
Table of Contents
Introduction
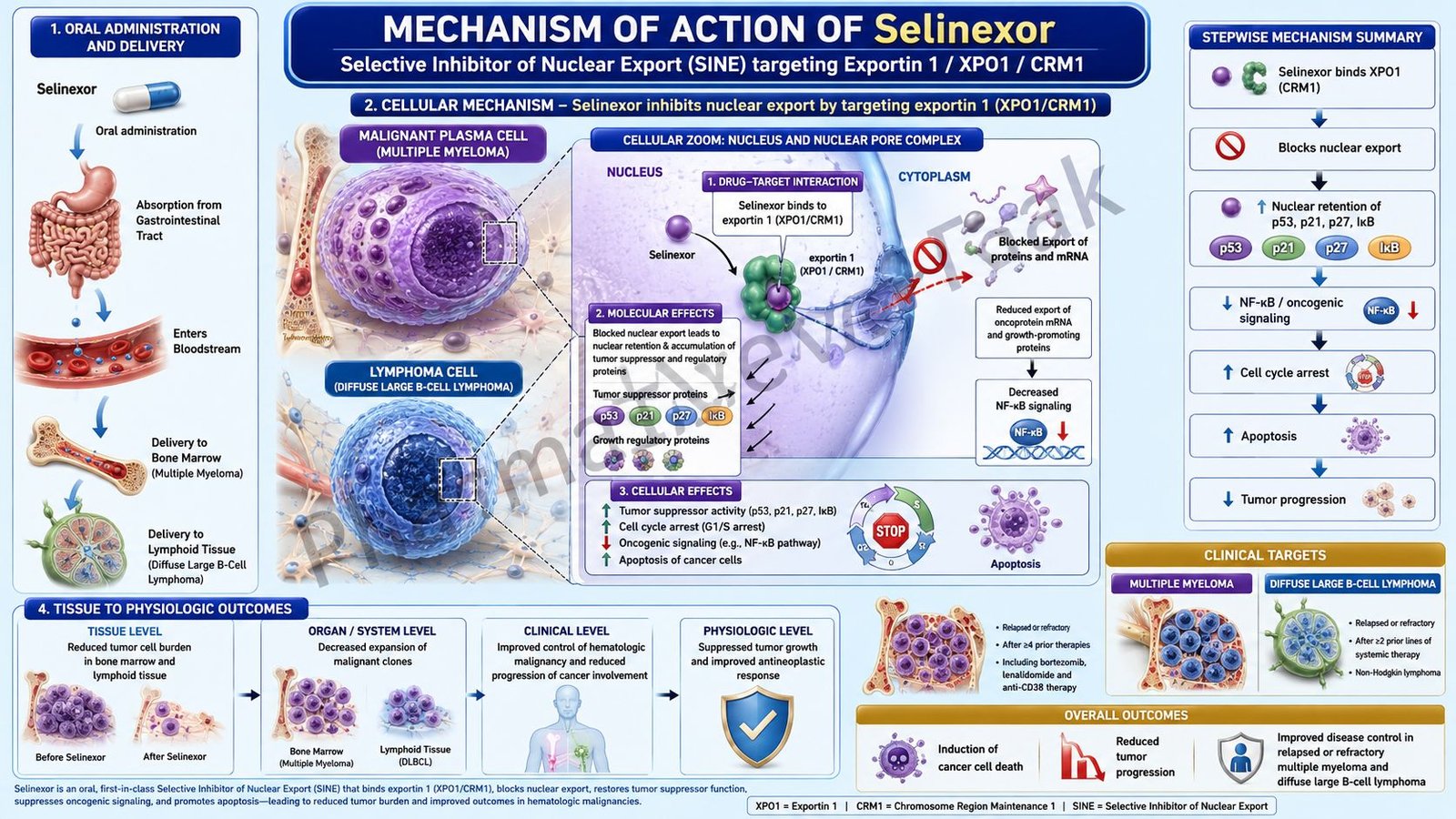
Selinexor is an oral targeted anticancer drug belonging to the class of selective inhibitors of nuclear export, commonly called SINE compounds. It is marketed under the brand name Xpovio and is mainly used in selected patients with relapsed or refractory multiple myeloma. Current prescribing information lists selinexor as a nuclear export inhibitor indicated in combination with bortezomib and dexamethasone for adults with multiple myeloma who have received at least one prior therapy, and in combination with dexamethasone for heavily pretreated relapsed or refractory multiple myeloma.
