
Table of Contents
Introduction
Everolimus is an oral mammalian target of rapamycin inhibitor, commonly called an mTOR inhibitor. It is used as an anticancer drug, immunosuppressant, and targeted therapy in selected genetic and proliferative disorders. It is marketed under different brand names depending on indication, such as Afinitor for oncology and tuberous sclerosis complex-related conditions, and Zortress for transplant rejection prophylaxis.
Everolimus is pharmacologically important because mTOR is a central intracellular kinase that regulates cell growth, protein synthesis, metabolism, angiogenesis, and immune cell proliferation. When the mTOR pathway becomes overactive, cells may show abnormal growth, survival, and proliferation. This is especially important in cancers, tuberous sclerosis complex, and transplant immunology.
Everolimus is used in several conditions, including advanced hormone receptor-positive, HER2-negative breast cancer in combination with exemestane, neuroendocrine tumors, advanced renal cell carcinoma after prior therapy, tuberous sclerosis complex-associated renal angiomyolipoma, tuberous sclerosis complex-associated subependymal giant cell astrocytoma, and selected seizure-related indications in tuberous sclerosis complex. Everolimus is also used as an immunosuppressant to prevent organ rejection in selected kidney and liver transplant patients. Current labeling lists these major oncology, TSC, and transplant-related uses.
For pharmacy, medical, nursing, and competitive exam students, everolimus is important because it connects cancer pharmacology, immunology, cell signaling, and transplant medicine. Its key mechanism is inhibition of mTOR complex 1 after binding to FKBP-12, leading to reduced protein synthesis, cell growth, angiogenesis, and immune cell proliferation.
Mechanism of Action (Step-wise)
- Primary target: mTOR pathway
