
Table of Contents
Introduction
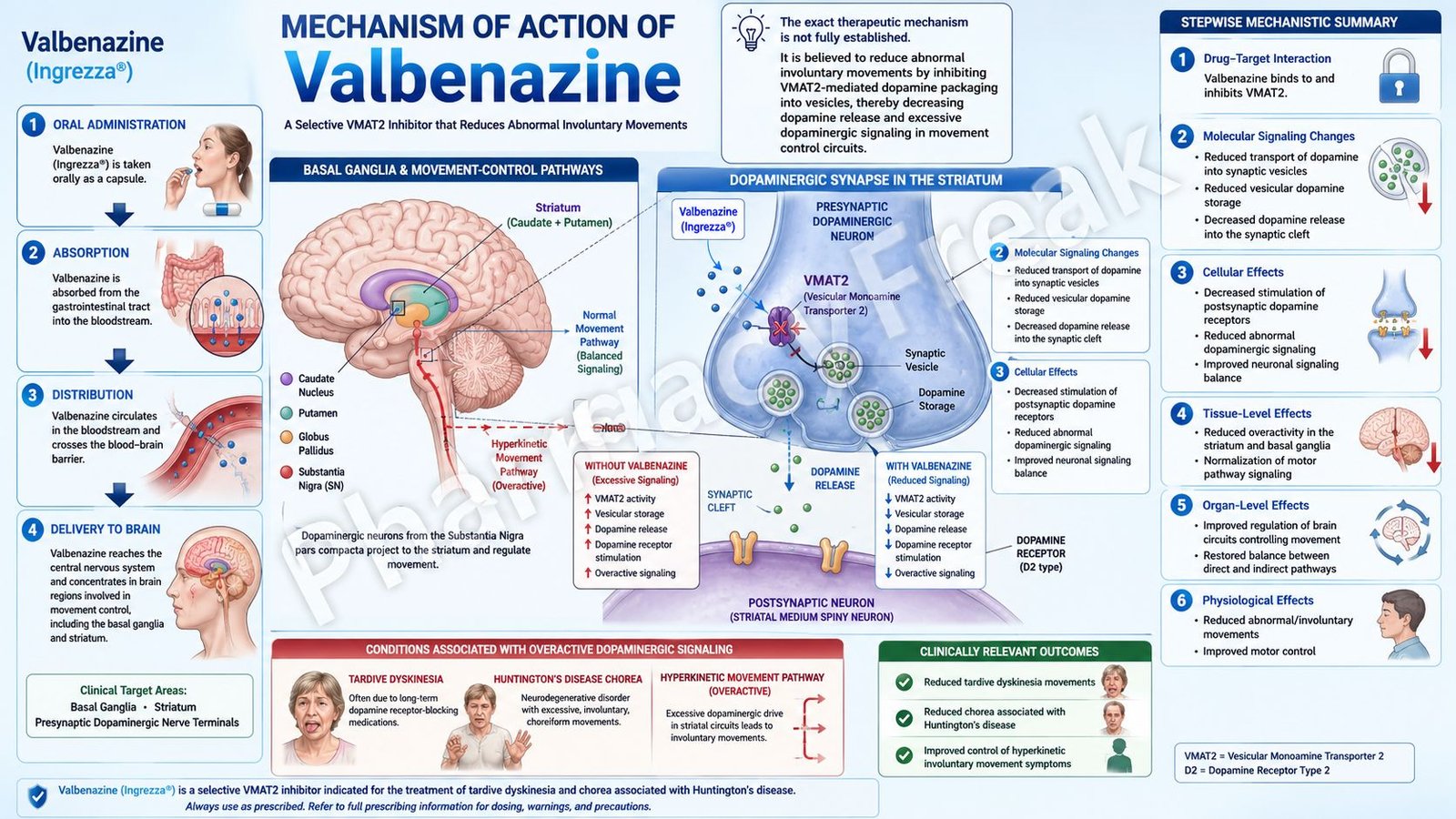
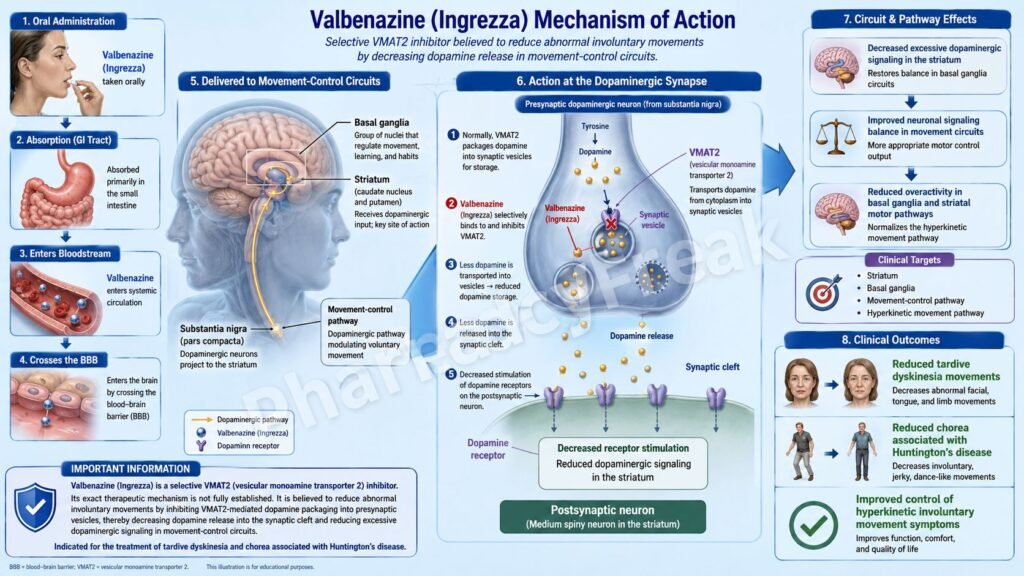
Valbenazine is an oral drug used for the treatment of abnormal involuntary movements. It is marketed under the brand names Ingrezza and Ingrezza Sprinkle. Pharmacologically, valbenazine is a vesicular monoamine transporter 2 inhibitor, commonly abbreviated as a VMAT2 inhibitor.
Valbenazine is mainly used in adults with tardive dyskinesia and chorea associated with Huntington’s disease. Tardive dyskinesia is a movement disorder that usually occurs after long-term exposure to dopamine receptor-blocking drugs, especially antipsychotics and some antiemetics. It commonly presents with involuntary movements of the face, tongue, lips, trunk, or limbs.
