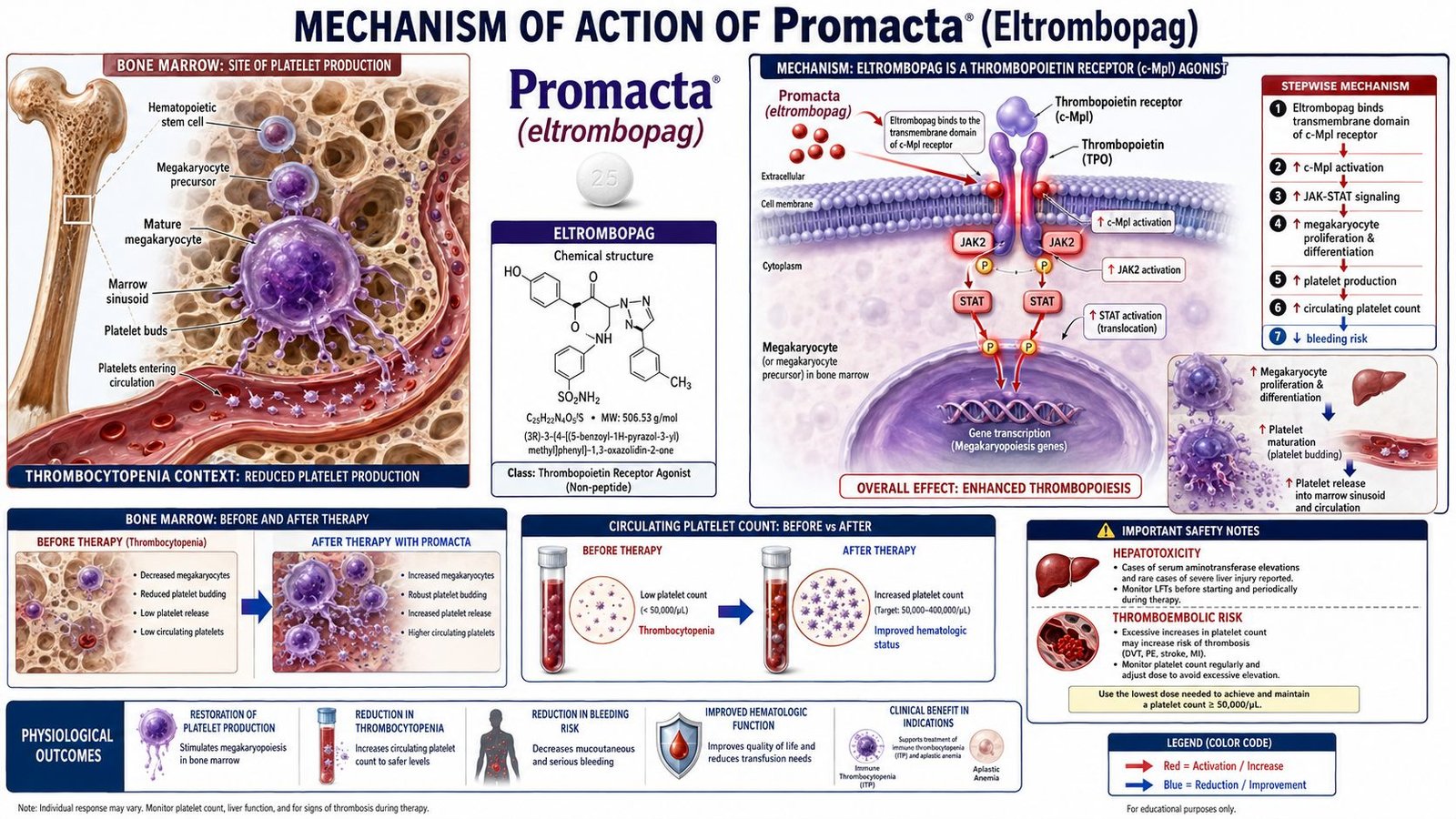
Promacta contains eltrombopag, a small-molecule thrombopoietin receptor agonist. It interacts with the human thrombopoietin receptor, also known as c-Mpl, which is expressed mainly on hematopoietic stem cells and megakaryocyte lineage cells.