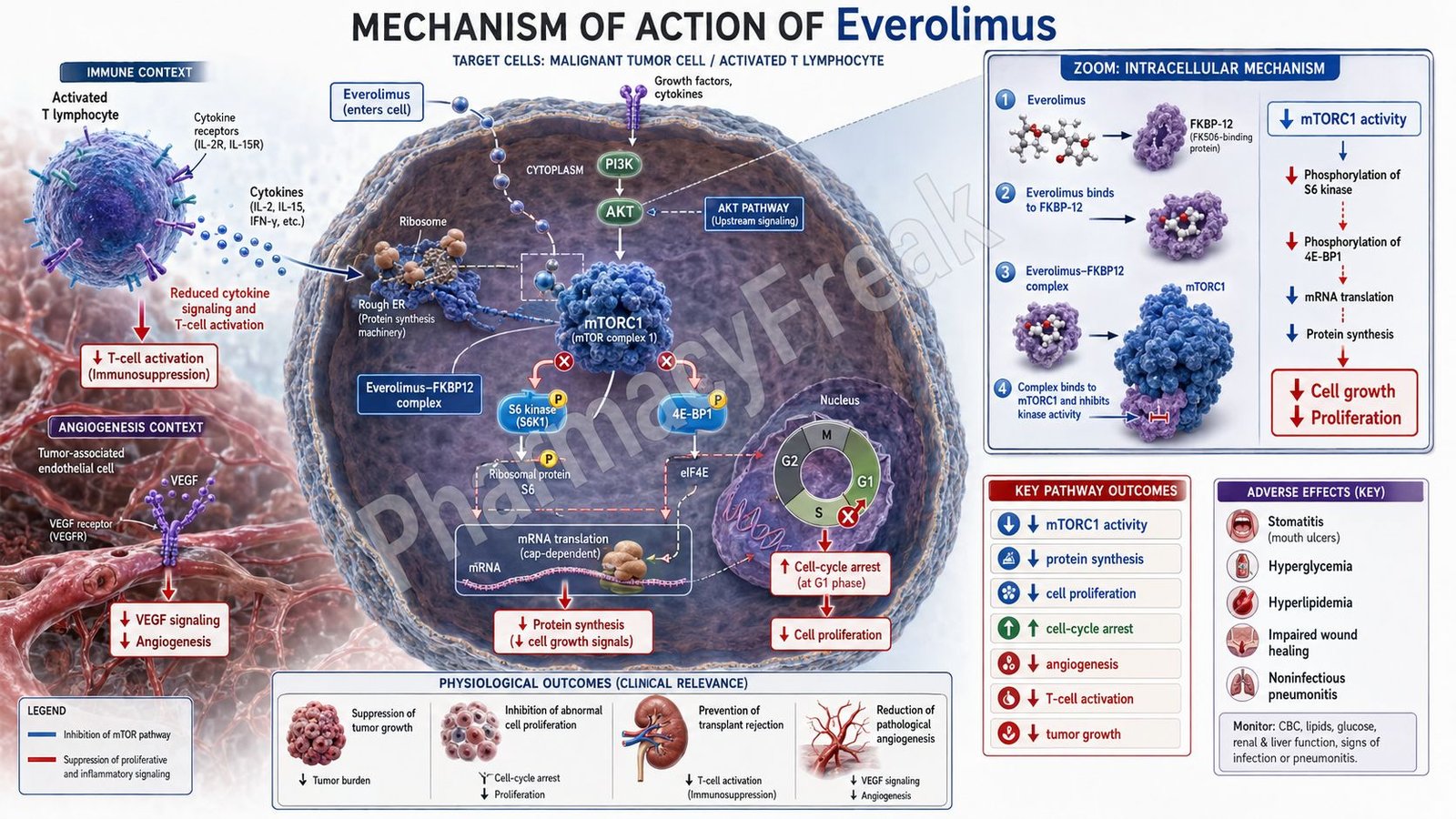
Everolimus targets the mammalian target of rapamycin pathway. mTOR is a serine-threonine kinase that exists mainly in two complexes: mTORC1 and mTORC2. Everolimus primarily inhibits mTORC1.
mTORC1 is involved in regulation of protein synthesis, cell growth, cell-cycle progression, angiogenesis, nutrient sensing, and metabolism.
- Binding to FKBP-12
Everolimus does not directly block mTOR alone. First, it binds to an intracellular protein called FKBP-12, also known as FK506-binding protein-12.
The everolimus-FKBP-12 complex then interacts with mTORC1 and inhibits its signaling activity. This is similar to the mechanism of sirolimus, but everolimus has different pharmacokinetic properties.
- Inhibition of mTORC1 signaling
After forming the everolimus-FKBP-12 complex, mTORC1 activity is inhibited. This suppresses downstream phosphorylation of important signaling proteins such as p70 S6 kinase and 4E-BP1.
These proteins normally promote translation of mRNAs required for cell growth, protein synthesis, and proliferation.
- Reduced protein synthesis and cell growth
By inhibiting p70 S6 kinase and 4E-BP1 signaling, everolimus decreases synthesis of proteins needed for cell-cycle progression and cellular growth.
This reduces the ability of tumor cells and abnormal proliferating cells to grow and divide.
- Cell-cycle arrest
Everolimus can cause arrest of cells in the G1 phase of the cell cycle. This prevents progression into the S phase, where DNA replication occurs.
This cell-cycle effect is important in cancers and proliferative disorders where cells are dividing abnormally.
- Reduced angiogenesis
mTOR signaling promotes production of pro-angiogenic factors such as vascular endothelial growth factor. By inhibiting mTORC1, everolimus can reduce angiogenic signaling.
This limits the formation of new blood vessels that support tumor growth and survival.