Chorea associated with Huntington’s disease is characterized by irregular, unpredictable, involuntary movements due to degeneration of brain areas involved in motor control, especially basal ganglia circuits. Valbenazine does not cure Huntington’s disease or reverse neurodegeneration, but it can reduce choreic movements in appropriate adult patients.
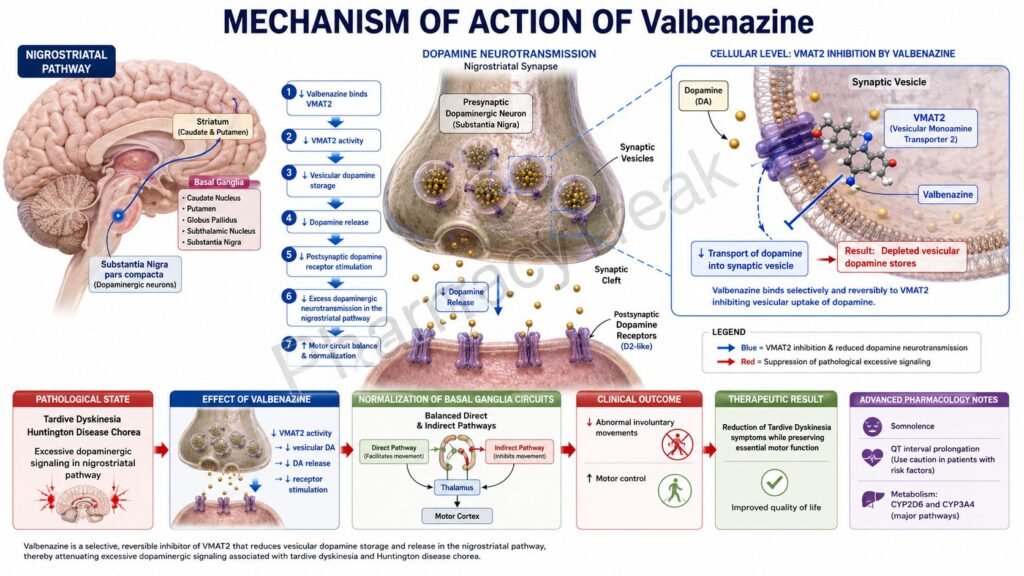
The exact therapeutic mechanism of valbenazine in tardive dyskinesia and Huntington’s disease-associated chorea is not fully established. However, its clinical effect is thought to occur mainly through reversible inhibition of VMAT2, which reduces presynaptic monoamine packaging and decreases dopamine release in motor pathways. Ingrezza and Ingrezza Sprinkle are currently labeled as VMAT2 inhibitors for adults with tardive dyskinesia and chorea associated with Huntington’s disease.