- Binding to the transmembrane domain of TPO receptor
Eltrombopag binds to the transmembrane domain of the thrombopoietin receptor. This is pharmacologically important because it binds at a site different from endogenous thrombopoietin. The FDA label describes eltrombopag as a TPO-receptor agonist that interacts with the transmembrane domain of the human TPO receptor and initiates signaling cascades that induce megakaryocyte proliferation and differentiation.
- Activation of intracellular signaling pathways
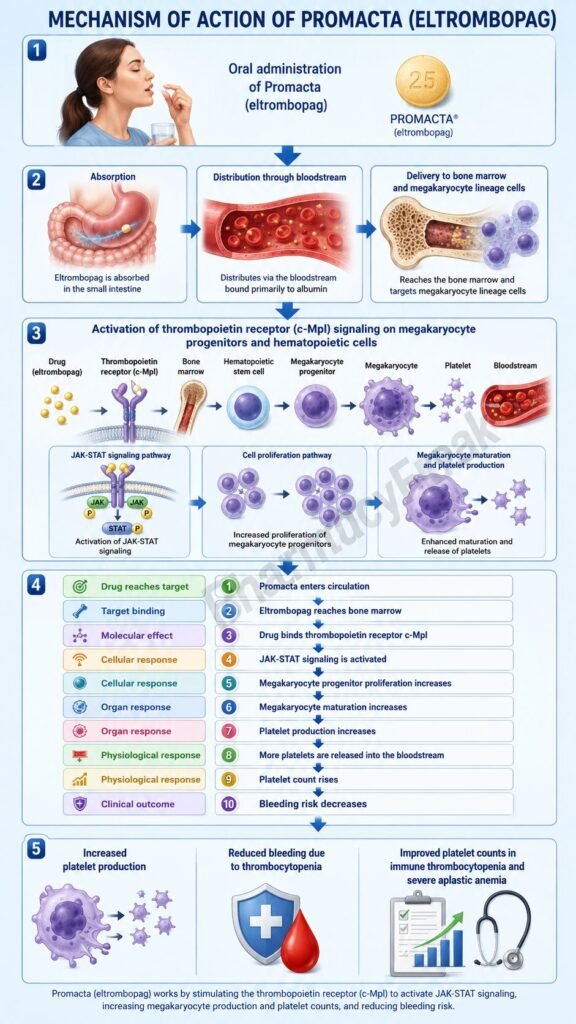
After receptor activation, intracellular signaling pathways are stimulated. These include pathways involved in hematopoietic cell growth, survival, maturation, and platelet formation. Important downstream pathways include JAK/STAT, MAPK, and PI3K-related signaling.
- Megakaryocyte proliferation
The megakaryocyte lineage is responsible for platelet formation. By activating thrombopoietin receptor signaling, Promacta increases the proliferation of megakaryocyte progenitor cells in the bone marrow.
- Megakaryocyte differentiation and maturation
Eltrombopag not only increases the number of megakaryocyte precursors but also supports their differentiation into mature megakaryocytes. Mature megakaryocytes extend cytoplasmic processes called proplatelets, which eventually fragment into circulating platelets.
- Increased platelet production
As megakaryocyte activity increases, platelet production rises. This helps improve thrombocytopenia and reduces bleeding tendency in responsive patients.
- Effect in immune thrombocytopenia
In immune thrombocytopenia, platelets are destroyed by immune-mediated mechanisms and platelet production may also be inadequate. Promacta helps compensate by increasing platelet generation from the bone marrow.
- Effect in severe aplastic anemia
In severe aplastic anemia, bone marrow failure leads to reduced production of blood cells. By stimulating thrombopoietin receptor signaling on hematopoietic progenitor cells, eltrombopag may improve platelet production and, in some patients, support broader hematopoietic recovery.
- Final therapeutic effect
The final therapeutic effect of Promacta is increased platelet count, reduced bleeding risk, and improved ability to continue necessary treatment in selected patients with thrombocytopenia.