Selinexor is pharmacologically important because it targets exportin 1, also known as XPO1 or CRM1. XPO1 is a nuclear export protein responsible for transporting several tumor suppressor proteins, growth-regulating proteins, and mRNAs from the nucleus to the cytoplasm. In many cancers, including multiple myeloma, abnormal nuclear export can reduce the nuclear activity of tumor suppressor proteins and support malignant cell survival.
For pharmacy, medical, nursing, and competitive exam students, selinexor is important because it represents a unique mechanism in oncology pharmacology. It does not work like alkylating agents, antimetabolites, proteasome inhibitors, or monoclonal antibodies. Instead, it restores nuclear retention of tumor suppressor proteins, reduces oncogenic protein expression, causes cell-cycle arrest, and promotes apoptosis of cancer cells.
A clinically important update is that selinexor’s former accelerated approval indication for relapsed or refractory diffuse large B-cell lymphoma was withdrawn in 2026, and this withdrawal did not affect its multiple myeloma indications.
Mechanism of Action (Step-wise)
- Primary target: Exportin 1
Selinexor selectively inhibits exportin 1, also called XPO1 or CRM1. XPO1 is a nuclear export protein that transports specific proteins and RNA molecules from the nucleus to the cytoplasm.
- Role of XPO1 in cancer cells
In normal cells, nuclear export helps regulate protein localization and gene expression. In cancer cells, XPO1 is often overexpressed or functionally increased. This can remove tumor suppressor proteins from the nucleus, reducing their ability to control abnormal cell growth.
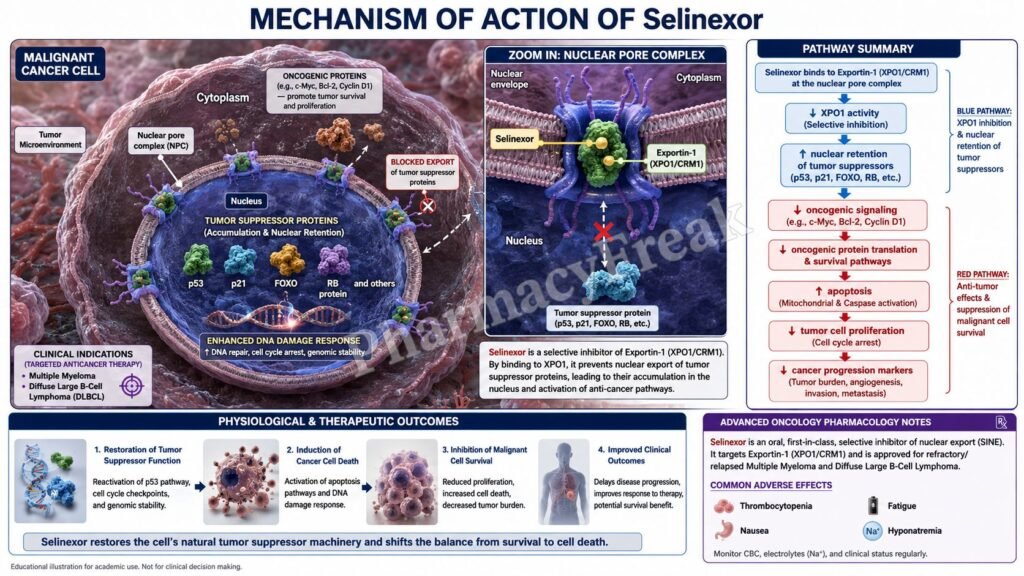
Important tumor suppressor proteins affected by XPO1-mediated export include p53, p21, p27, FOXO proteins, and other growth-regulatory proteins.
