
Table of Contents
Introduction
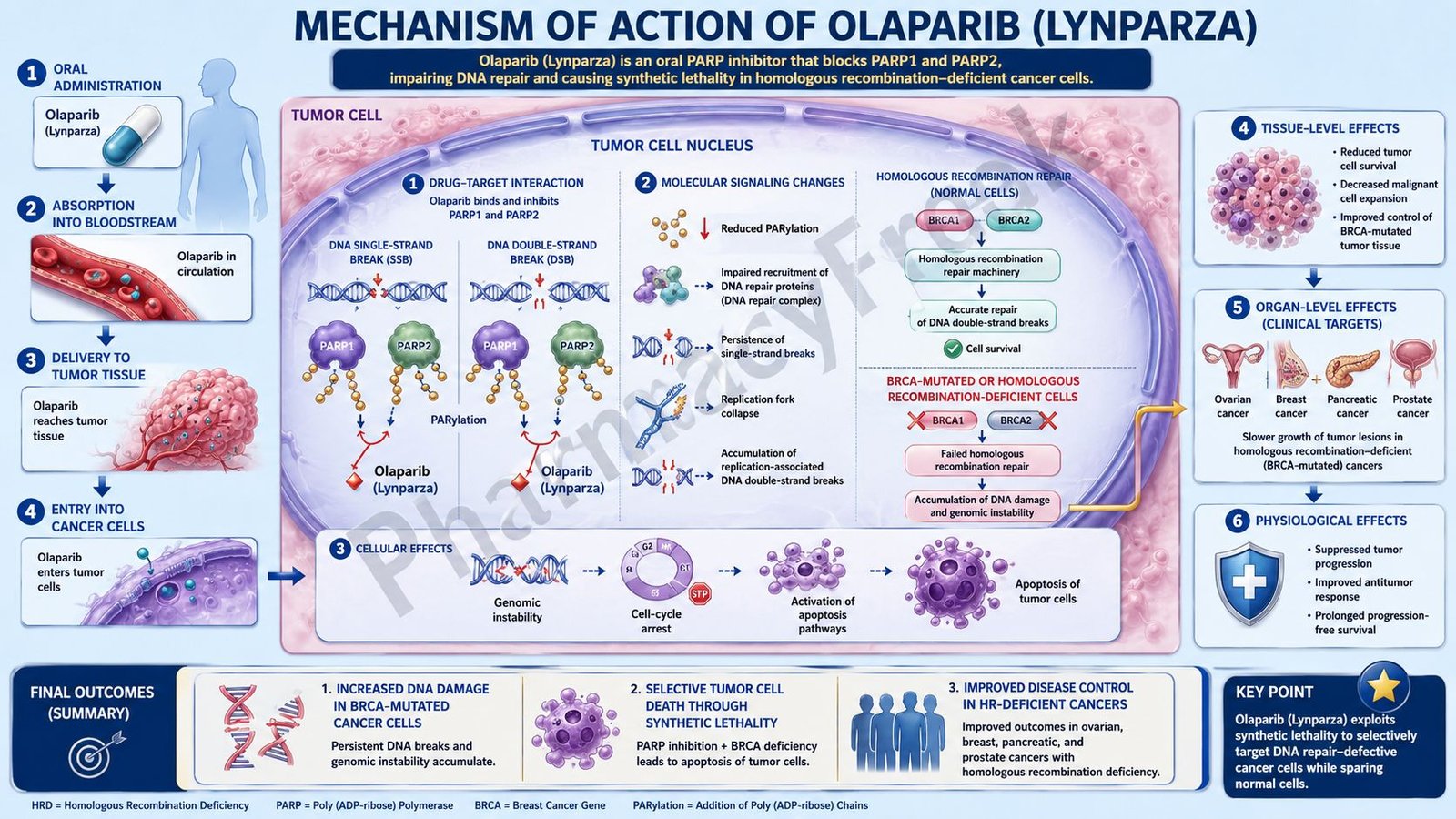
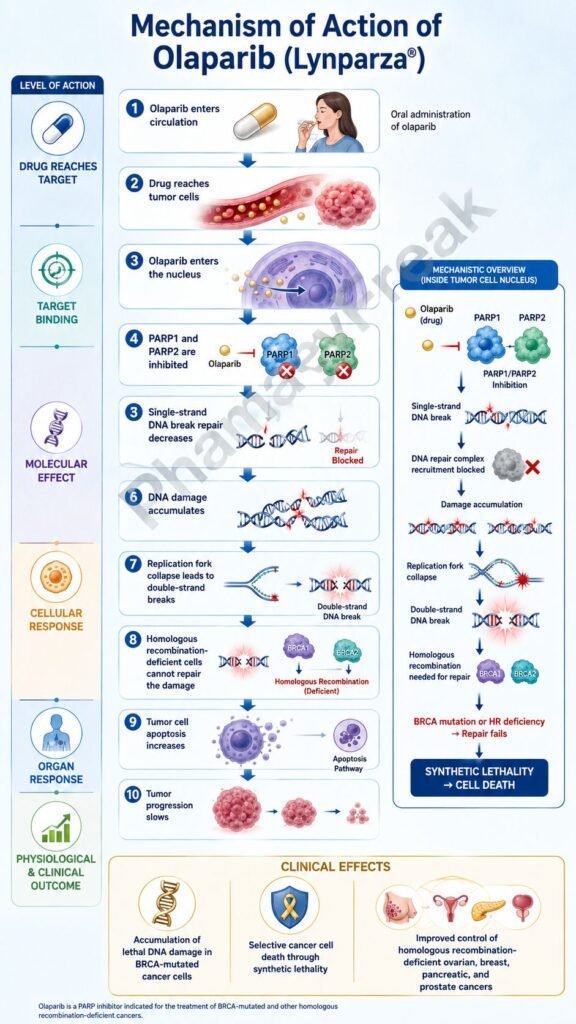
Olaparib is an oral anticancer drug that belongs to the poly ADP-ribose polymerase inhibitor class, commonly called PARP inhibitors. It is marketed under the brand name Lynparza. Olaparib is an important targeted anticancer drug used in cancers with defects in DNA repair pathways, especially BRCA1, BRCA2, and other homologous recombination repair gene abnormalities.
The central pharmacological idea behind olaparib is synthetic lethality. Normal cells can repair DNA damage through multiple repair pathways. However, cancer cells with BRCA or homologous recombination repair defects already have a weakened ability to repair double-strand DNA breaks. When olaparib blocks PARP-mediated repair of single-strand DNA breaks, DNA damage accumulates, replication forks collapse, double-strand breaks increase, and cancer cells undergo death.
Olaparib is especially exam-relevant because it connects molecular oncology with pharmacology. It does not act like traditional cytotoxic chemotherapy that broadly damages all rapidly dividing cells. Instead, it exploits a specific DNA repair weakness in tumor cells. However, it can still cause serious adverse effects such as anemia, myelosuppression, myelodysplastic syndrome, acute myeloid leukemia, pneumonitis, venous thromboembolism, hepatotoxicity, and embryo-fetal toxicity. The current U.S. label lists olaparib as a PARP inhibitor indicated in selected ovarian, breast, pancreatic, and prostate cancers based on biomarker status and clinical setting.
Mechanism of Action (Step-wise)
Step 1: DNA damage occurs continuously in cells
Cells are constantly exposed to DNA damage from normal metabolism, oxidative stress, radiation, chemicals, and replication errors. Single-strand DNA breaks are among the most common forms of DNA injury. If these breaks are not repaired properly, they can interfere with DNA replication and cell survival.