Mechanism of Action (Step-wise)
Step 1: Dopamine signaling is involved in movement control
Normal voluntary movement depends on balanced signaling in the basal ganglia. Dopamine plays a major role in regulating motor pathways, especially in circuits connecting the striatum, globus pallidus, substantia nigra, thalamus, and motor cortex.
Step 2: Excess dopaminergic activity contributes to abnormal movements
In tardive dyskinesia, chronic dopamine D2 receptor blockade may lead to dopamine receptor supersensitivity and abnormal motor signaling. This can produce repetitive, involuntary, purposeless movements. In Huntington’s disease-associated chorea, altered basal ganglia function also produces excessive and poorly controlled motor output.
Step 3: Monoamines are stored in presynaptic vesicles
Before dopamine and other monoamines are released into the synaptic cleft, they must be transported from the neuronal cytoplasm into synaptic vesicles. This vesicular storage is essential because neurotransmitters are released by exocytosis from these vesicles.
Step 4: VMAT2 transports monoamines into vesicles
Vesicular monoamine transporter 2, or VMAT2, is located on synaptic vesicles in monoaminergic neurons. It transports monoamines such as dopamine, norepinephrine, serotonin, and histamine from the cytoplasm into storage vesicles.
Step 5: Valbenazine reversibly inhibits VMAT2
Valbenazine inhibits VMAT2 reversibly. By inhibiting VMAT2, valbenazine reduces the transport of monoamines into synaptic vesicles. Since fewer dopamine molecules are packaged into vesicles, less dopamine is available for release during neuronal firing.
Step 6: Dopamine release into synapses is reduced
The clinically important effect is reduced presynaptic dopamine release in motor circuits. This helps decrease excessive dopaminergic signaling in basal ganglia pathways involved in involuntary movements.
Step 7: Active metabolite contributes strongly to VMAT2 inhibition
Valbenazine is converted to the active metabolite [+]-alpha-dihydrotetrabenazine, also called [+]-alpha-HTBZ. This metabolite has high affinity for human VMAT2 and contributes significantly to the drug’s therapeutic effect. Valbenazine and its active metabolite have no appreciable binding affinity for dopamine D2, serotonin, adrenergic, histamine, or muscarinic receptors, making VMAT2 inhibition the key pharmacological action.
Step 8: Abnormal involuntary movements decrease
By reducing vesicular dopamine storage and dopamine release, valbenazine helps reduce involuntary movements in tardive dyskinesia and chorea associated with Huntington’s disease.
Step 9: The drug does not directly block dopamine receptors
A useful exam point is that valbenazine does not work by directly blocking dopamine receptors like antipsychotics. Instead, it reduces presynaptic dopamine availability by inhibiting VMAT2. This distinction is important because dopamine receptor blockers can worsen or cause tardive dyskinesia, while VMAT2 inhibitors can treat it.
Step 10: Therapeutic benefit is symptomatic
Valbenazine improves abnormal movement symptoms, but it does not remove the underlying cause of tardive dyskinesia or stop the progression of Huntington’s disease. Its role is symptomatic control of involuntary movements.