- Blocking nuclear export
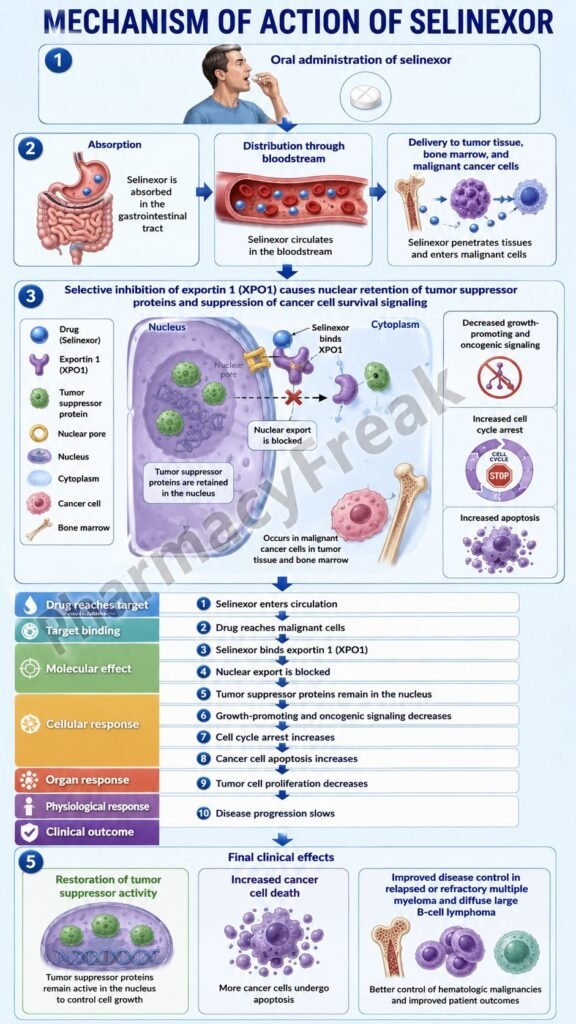
Selinexor binds to XPO1 and reversibly blocks its nuclear export function. This prevents export of tumor suppressor proteins, growth regulators, and certain mRNAs of oncogenic proteins from the nucleus to the cytoplasm. The official label describes selinexor as reversibly inhibiting nuclear export by blocking XPO1, leading to nuclear accumulation of tumor suppressor proteins and reduction of oncoproteins such as c-myc and cyclin D1.
- Nuclear accumulation of tumor suppressor proteins
When XPO1 is inhibited, tumor suppressor proteins remain in the nucleus. Inside the nucleus, these proteins can resume their normal anticancer functions, including DNA damage response, cell-cycle control, transcriptional regulation, and induction of apoptosis.
- Reduction of oncogenic proteins
Selinexor also reduces the expression of several cancer-promoting proteins, including c-Myc and cyclin D1. These proteins normally support malignant cell proliferation, survival, and cell-cycle progression.
- Cell-cycle arrest
By increasing nuclear tumor suppressor activity and reducing oncogenic drivers, selinexor interferes with cell-cycle progression. Cancer cells become less able to divide and proliferate.
- Induction of apoptosis
The combined effect of tumor suppressor activation, reduced oncoprotein expression, and cell-cycle arrest leads to programmed cell death, or apoptosis, especially in malignant cells that depend heavily on abnormal nuclear export.
- Effect in multiple myeloma
In multiple myeloma, malignant plasma cells rely on several survival pathways. Selinexor disrupts nuclear export-dependent survival signaling and may enhance the activity of drugs such as bortezomib and dexamethasone.
- Final therapeutic effect
The final therapeutic effect of selinexor is inhibition of cancer cell survival, reduced malignant plasma cell proliferation, cell-cycle arrest, and apoptosis. This helps control disease progression in selected patients with relapsed or refractory multiple myeloma.
Pharmacokinetics
Selinexor is administered orally as a tablet. It is usually given once weekly or twice weekly depending on the regimen and combination therapy.
Absorption:
Selinexor is absorbed after oral administration. Food does not have a major clinically significant effect on its overall exposure, so it may be taken with or without food depending on the prescribed regimen and patient tolerance.
Distribution:
Selinexor is distributed systemically and reaches malignant cells where it inhibits XPO1. It is highly protein-bound in plasma.
Metabolism:
Selinexor undergoes hepatic metabolism through multiple pathways, including CYP3A4-mediated oxidation, glucuronidation, and glutathione conjugation. Because CYP3A4 participates in metabolism, clinically relevant drug interactions should be considered.
Excretion:
Selinexor and its metabolites are eliminated through both fecal and urinary routes. It is not mainly excreted unchanged as an active drug through a single renal pathway.
Half-life and duration:
Selinexor has a relatively short plasma half-life compared with monoclonal antibodies, but its pharmacodynamic effect on nuclear export and cancer cell signaling supports intermittent dosing schedules.
Special pharmacokinetic point:
Because adverse effects such as nausea, anorexia, thrombocytopenia, and hyponatremia can limit tolerability, dose modification and supportive care are important parts of selinexor therapy.