Pharmacokinetics
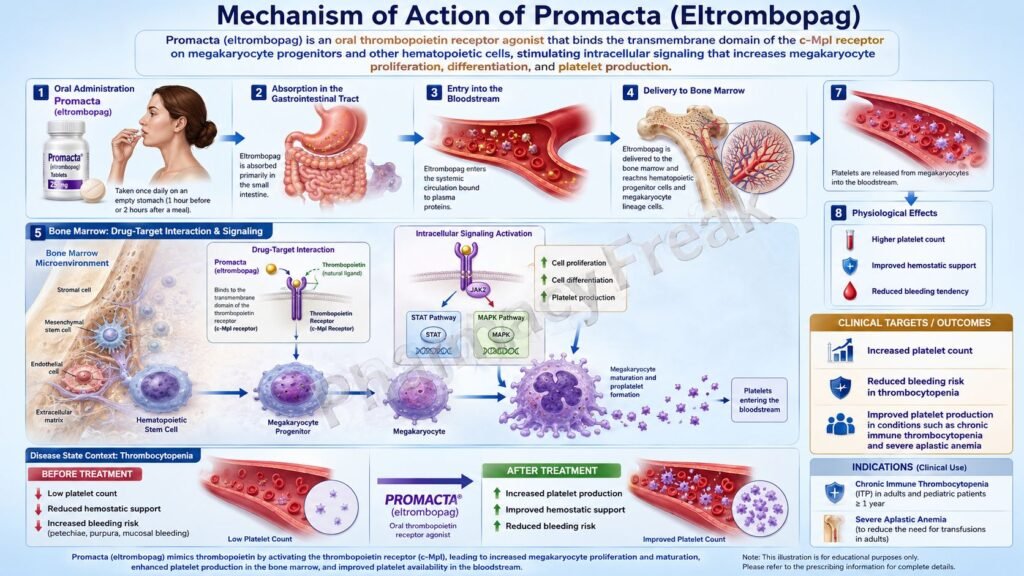
Promacta is administered orally as tablets or oral suspension. It is usually given once daily, and dosing is adjusted according to platelet count response and clinical condition.
Absorption:
Eltrombopag is absorbed after oral administration, with peak concentration occurring approximately 2 to 6 hours after dosing. The label reports that oral absorption of drug-related material after a single 75 mg solution dose was estimated to be at least 52%.
Effect of food and minerals:
A key pharmacokinetic point is chelation with polyvalent cations. Calcium, iron, magnesium, aluminum, selenium, zinc, antacids, dairy products, and mineral supplements can reduce eltrombopag absorption. Therefore, Promacta should be separated from such products according to prescribing instructions.
Distribution:
Eltrombopag is highly bound to plasma proteins, with in vitro studies showing more than 99% binding to human plasma proteins. It is also a substrate of BCRP but not a substrate for P-glycoprotein or OATP1B1.
Metabolism:
Eltrombopag is extensively metabolized through multiple pathways, including cleavage, oxidation, and conjugation with glucuronic acid, glutathione, or cysteine. CYP1A2 and CYP2C8 contribute to oxidative metabolism, while UGT1A1 and UGT1A3 are involved in glucuronidation.
Excretion:
The predominant route of excretion is fecal. About 59% of the dose is eliminated in feces and about 31% in urine. Unchanged eltrombopag is detected in feces but not in urine.
Half-life and duration:
The plasma elimination half-life is approximately 21 to 32 hours in healthy subjects and approximately 26 to 35 hours in patients with immune thrombocytopenia. This supports once-daily dosing.
Special pharmacokinetic point:
Exposure may be higher in some populations, including East or Southeast Asian ancestry patients. Dose adjustment may be needed based on ancestry, hepatic function, platelet response, and clinical indication.
Clinical Uses
- Persistent or chronic immune thrombocytopenia:
Promacta is used in adults and pediatric patients 1 year and older with persistent or chronic immune thrombocytopenia who have had an insufficient response to corticosteroids, immunoglobulins, or splenectomy. It is used when thrombocytopenia and clinical condition increase bleeding risk. - Chronic hepatitis C-associated thrombocytopenia:
Promacta is used to treat thrombocytopenia in patients with chronic hepatitis C when low platelet counts prevent the initiation or maintenance of interferon-based therapy. It is not established for use with direct-acting antiviral regimens without interferon. - Severe aplastic anemia as first-line combination therapy:
Promacta is used with standard immunosuppressive therapy for first-line treatment of severe aplastic anemia in adult and pediatric patients 2 years and older. - Refractory severe aplastic anemia:
It is also used in patients with severe aplastic anemia who have had an insufficient response to immunosuppressive therapy. - Reduction of bleeding risk:
The main therapeutic goal is to raise platelet count enough to reduce bleeding risk, not to normalize platelet count.