Pharmacokinetics
Valbenazine is administered orally once daily. It is available as Ingrezza capsules and Ingrezza Sprinkle capsules. Ingrezza Sprinkle can be swallowed whole or opened and sprinkled over soft food when swallowing capsules is difficult, but it should not be crushed, chewed, or administered through enteral feeding tubes according to labeling instructions.
Valbenazine may be taken with or without food. After oral administration, valbenazine reaches peak plasma concentration in about 0.5 to 1 hour. Steady-state plasma concentrations are reached within about 1 week. The absolute oral bioavailability is approximately 49%.
Valbenazine is extensively metabolized. One important pathway is hydrolysis of the valine ester to form the active metabolite [+]-alpha-HTBZ. Another pathway is oxidative metabolism, mainly through CYP3A4 and CYP3A5. The active metabolite is further metabolized partly by CYP2D6.
The half-life of valbenazine and its active metabolite is approximately 15 to 22 hours, supporting once-daily dosing. Valbenazine is more than 99% protein bound, while the active metabolite is approximately 64% protein bound.
Excretion occurs through both urine and feces. About 60% of administered radioactivity is recovered in urine and about 30% in feces, but less than 2% is excreted as unchanged valbenazine or active metabolite.
Drug interactions are clinically important. Monoamine oxidase inhibitors should generally be avoided because they may increase monoamine-related effects. Strong CYP3A4 inducers are not recommended because they can reduce valbenazine exposure and decrease efficacy. Strong CYP3A4 inhibitors and strong CYP2D6 inhibitors may increase exposure and require dose reduction. Known CYP2D6 poor metabolizers also require lower recommended dosing due to increased active metabolite exposure. Moderate or severe hepatic impairment also requires dose reduction, while renal dose adjustment is generally not required for mild, moderate, or severe renal impairment.
Clinical Uses
Valbenazine is used for the treatment of tardive dyskinesia in adults. Tardive dyskinesia is commonly associated with long-term use of dopamine receptor-blocking medications, especially antipsychotics used in schizophrenia, bipolar disorder, depression augmentation, and other psychiatric conditions.
Valbenazine is also used for chorea associated with Huntington’s disease in adults. In this setting, it reduces choreic movements but does not treat the genetic cause or slow the neurodegenerative process of Huntington’s disease.
In clinical practice, valbenazine is useful because it can reduce movement severity while often allowing continued treatment of the underlying psychiatric condition when stopping antipsychotic therapy is not feasible. This is important because abruptly stopping antipsychotic therapy may destabilize psychiatric illness in some patients.
Valbenazine is not approved for pediatric patients, and its safety and effectiveness have not been established in children. It is also not a general treatment for Parkinson’s disease, essential tremor, restless legs syndrome, dystonia unrelated to tardive dyskinesia, or all forms of drug-induced movement disorders.
Adverse Effects
The most common adverse effect of valbenazine in tardive dyskinesia is somnolence. Patients should be warned about sedation and should avoid driving or operating hazardous machinery until they know how the drug affects them.
In chorea associated with Huntington’s disease, common adverse effects include somnolence, lethargy, sedation, urticaria, rash, and insomnia. Because Huntington’s disease itself is associated with psychiatric symptoms, careful monitoring is especially important.
Valbenazine has a boxed warning for depression and suicidal ideation and behavior in patients with Huntington’s disease. VMAT2 inhibitors can increase the risk of depression and suicidal thoughts or behaviors in these patients. Patients, caregivers, and families should monitor for new or worsening depression, suicidal ideation, or unusual behavior changes.
QT prolongation is another important safety warning. At usual concentrations, QT prolongation is generally not clinically significant in most patients, but the risk can become more important in CYP2D6 poor metabolizers, patients taking strong CYP2D6 inhibitors, or patients taking strong CYP3A4 inhibitors. Valbenazine should be avoided in patients with congenital long QT syndrome or arrhythmias associated with prolonged QT interval.
Hypersensitivity reactions may occur, including rash, urticaria, and angioedema involving the face, lips, mouth, eyelids, larynx, or glottis. Angioedema involving the airway can be serious or fatal, so valbenazine should be discontinued if clinically significant hypersensitivity occurs.