Clinical Uses
- Multiple myeloma after at least one prior therapy:
Selinexor is used in combination with bortezomib and dexamethasone in adults with multiple myeloma who have received at least one prior therapy. - Heavily pretreated relapsed or refractory multiple myeloma:
Selinexor is used in combination with dexamethasone for adults with relapsed or refractory multiple myeloma who have received at least four prior therapies and whose disease is refractory to at least two proteasome inhibitors, at least two immunomodulatory agents, and an anti-CD38 monoclonal antibody. - Targeted therapy in resistant disease:
Selinexor is useful because its mechanism is different from proteasome inhibitors, immunomodulatory drugs, and anti-CD38 monoclonal antibodies. - Combination therapy:
It is commonly combined with dexamethasone and may be combined with bortezomib depending on the treatment setting. - Not a current FDA-approved DLBCL indication:
Selinexor previously had an accelerated approval indication for relapsed or refractory diffuse large B-cell lymphoma, but this indication was withdrawn in 2026.
Adverse Effects
Common adverse effects of selinexor include:
- Nausea
- Vomiting
- Diarrhea
- Decreased appetite
- Weight loss
- Fatigue
- Thrombocytopenia
- Anemia
- Neutropenia
- Hyponatremia
- Dizziness
- Confusion
- Taste changes
- Constipation
- Upper respiratory tract infection
Important serious adverse effects include:
- Severe thrombocytopenia
- Severe neutropenia
- Serious infections
- Severe gastrointestinal toxicity
- Hyponatremia
- Neurological toxicity
- Dehydration
- Weight loss and anorexia
- Cataracts
- Embryo-fetal toxicity
Thrombocytopenia is one of the most important exam points. Selinexor can reduce platelet counts and increase bleeding risk. Complete blood count monitoring is essential during therapy.
Hyponatremia is another clinically important adverse effect. Sodium levels should be monitored, especially in patients with poor oral intake, vomiting, diarrhea, dehydration, or advanced disease.
Gastrointestinal toxicity is very common. Antiemetic prophylaxis, appetite support, hydration, dose interruption, or dose reduction may be required.
Neurological adverse effects such as dizziness, confusion, altered mental status, or syncope can occur, especially in older or frail patients.
Comparative Analysis
| Feature | Selinexor | Bortezomib | Lenalidomide | Daratumumab |
|---|---|---|---|---|
| Drug class | Selective inhibitor of nuclear export | Proteasome inhibitor | Immunomodulatory drug | Anti-CD38 monoclonal antibody |
| Main target | XPO1/exportin 1 | 26S proteasome | Cereblon-mediated immune and anti-myeloma effects | CD38 on plasma cells |
| Main action | Blocks nuclear export of tumor suppressor proteins | Inhibits proteasomal protein degradation | Enhances immune killing and inhibits myeloma cell survival | Promotes immune-mediated plasma cell killing |
| Main use | Relapsed/refractory multiple myeloma | Multiple myeloma, mantle cell lymphoma | Multiple myeloma and other hematologic indications | Multiple myeloma |
| Route | Oral | Subcutaneous or intravenous | Oral | Intravenous or subcutaneous |
| Major adverse effects | Thrombocytopenia, nausea, hyponatremia, fatigue | Peripheral neuropathy, thrombocytopenia | Myelosuppression, thrombosis, teratogenicity | Infusion reaction, infection risk |
| Mechanism uniqueness | Nuclear export inhibition | Proteasome blockade | Immunomodulation | Monoclonal antibody targeting |
Selinexor differs from bortezomib because it inhibits nuclear export rather than proteasome function. It differs from lenalidomide because it does not primarily act through cereblon-mediated immunomodulation. It differs from daratumumab because it is not a monoclonal antibody and does not target CD38. Its key exam identity is XPO1 inhibition, nuclear retention of tumor suppressor proteins, and apoptosis of malignant cells.
MCQs
- Selinexor belongs to which drug class?
a) Proteasome inhibitor
b) Selective inhibitor of nuclear export
c) Alkylating agent
d) Antimetabolite
Answer: b) Selective inhibitor of nuclear export
- The primary molecular target of selinexor is:
a) CD38
b) EGFR
c) XPO1/exportin 1
d) BCR-ABL
Answer: c) XPO1/exportin 1
- XPO1 is mainly involved in:
a) Nuclear export of proteins and RNA molecules
b) Bacterial cell wall synthesis
c) DNA topoisomerase inhibition
d) Insulin secretion
Answer: a) Nuclear export of proteins and RNA molecules
- Selinexor causes accumulation of tumor suppressor proteins in the:
a) Cytoplasm
b) Nucleus
c) Mitochondrial matrix only
d) Lysosome only
Answer: b) Nucleus
- Which cancer is a current major use of selinexor?