Step 2: PARP enzymes detect DNA single-strand breaks
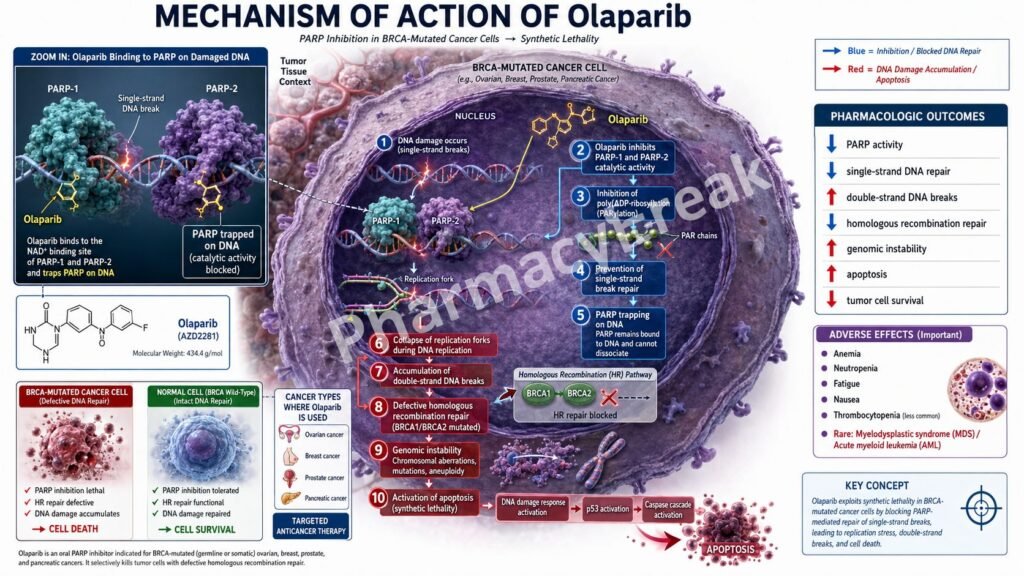
Poly ADP-ribose polymerase enzymes, especially PARP1 and PARP2, detect single-strand DNA breaks. PARP3 also contributes to DNA repair-related processes. These enzymes bind to damaged DNA and help recruit repair proteins to the site of injury. Olaparib inhibits PARP1, PARP2, and PARP3.
Step 3: PARP uses NAD+ to form poly ADP-ribose chains
After binding damaged DNA, PARP enzymes use nicotinamide adenine dinucleotide, or NAD+, to add poly ADP-ribose chains to themselves and other proteins. This process is called PARylation. PARylation acts like a molecular signal that attracts DNA repair proteins.
Step 4: Base excision repair is supported by PARP activity
PARP activity is especially important in base excision repair and repair of single-strand DNA breaks. When PARP works normally, damaged DNA is recognized, repair proteins are recruited, and DNA integrity is restored.
Step 5: Olaparib inhibits PARP catalytic activity
Olaparib binds to the catalytic domain of PARP enzymes and inhibits their enzymatic activity. This prevents proper PARylation and reduces recruitment of DNA repair machinery. As a result, single-strand DNA breaks are not repaired efficiently.
Step 6: PARP-DNA trapping increases DNA damage
Olaparib not only inhibits PARP enzyme activity but may also increase formation of PARP-DNA complexes. These trapped complexes block normal DNA replication and create physical obstacles at the replication fork. This is called PARP trapping and is an important mechanism of cytotoxicity.
Step 7: Single-strand breaks convert into double-strand breaks
During DNA replication, unrepaired single-strand breaks can become double-strand DNA breaks. Double-strand breaks are much more dangerous for the cell because both strands of DNA are damaged.
Step 8: Normal cells repair double-strand breaks by homologous recombination
Healthy cells often repair double-strand DNA breaks using homologous recombination repair. This pathway requires functional BRCA1, BRCA2, PALB2, RAD51, and related homologous recombination repair proteins. Homologous recombination is an accurate repair process because it uses the sister chromatid as a template.
Step 9: BRCA-mutated tumor cells cannot repair double-strand breaks properly
Cancer cells with BRCA1 or BRCA2 mutations are defective in homologous recombination repair. Other homologous recombination repair gene defects can produce similar vulnerability. When olaparib causes accumulation of DNA breaks in these cells, they cannot repair the damage effectively.
Step 10: Synthetic lethality occurs
Synthetic lethality means that loss of either one repair pathway alone may be tolerated, but loss of two complementary repair mechanisms causes cell death. In BRCA-mutated cells, homologous recombination is already impaired. Olaparib then blocks PARP-dependent repair. Together, these defects lead to lethal DNA damage in cancer cells.
Step 11: Cancer cell death occurs
Accumulated DNA damage causes replication fork collapse, genomic instability, cell-cycle arrest, and apoptosis. The final therapeutic outcome is selective killing or growth inhibition of tumor cells with DNA repair defects.
Step 12: Platinum sensitivity is pharmacologically relevant
Tumors that respond to platinum-based chemotherapy often have DNA repair weakness. This is why olaparib is commonly used as maintenance therapy after platinum response in selected ovarian and pancreatic cancer settings. Platinum drugs create DNA damage, and PARP inhibition further exploits impaired DNA repair.