Neuroleptic malignant syndrome has been reported with VMAT2 inhibitors. Symptoms may include hyperthermia, severe muscle rigidity, altered mental status, autonomic instability, elevated creatine kinase, and leukocytosis. If suspected, valbenazine should be stopped and urgent medical evaluation is required.
Parkinsonism can occur with valbenazine and other VMAT2 inhibitors. Symptoms may include bradykinesia, rigidity, tremor, gait disturbance, drooling, or falls. Dose reduction or discontinuation may be required if clinically significant parkinson-like symptoms develop.
Pregnancy may involve fetal risk based on animal data, and breastfeeding is not recommended during treatment and for 5 days after the final dose according to product guidance.
Comparative Analysis
Valbenazine is commonly compared with deutetrabenazine and tetrabenazine because all are VMAT2 inhibitors used for hyperkinetic movement disorders.
Valbenazine is a selective VMAT2 inhibitor with once-daily dosing. It is approved for adults with tardive dyskinesia and chorea associated with Huntington’s disease. Its active metabolite, [+]-alpha-HTBZ, contributes strongly to VMAT2 inhibition.
Deutetrabenazine is another VMAT2 inhibitor used for tardive dyskinesia and chorea associated with Huntington’s disease. It is chemically related to tetrabenazine but contains deuterium, which slows metabolism and allows more stable drug exposure. Deutetrabenazine is usually dosed once or twice daily depending on formulation and indication.
Tetrabenazine is an older VMAT2 inhibitor used mainly for chorea associated with Huntington’s disease. It has a shorter duration of action and often requires multiple daily dosing. It also has important warnings for depression, suicidality, parkinsonism, akathisia, and sedation.
Compared with antipsychotics, valbenazine does not directly block dopamine D2 receptors. This is an important distinction because dopamine receptor blockers may cause or worsen tardive dyskinesia, while valbenazine treats tardive dyskinesia by reducing presynaptic dopamine release.
Compared with benzodiazepines, valbenazine is more mechanism-specific for tardive dyskinesia and Huntington’s chorea. Benzodiazepines may reduce anxiety or muscle activity in some movement disorders, but they do not specifically target VMAT2 and commonly cause sedation, dependence, and cognitive impairment.
Compared with anticholinergic drugs such as benztropine, valbenazine is more appropriate for tardive dyskinesia. Anticholinergics may help drug-induced parkinsonism or acute dystonia, but they can worsen tardive dyskinesia in some patients and are not the preferred mechanism-based treatment for TD.
MCQs
- Valbenazine belongs to which pharmacological class?
a) VMAT2 inhibitor
b) Dopamine D2 receptor agonist
c) Acetylcholinesterase inhibitor
d) NMDA receptor antagonist
Answer: a) VMAT2 inhibitor
- The main brand name of valbenazine is:
a) Austedo
b) Ingrezza
c) Xenazine
d) Clozaril
Answer: b) Ingrezza
- Valbenazine is mainly used for the treatment of:
a) Essential hypertension
b) Tardive dyskinesia and Huntington’s disease-associated chorea
c) Acute bacterial meningitis
d) Myasthenia gravis
Answer: b) Tardive dyskinesia and Huntington’s disease-associated chorea
- The exact therapeutic mechanism of valbenazine is:
a) Completely unrelated to monoamines
b) Fully established as direct D2 receptor blockade
c) Not fully established, but thought to involve reversible VMAT2 inhibition
d) Based only on acetylcholine receptor stimulation
Answer: c) Not fully established, but thought to involve reversible VMAT2 inhibition
- VMAT2 normally functions to:
a) Transport monoamines into synaptic vesicles
b) Break down acetylcholine in the synaptic cleft
c) Block sodium channels in axons
d) Activate opioid receptors
Answer: a) Transport monoamines into synaptic vesicles
- Valbenazine reduces abnormal movements mainly by decreasing synaptic release of:
a) Dopamine
b) Insulin
c) Histamine from mast cells only
d) Acetylcholine at neuromuscular junctions
Answer: a) Dopamine
- Which active metabolite contributes to valbenazine’s action?