Adverse Effects
Common adverse effects of Promacta may include:
- Nausea
- Diarrhea
- Headache
- Fatigue
- Cough
- Upper respiratory tract infection
- Increased liver enzymes
- Arthralgia
- Myalgia
- Oropharyngeal pain
- Abdominal discomfort
- Rash
Important serious adverse effects include:
- Hepatotoxicity
- Hepatic decompensation in chronic hepatitis C patients receiving interferon-based therapy
- Thrombotic or thromboembolic events
- Cataracts
- Bone marrow reticulin formation
- Increased risk of progression of myelodysplastic syndrome to acute myeloid leukemia
- Severe skin reactions, rarely
- Laboratory test interference due to discoloration effects
Promacta carries a warning for hepatic decompensation in patients with chronic hepatitis C and risk of hepatotoxicity. The label states that Promacta in combination with interferon and ribavirin may increase hepatic decompensation risk in chronic hepatitis C, and that Promacta may increase the risk of severe and potentially life-threatening hepatotoxicity.
Thrombotic risk is an important exam point. Because Promacta increases platelet counts, excessive platelet elevation can increase the risk of thrombosis. Therefore, the dose should be adjusted to maintain platelet counts at a safe level rather than a normal level.
Promacta is not indicated for treatment of myelodysplastic syndromes because of concern about increased risk of death and progression to acute myeloid leukemia in that setting.
Comparative Analysis
| Feature | Promacta | Romiplostim | Avatrombopag | Platelet Transfusion |
|---|---|---|---|---|
| Generic name | Eltrombopag | Romiplostim | Avatrombopag | Platelet concentrate |
| Drug class | TPO receptor agonist | TPO receptor agonist | TPO receptor agonist | Blood component therapy |
| Main target | TPO receptor/c-Mpl | TPO receptor/c-Mpl | TPO receptor/c-Mpl | Direct platelet replacement |
| Main action | Stimulates megakaryocyte proliferation and platelet production | Stimulates megakaryocyte proliferation and platelet production | Stimulates megakaryocyte proliferation and platelet production | Immediately increases circulating platelets |
| Route | Oral | Subcutaneous injection | Oral | Intravenous transfusion |
| Common use | ITP, HCV-related thrombocytopenia, severe aplastic anemia | ITP | Thrombocytopenia in chronic liver disease and ITP in some settings | Emergency bleeding or procedural support |
| Major concern | Hepatotoxicity, chelation interactions, thrombosis | Thrombosis, marrow reticulin | Thrombosis | Transfusion reaction, infection risk, short duration |
| Onset of platelet rise | Gradual | Gradual | Gradual | Rapid |
Promacta and romiplostim both stimulate the thrombopoietin receptor, but Promacta is an oral small molecule, while romiplostim is given by subcutaneous injection. Avatrombopag is another oral TPO receptor agonist, but its approved uses and food interaction profile differ from eltrombopag. Platelet transfusion acts immediately by providing platelets directly, while Promacta works gradually by stimulating bone marrow platelet production.
MCQs
- Promacta contains which active drug?
a) Romiplostim
b) Eltrombopag
c) Avatrombopag
d) Filgrastim
Answer: b) Eltrombopag
- Promacta belongs to which drug class?
a) Anticoagulant
b) Thrombopoietin receptor agonist
c) Antiplatelet drug
d) Fibrinolytic drug
Answer: b) Thrombopoietin receptor agonist
- The main receptor targeted by Promacta is:
a) Erythropoietin receptor
b) Thrombopoietin receptor
c) Insulin receptor
d) Histamine H1 receptor
Answer: b) Thrombopoietin receptor
- The thrombopoietin receptor is also known as:
a) c-Mpl
b) EGFR
c) HER2
d) CD20
Answer: a) c-Mpl
- Promacta increases platelet count mainly by stimulating:
a) Platelet destruction
b) Megakaryocyte proliferation and differentiation
c) Fibrin degradation
d) Red cell hemolysis
Answer: b) Megakaryocyte proliferation and differentiation
- Which condition is treated with Promacta?