Step 13: In prostate cancer, androgen receptor interaction may contribute
In prostate cancer models, PARP1 has been shown to contribute to androgen receptor activity regulation. Combining olaparib with androgen receptor pathway inhibition, such as abiraterone, may increase antitumor activity in selected BRCA-mutated metastatic castration-resistant prostate cancer.
Pharmacokinetics
Olaparib is administered orally as tablets. The usual recommended tablet dose in adults is 300 mg twice daily with or without food, depending on indication and tolerance. The tablets should be swallowed whole and should not be chewed, crushed, dissolved, or divided.
After oral administration, olaparib reaches peak plasma concentration in about 1.5 hours. A high-fat, high-calorie meal may slow absorption but does not significantly change the overall extent of absorption. This is why it may be taken with or without food.
Olaparib is approximately 82% protein bound. Its terminal plasma half-life is about 14.9 hours after a single 300 mg dose, supporting twice-daily dosing.
Olaparib is metabolized mainly by CYP3A enzymes. Strong or moderate CYP3A inhibitors can increase olaparib exposure and increase adverse effects, so they should generally be avoided or require dose adjustment. Strong or moderate CYP3A inducers can reduce olaparib exposure and may reduce efficacy, so they should also generally be avoided.
Olaparib is eliminated through both urine and feces, mostly as metabolites. Moderate renal impairment requires dose reduction. There are limited data in severe renal impairment or end-stage renal disease. Mild or moderate hepatic impairment does not require starting dose adjustment, but there are limited data in severe hepatic impairment.
Clinical Uses
Olaparib is used in selected cancers where DNA repair defects make tumor cells vulnerable to PARP inhibition. Patient selection commonly depends on BRCA mutation, homologous recombination deficiency, or homologous recombination repair gene mutation status.
In ovarian cancer, olaparib is used as maintenance treatment in adults with deleterious or suspected deleterious germline or somatic BRCA-mutated advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in complete or partial response to first-line platinum-based chemotherapy.
Olaparib is also used with bevacizumab as first-line maintenance treatment in adults with advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer who respond to first-line platinum-based chemotherapy and whose cancer is homologous recombination deficiency-positive. HRD-positive status may be defined by BRCA mutation and/or genomic instability.
In recurrent ovarian cancer, olaparib is used as maintenance therapy in adults with germline or somatic BRCA-mutated recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in complete or partial response to platinum-based chemotherapy.
In breast cancer, olaparib is used as adjuvant treatment in adults with deleterious or suspected deleterious germline BRCA-mutated, HER2-negative, high-risk early breast cancer who have already received neoadjuvant or adjuvant chemotherapy. It is also used in adults with germline BRCA-mutated, HER2-negative metastatic breast cancer who have received chemotherapy in the neoadjuvant, adjuvant, or metastatic setting. Hormone receptor-positive patients should have received endocrine therapy or be considered inappropriate for endocrine therapy.
In pancreatic cancer, olaparib is used as maintenance treatment in adults with germline BRCA-mutated metastatic pancreatic adenocarcinoma whose disease has not progressed after at least 16 weeks of first-line platinum-based chemotherapy.
In prostate cancer, olaparib is used in adults with germline or somatic homologous recombination repair gene-mutated metastatic castration-resistant prostate cancer who have progressed after enzalutamide or abiraterone. It is also used with abiraterone and prednisone or prednisolone for adults with BRCA-mutated metastatic castration-resistant prostate cancer.
Adverse Effects
The most important adverse effect of olaparib is hematological toxicity. Anemia is especially common and may require dose interruption, dose reduction, transfusion, or discontinuation depending on severity. Neutropenia, leukopenia, thrombocytopenia, and lymphopenia may also occur.
Myelodysplastic syndrome and acute myeloid leukemia are rare but serious warnings. The label reports MDS/AML in approximately 1.2% of exposed patients across approved cancer settings, with many cases fatal. Complete blood count monitoring is recommended at baseline and monthly during treatment.
Pneumonitis, including severe and fatal cases, can occur. New or worsening dyspnea, cough, fever, or radiological lung abnormalities should prompt interruption and evaluation. If pneumonitis is confirmed, olaparib should be discontinued.