a) Morphine-6-glucuronide
b) N-desmethylclozapine
c) [+]-alpha-dihydrotetrabenazine
d) Norfluoxetine
Answer: c) [+]-alpha-dihydrotetrabenazine
- Valbenazine differs from antipsychotics because it:
a) Directly blocks dopamine D2 receptors
b) Inhibits VMAT2 instead of directly blocking dopamine receptors
c) Is used only as an antibiotic
d) Stimulates serotonin 5-HT2A receptors
Answer: b) Inhibits VMAT2 instead of directly blocking dopamine receptors
- Which adverse effect is commonly associated with valbenazine?
a) Somnolence
b) Severe hypoglycemia
c) Ototoxicity in all patients
d) Gingival hyperplasia
Answer: a) Somnolence
- Which boxed warning is especially relevant when valbenazine is used in Huntington’s disease?
a) Depression and suicidal ideation and behavior
b) Severe neutropenia in all patients
c) Fatal hypoglycemia
d) Irreversible pulmonary fibrosis
Answer: a) Depression and suicidal ideation and behavior
- Which cardiac safety issue is associated with valbenazine?
a) QT prolongation
b) Complete prevention of arrhythmia
c) Mandatory heart failure in all patients
d) Severe hypertension crisis after every dose
Answer: a) QT prolongation
- Valbenazine is metabolized partly through which enzyme system?
a) CYP3A4/5 and CYP2D6 pathways
b) Acetylcholinesterase only
c) Cyclooxygenase-1 only
d) Xanthine oxidase only
Answer: a) CYP3A4/5 and CYP2D6 pathways
- Which concomitant drug class should generally be avoided with valbenazine because of monoamine-related interaction concerns?
a) Monoamine oxidase inhibitors
b) Penicillin antibiotics
c) Proton pump inhibitors
d) Inhaled corticosteroids
Answer: a) Monoamine oxidase inhibitors
- Which adverse motor effect can occur with valbenazine?
a) Parkinsonism
b) Permanent paralysis after every dose
c) Myasthenic crisis in all patients
d) Acute demyelination
Answer: a) Parkinsonism
- Which statement about valbenazine is correct?
a) It cures Huntington’s disease permanently
b) It is a symptomatic treatment for chorea associated with Huntington’s disease
c) It is approved for all pediatric movement disorders
d) It directly reverses genetic degeneration in Huntington’s disease
Answer: b) It is a symptomatic treatment for chorea associated with Huntington’s disease
FAQs
What is the mechanism of action of valbenazine?
The exact therapeutic mechanism is not fully established, but valbenazine is thought to work by reversible inhibition of VMAT2. This reduces monoamine storage in synaptic vesicles and decreases dopamine release in motor pathways.
What is the brand name of valbenazine?
Valbenazine is marketed under the brand names Ingrezza and Ingrezza Sprinkle.
What is VMAT2?
VMAT2 stands for vesicular monoamine transporter 2. It transports monoamines such as dopamine, norepinephrine, serotonin, and histamine into synaptic vesicles for storage and release.
Why is valbenazine useful in tardive dyskinesia?
Tardive dyskinesia involves abnormal involuntary movements linked to altered dopamine signaling. Valbenazine reduces presynaptic dopamine release by inhibiting VMAT2, helping reduce involuntary movements.
Does valbenazine cure Huntington’s disease?
No. Valbenazine does not cure Huntington’s disease or stop neurodegeneration. It is used to reduce chorea symptoms associated with Huntington’s disease in adults.
What is the most important warning with valbenazine in Huntington’s disease?
The most important warning is depression and suicidal ideation or behavior. Patients with Huntington’s disease should be closely monitored for mood changes, worsening depression, or suicidal thoughts.
Can valbenazine cause QT prolongation?
Yes. Valbenazine may prolong the QT interval, especially in CYP2D6 poor metabolizers or patients taking strong CYP2D6 or CYP3A4 inhibitors. It should be avoided in congenital long QT syndrome or arrhythmias associated with prolonged QT interval.
How is valbenazine different from tetrabenazine?
Both inhibit VMAT2, but valbenazine is newer and is given once daily. Tetrabenazine is older, has shorter action, often requires multiple daily dosing, and has important neuropsychiatric safety concerns.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