- Effect in cancer
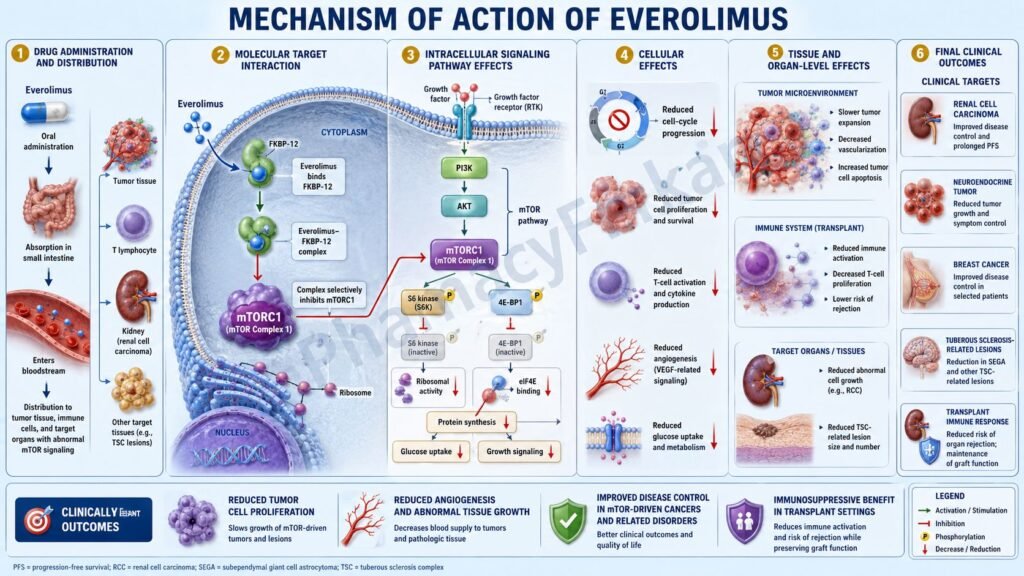
In cancer cells, abnormal PI3K/AKT/mTOR pathway activation promotes growth, survival, metabolism, and resistance to apoptosis. Everolimus suppresses this pathway downstream at mTORC1.
The final anticancer effect is reduced tumor cell proliferation, reduced angiogenesis, and slower disease progression in selected cancers.
- Effect in tuberous sclerosis complex
In tuberous sclerosis complex, mutations in TSC1 or TSC2 lead to increased mTOR pathway activation. This causes abnormal cell growth and tumor-like lesions such as renal angiomyolipoma and subependymal giant cell astrocytoma.
Everolimus inhibits the overactive mTOR pathway and helps reduce abnormal growth in selected TSC-related conditions.
- Effect in transplantation
In transplant medicine, everolimus inhibits cytokine-driven T-cell proliferation. After antigen stimulation, interleukin-2 normally promotes T-cell clonal expansion. Everolimus blocks downstream mTOR signaling required for this proliferation.
This reduces immune activation against the transplanted organ and helps prevent rejection when used with other immunosuppressants.
- Final therapeutic effect
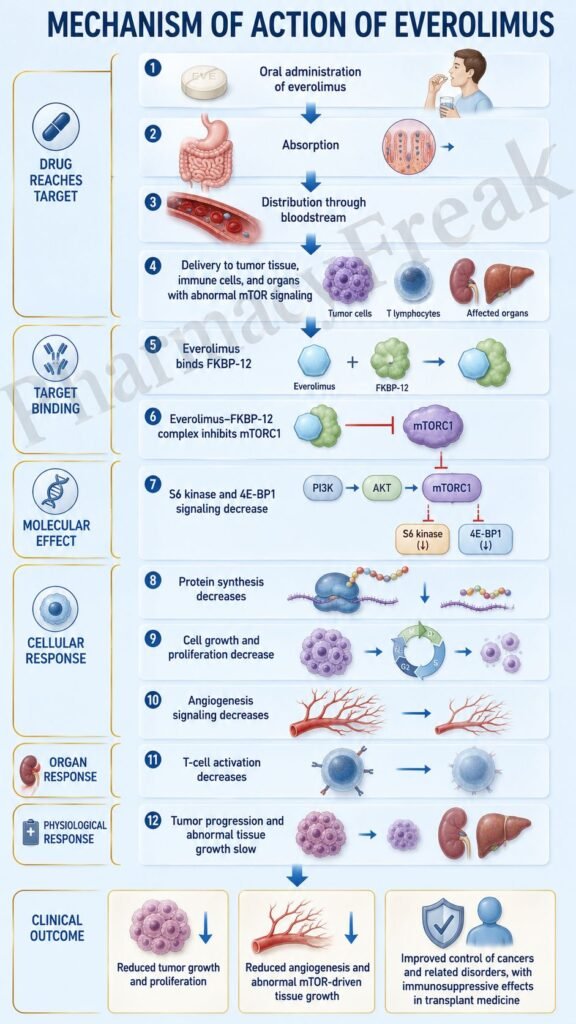
The final therapeutic effect of everolimus is inhibition of mTORC1-mediated signaling, reduced protein synthesis, reduced cell-cycle progression, decreased angiogenesis, suppression of abnormal cell growth, and inhibition of immune cell proliferation.