Venous thromboembolism, including pulmonary embolism, is an important warning, especially in metastatic castration-resistant prostate cancer. Patients should be monitored for symptoms such as leg swelling, chest pain, shortness of breath, or sudden unexplained hypoxia.
Hepatotoxicity, including drug-induced liver injury, has been reported. Liver enzymes and bilirubin should be monitored at baseline and during treatment, especially if symptoms or abnormal liver tests occur. If drug-induced liver injury is confirmed, olaparib should be discontinued.
Common adverse effects include nausea, vomiting, fatigue, asthenia, anemia, diarrhea, decreased appetite, dysgeusia, headache, dizziness, cough, abdominal pain, constipation, stomatitis, rash, and laboratory abnormalities such as decreased hemoglobin, decreased lymphocytes, decreased neutrophils, and decreased platelets.
Olaparib can cause embryo-fetal toxicity based on its mechanism and animal data. Females of reproductive potential should use effective contraception during treatment and for 6 months after the last dose. Male patients with female partners of reproductive potential or pregnant partners should use effective contraception during treatment and for 3 months after the last dose.
Comparative Analysis
Olaparib is one of several PARP inhibitors used in oncology. Other important drugs in this class include niraparib, rucaparib, and talazoparib. All inhibit PARP-related DNA repair, but they differ in approved uses, toxicity profile, dosing, and relative PARP-trapping potency.
Compared with niraparib, olaparib is more strongly associated with biomarker-selected BRCA or homologous recombination repair settings in several indications. Niraparib is also used in ovarian cancer maintenance settings and is notable for thrombocytopenia, hypertension, and individualized starting-dose considerations.
Compared with rucaparib, olaparib has a broader range of major approved indications across ovarian, breast, pancreatic, and prostate cancer. Rucaparib is also a PARP inhibitor but its approved use and regulatory history differ by country and indication.
Compared with talazoparib, olaparib has less emphasis on extreme PARP-trapping potency. Talazoparib is considered a potent PARP-trapping drug and is used in selected breast and prostate cancer settings. Both drugs exploit homologous recombination repair deficiency.
Compared with platinum chemotherapy, olaparib is more targeted. Platinum drugs directly create DNA cross-links and broad DNA damage, while olaparib prevents repair of DNA breaks and is especially effective when homologous recombination repair is defective. Platinum sensitivity often predicts benefit from PARP inhibition in some tumors.
Compared with classic antimetabolites such as methotrexate, 5-fluorouracil, or cytarabine, olaparib does not primarily block nucleotide synthesis. Instead, it blocks DNA repair enzyme activity and traps PARP on DNA, causing lethal DNA damage in susceptible cancer cells.
Compared with monoclonal antibodies such as bevacizumab, olaparib acts inside tumor cells on DNA repair. Bevacizumab blocks vascular endothelial growth factor and reduces tumor angiogenesis. The combination of olaparib with bevacizumab is used in selected HRD-positive ovarian cancer maintenance therapy because the two drugs target different cancer survival mechanisms.
MCQs
- Olaparib belongs to which pharmacological class?
a) PARP inhibitor
b) EGFR inhibitor
c) Aromatase inhibitor
d) Proteasome inhibitor
Answer: a) PARP inhibitor
- The brand name of olaparib is:
a) Lynparza
b) Tasigna
c) Ibrance
d) Keytruda
Answer: a) Lynparza
- Olaparib mainly inhibits which enzymes?
a) PARP1, PARP2, and PARP3
b) COX-1 and COX-2
c) ACE and renin
d) HMG-CoA reductase
Answer: a) PARP1, PARP2, and PARP3
- PARP enzymes are mainly involved in:
a) DNA repair
b) Dopamine synthesis
c) Insulin secretion
d) Bile acid absorption
Answer: a) DNA repair
- The key pharmacological concept behind olaparib activity in BRCA-mutated tumors is:
a) Competitive antagonism
b) Synthetic lethality
c) Enzyme induction
d) Receptor desensitization
Answer: b) Synthetic lethality
- BRCA1 and BRCA2 are mainly involved in which DNA repair pathway?