a) Persistent or chronic immune thrombocytopenia
b) Acute myocardial infarction
c) Hypertensive emergency
d) Acute asthma attack
Answer: a) Persistent or chronic immune thrombocytopenia
- Which food-related issue is important with Promacta?
a) Chelation with polyvalent cations reduces absorption
b) Grapefruit completely blocks absorption
c) High sugar foods increase toxicity only
d) Protein meals prevent all metabolism
Answer: a) Chelation with polyvalent cations reduces absorption
- Which adverse effect is a major warning with Promacta?
a) Hepatotoxicity
b) Ototoxicity
c) Severe hypoglycemia
d) Gingival hyperplasia
Answer: a) Hepatotoxicity
- Promacta should be used to:
a) Normalize platelet count in all patients
b) Raise platelet count enough to reduce bleeding risk
c) Reduce platelet count in thrombocytosis
d) Dissolve existing clots
Answer: b) Raise platelet count enough to reduce bleeding risk
- Which mineral can reduce Promacta absorption by chelation?
a) Calcium
b) Chloride
c) Iodide only
d) Fluoride only
Answer: a) Calcium
- Which serious complication can occur if platelet count rises excessively during Promacta therapy?
a) Thrombosis
b) Severe hypokalemia only
c) Acute bronchospasm
d) Hyperthyroidism
Answer: a) Thrombosis
- Promacta is not indicated for:
a) Myelodysplastic syndromes
b) Chronic ITP with bleeding risk
c) Severe aplastic anemia
d) HCV-related thrombocytopenia with interferon therapy limitation
Answer: a) Myelodysplastic syndromes
- Eltrombopag is administered mainly by which route?
a) Oral
b) Intravenous
c) Intrathecal
d) Inhalational
Answer: a) Oral
- Which cell lineage is directly stimulated by Promacta?
a) Megakaryocytic lineage
b) Neuronal lineage
c) Epithelial lineage only
d) Adipocyte lineage
Answer: a) Megakaryocytic lineage
- Which statement about Promacta is correct?
a) It is an oral TPO receptor agonist that increases platelet production
b) It is a platelet aggregation inhibitor
c) It directly dissolves thrombi
d) It blocks vitamin K recycling
Answer: a) It is an oral TPO receptor agonist that increases platelet production
FAQs
- What is Promacta used for?
Promacta is used to treat low platelet counts in selected patients with persistent or chronic immune thrombocytopenia, chronic hepatitis C-associated thrombocytopenia when interferon-based therapy is limited by low platelets, and severe aplastic anemia.
- What is the mechanism of action of Promacta?
Promacta contains eltrombopag, a thrombopoietin receptor agonist. It stimulates c-Mpl receptors on megakaryocyte progenitor cells, promoting megakaryocyte proliferation, differentiation, and platelet production.
- Is Promacta a platelet transfusion?
No. Promacta is not a platelet transfusion. It does not directly provide platelets. It stimulates the bone marrow to produce more platelets over time.
- Why should Promacta not be taken with dairy or minerals?
Promacta can chelate with polyvalent cations such as calcium, iron, magnesium, aluminum, zinc, and selenium. This reduces absorption and may decrease effectiveness.
- Does Promacta increase bleeding or reduce bleeding?
Promacta is used to reduce bleeding risk by increasing platelet count in patients with clinically significant thrombocytopenia.
- Why is liver monitoring important with Promacta?
Promacta may cause hepatotoxicity and can increase the risk of hepatic decompensation in chronic hepatitis C patients receiving interferon-based therapy. Liver function should be monitored before and during therapy.
- Can Promacta cause blood clots?
Yes. Promacta can increase thrombotic or thromboembolic risk, especially if platelet counts rise too high or if the patient has other risk factors for thrombosis.
- Is Promacta used to normalize platelet count?
No. The goal is not to normalize platelet count. The goal is to increase platelet count enough to reduce bleeding risk.
- Is Promacta used in myelodysplastic syndrome?
No. Promacta is not indicated for patients with myelodysplastic syndromes because of concern about increased risk of death and progression to acute myeloid leukemia.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology
K.D. Tripathi Essentials of Medical Pharmacology
Harrison’s Principles of Internal Medicine