Pharmacokinetics
Everolimus is administered orally as tablets or dispersible tablets, depending on the indication and formulation. It is usually taken once daily for oncology and tuberous sclerosis complex-related uses, while transplant regimens may use specific dosing schedules with therapeutic drug monitoring.
Absorption:
Everolimus is absorbed after oral administration. Food can affect drug exposure, so patients should take it consistently either with food or without food according to prescribed instructions. Consistency is important to maintain stable exposure.
Distribution:
Everolimus distributes into blood and tissues and is significantly bound to plasma proteins. Because it acts intracellularly, it must enter target cells and form a complex with FKBP-12 to inhibit mTORC1.
Metabolism:
Everolimus is extensively metabolized in the liver and intestinal wall, mainly by CYP3A4. It is also a substrate of P-glycoprotein. This makes drug interactions clinically important.
Strong CYP3A4 or P-glycoprotein inhibitors can increase everolimus exposure and toxicity. Strong CYP3A4 inducers can reduce exposure and decrease effectiveness.
Excretion:
Everolimus and its metabolites are eliminated mainly through feces, with a smaller amount eliminated through urine. Unchanged drug is not the major form eliminated.
Half-life and duration:
Everolimus has a relatively long elimination half-life of approximately 30 hours, which supports once-daily dosing in many non-transplant indications.
Special pharmacokinetic point:
In transplant patients, therapeutic drug monitoring is important because too little drug may increase rejection risk, while excessive exposure may increase infection, toxicity, nephrotoxicity, and other adverse effects. Zortress labeling specifically recommends therapeutic drug monitoring when everolimus is used with cyclosporine or tacrolimus-based transplant regimens.
Clinical Uses
- Advanced hormone receptor-positive, HER2-negative breast cancer:
Everolimus is used with exemestane in postmenopausal women with advanced HR-positive, HER2-negative breast cancer after failure of letrozole or anastrozole. - Neuroendocrine tumors:
Everolimus is used in selected adult patients with progressive neuroendocrine tumors of pancreatic origin and well-differentiated, non-functional neuroendocrine tumors of gastrointestinal or lung origin. - Advanced renal cell carcinoma:
Everolimus is used in adult patients with advanced renal cell carcinoma after failure of treatment with sunitinib or sorafenib. - Tuberous sclerosis complex-associated renal angiomyolipoma:
It is used in adult patients with renal angiomyolipoma associated with tuberous sclerosis complex who do not require immediate surgery. - Tuberous sclerosis complex-associated brain lesions:
Everolimus is used in selected patients with subependymal giant cell astrocytoma associated with tuberous sclerosis complex. - Tuberous sclerosis complex-associated seizures:
Everolimus dispersible tablets may be used as adjunctive therapy for certain partial-onset seizures associated with tuberous sclerosis complex. - Prevention of organ rejection:
Everolimus is used as an immunosuppressant to prevent kidney and liver transplant rejection in selected adult patients, usually with reduced-dose calcineurin inhibitors and corticosteroids.