a) Multiple myeloma
b) Acute bacterial leukemia infection
c) Basal cell carcinoma only
d) Malaria-associated cancer
Answer: a) Multiple myeloma
- Selinexor reduces levels of which oncoproteins?
a) c-Myc and cyclin D1
b) Insulin and glucagon
c) Hemoglobin and albumin
d) Acetylcholine and dopamine
Answer: a) c-Myc and cyclin D1
- The final anticancer effect of selinexor includes:
a) Cell-cycle arrest and apoptosis
b) Increased platelet aggregation only
c) Increased bacterial killing
d) Direct bronchodilation
Answer: a) Cell-cycle arrest and apoptosis
- Selinexor is administered mainly by which route?
a) Oral
b) Intravenous
c) Intrathecal
d) Inhalational
Answer: a) Oral
- Which adverse effect is commonly associated with selinexor?
a) Thrombocytopenia
b) Severe ototoxicity
c) Gingival hyperplasia
d) Hypertrichosis
Answer: a) Thrombocytopenia
- Which electrolyte abnormality is clinically important with selinexor?
a) Hyponatremia
b) Hypercalcemia only
c) Hypermagnesemia only
d) Hypophosphatemia only
Answer: a) Hyponatremia
- Selinexor is commonly combined with which steroid in multiple myeloma regimens?
a) Dexamethasone
b) Hydrocortisone cream
c) Fludrocortisone only
d) Prednisolone eye drops
Answer: a) Dexamethasone
- Which statement about selinexor is correct?
a) It blocks XPO1 and retains tumor suppressor proteins in the nucleus
b) It blocks bacterial ribosomes
c) It is a beta-blocker
d) It directly replaces insulin
Answer: a) It blocks XPO1 and retains tumor suppressor proteins in the nucleus
- Which monitoring is important during selinexor therapy?
a) Complete blood count and serum sodium
b) Blood group only
c) Visual acuity only
d) Serum calcium only
Answer: a) Complete blood count and serum sodium
- Bortezomib differs from selinexor because bortezomib mainly inhibits:
a) Proteasome activity
b) XPO1 nuclear export
c) Estrogen receptor signaling
d) Sodium channels
Answer: a) Proteasome activity
- Selinexor’s former DLBCL accelerated approval indication was:
a) Withdrawn in 2026
b) Expanded to all lymphomas
c) Converted into an antibiotic indication
d) Used for type 1 diabetes
Answer: a) Withdrawn in 2026
FAQs
- What is selinexor used for?
Selinexor is used in selected adults with multiple myeloma, usually in combination with dexamethasone and sometimes with bortezomib depending on the treatment setting.
- What is the mechanism of action of selinexor?
Selinexor inhibits XPO1, also called exportin 1. This blocks nuclear export of tumor suppressor proteins and growth regulators, causing nuclear accumulation of tumor suppressor proteins, reduced oncoproteins, cell-cycle arrest, and apoptosis.
- What does XPO1 do?
XPO1 is a nuclear export protein that transports certain proteins and RNA molecules from the nucleus to the cytoplasm. Cancer cells may use this pathway to remove tumor suppressor proteins from the nucleus.
- Why does selinexor cause cancer cell death?
Selinexor keeps tumor suppressor proteins inside the nucleus, where they can restore cell-cycle control and trigger apoptosis. It also reduces cancer-promoting proteins such as c-Myc and cyclin D1.
- Is selinexor chemotherapy?
Selinexor is not traditional cytotoxic chemotherapy. It is a targeted anticancer drug and selective inhibitor of nuclear export.
- What are common side effects of selinexor?
Common side effects include nausea, vomiting, diarrhea, decreased appetite, weight loss, fatigue, thrombocytopenia, anemia, neutropenia, and hyponatremia.
- Why is thrombocytopenia important with selinexor?
Selinexor can reduce platelet counts, increasing bleeding risk. Regular complete blood count monitoring is important during treatment.
- Why is sodium monitoring important with selinexor?
Selinexor can cause hyponatremia, which may lead to weakness, confusion, dizziness, or neurological symptoms. Serum sodium should be monitored during therapy.
- Is selinexor still used for diffuse large B-cell lymphoma?
Selinexor’s accelerated approval indication for relapsed or refractory diffuse large B-cell lymphoma was withdrawn in 2026. Its multiple myeloma indications were not affected.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology
K.D. Tripathi Essentials of Medical Pharmacology
Harrison’s Principles of Internal Medicine