a) Homologous recombination repair
b) Mismatch repair only
c) Histamine degradation
d) Ribosomal RNA synthesis
Answer: a) Homologous recombination repair
- PARP inhibition in BRCA-deficient cells leads to:
a) Accumulation of DNA damage and cancer cell death
b) Increased repair of double-strand breaks
c) Complete protection from chemotherapy toxicity
d) Increased bacterial cell wall synthesis
Answer: a) Accumulation of DNA damage and cancer cell death
- Which cancer type is an important approved use of olaparib in selected patients?
a) BRCA-mutated ovarian cancer
b) Acute bacterial pneumonia
c) Type 1 diabetes mellitus
d) Essential hypertension
Answer: a) BRCA-mutated ovarian cancer
- Olaparib is used as maintenance therapy in germline BRCA-mutated metastatic pancreatic adenocarcinoma after:
a) No prior therapy of any kind
b) Disease has not progressed after first-line platinum-based chemotherapy
c) Failure of all antibiotics
d) Prior thyroid hormone therapy
Answer: b) Disease has not progressed after first-line platinum-based chemotherapy
- Which adverse effect is especially important with olaparib?
a) Anemia
b) Gingival hyperplasia
c) Ototoxicity in all patients
d) Severe hypoglycemia
Answer: a) Anemia
- Which serious hematologic complication is associated with olaparib?
a) Myelodysplastic syndrome and acute myeloid leukemia
b) Sickle cell trait conversion
c) Hemophilia A
d) Polycythemia vera cure
Answer: a) Myelodysplastic syndrome and acute myeloid leukemia
- Olaparib is metabolized mainly by:
a) CYP3A
b) CYP2D6 only
c) Acetylcholinesterase
d) Xanthine oxidase
Answer: a) CYP3A
- Strong CYP3A inhibitors can:
a) Increase olaparib exposure and toxicity
b) Completely block olaparib absorption forever
c) Convert olaparib into aspirin
d) Eliminate the need for monitoring
Answer: a) Increase olaparib exposure and toxicity
- Which warning is associated with olaparib therapy?
a) Pneumonitis
b) Irreversible cataract in all patients
c) Mandatory severe hypercalcemia
d) Acute opioid withdrawal
Answer: a) Pneumonitis
- Which contraception advice is correct for olaparib?
a) It may cause fetal harm, so effective contraception is required according to product guidance
b) It is completely safe during pregnancy
c) It is used to improve fertility
d) It has no effect on embryo-fetal development
Answer: a) It may cause fetal harm, so effective contraception is required according to product guidance
FAQs
What is the mechanism of action of olaparib?
Olaparib inhibits PARP enzymes, especially PARP1, PARP2, and PARP3. This blocks repair of single-strand DNA breaks, increases PARP-DNA trapping, causes accumulation of DNA damage, and leads to cancer cell death, especially in BRCA or homologous recombination repair-deficient tumors.
What is the brand name of olaparib?
The brand name of olaparib is Lynparza.
Why is olaparib effective in BRCA-mutated cancers?
BRCA-mutated cancer cells have defective homologous recombination repair. When olaparib blocks PARP-dependent DNA repair, DNA damage accumulates beyond the cell’s ability to repair it. This causes synthetic lethality and cancer cell death.
Is olaparib chemotherapy?
Olaparib is not traditional cytotoxic chemotherapy. It is a targeted anticancer drug that inhibits DNA repair enzymes. However, it can still cause serious toxicities such as anemia, myelosuppression, MDS/AML, pneumonitis, and embryo-fetal toxicity.
Which cancers is olaparib used for?
Olaparib is used in selected ovarian, breast, pancreatic, and prostate cancers. Use depends on cancer type, disease stage, prior therapy, BRCA or HRR/HRD biomarker status, and whether it is being used alone or in combination.
What is the most important adverse effect of olaparib?
Anemia and other hematological toxicities are very important. Rare but serious myelodysplastic syndrome and acute myeloid leukemia can occur, so complete blood count monitoring is required.
Does olaparib interact with CYP3A drugs?
Yes. Olaparib is metabolized mainly by CYP3A. Strong or moderate CYP3A inhibitors can increase olaparib exposure, while strong or moderate CYP3A inducers can reduce its effectiveness.
Can olaparib be used in pregnancy?
Olaparib can cause fetal harm and should generally be avoided during pregnancy. Effective contraception is required during treatment and for the recommended period after the last dose.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