Adverse Effects
Common adverse effects of everolimus include:
- Stomatitis
- Mouth ulcers
- Rash
- Fatigue
- Diarrhea
- Nausea
- Vomiting
- Decreased appetite
- Weight loss
- Infections
- Cough
- Headache
- Edema
- Hyperglycemia
- Hyperlipidemia
- Anemia
- Thrombocytopenia
- Neutropenia
- Increased liver enzymes
Important serious adverse effects include:
- Non-infectious pneumonitis
- Serious infections
- Stomatitis and severe oral ulceration
- Renal failure or worsening renal function
- Hyperglycemia
- Hyperlipidemia
- Myelosuppression
- Delayed wound healing
- Severe hypersensitivity reactions
- Angioedema, especially with ACE inhibitors
- Hepatitis B reactivation
- Embryo-fetal toxicity
- Increased risk of malignancy with chronic immunosuppression
- Kidney graft thrombosis in transplant settings
Stomatitis is one of the most common and exam-important adverse effects. It may require mouth care, topical therapy, dose interruption, or dose reduction.
Non-infectious pneumonitis is a serious adverse effect of mTOR inhibitors. Patients may present with cough, dyspnea, hypoxia, or pulmonary infiltrates.
Everolimus can suppress immune function, increasing the risk of bacterial, viral, fungal, and opportunistic infections. Transplant labeling also carries major warnings for malignancies, serious infections, kidney graft thrombosis, nephrotoxicity, and mortality in heart transplantation.
Comparative Analysis
| Feature | Everolimus | Sirolimus | Temsirolimus | Alpelisib |
|---|---|---|---|---|
| Drug class | mTOR inhibitor | mTOR inhibitor | mTOR inhibitor | PI3K alpha inhibitor |
| Main target | mTORC1 through FKBP-12 | mTORC1 through FKBP-12 | mTOR pathway | PI3K alpha |
| Main pathway | PI3K/AKT/mTOR pathway | PI3K/AKT/mTOR pathway | PI3K/AKT/mTOR pathway | PI3K/AKT/mTOR pathway upstream |
| Main uses | Cancer, TSC, transplant rejection prophylaxis | Transplant, lymphangioleiomyomatosis | Renal cell carcinoma | PIK3CA-mutated breast cancer, PROS |
| Route | Oral | Oral | Intravenous | Oral |
| Important adverse effects | Stomatitis, infections, pneumonitis, hyperglycemia, hyperlipidemia | Hyperlipidemia, infections, wound healing delay | Rash, hyperglycemia, pneumonitis | Hyperglycemia, rash, diarrhea |
| Immunosuppressive role | Yes | Yes | Limited compared with sirolimus/everolimus | No routine transplant role |
| Angiogenesis effect | Reduces VEGF-related signaling | Reduces proliferative signaling | Antitumor mTOR inhibition | Indirect pathway effect |
Everolimus and sirolimus both inhibit mTORC1 after binding FKBP-12, but everolimus has different pharmacokinetic properties and broader oncology-related indications. Temsirolimus is another mTOR inhibitor but is given intravenously and is mainly used in renal cell carcinoma. Alpelisib works upstream of mTOR by inhibiting PI3K alpha, while everolimus works downstream at mTORC1.
MCQs
- Everolimus belongs to which drug class?
a) mTOR inhibitor
b) Beta-blocker
c) Alkylating agent
d) Antihistamine
Answer: a) mTOR inhibitor
- Everolimus primarily inhibits which mTOR complex?
a) mTORC1
b) mTORC2 only
c) Proteasome complex
d) Cyclooxygenase complex
Answer: a) mTORC1
- Before inhibiting mTORC1, everolimus binds to:
a) FKBP-12
b) HER2 receptor
c) CD20
d) EGFR
Answer: a) FKBP-12
- The mTOR pathway is important for:
a) Cell growth, protein synthesis, and proliferation
b) Gastric acid neutralization only
c) Bacterial cell wall synthesis
d) Sodium channel opening only
Answer: a) Cell growth, protein synthesis, and proliferation
- Everolimus reduces phosphorylation of downstream proteins such as:
a) p70 S6 kinase and 4E-BP1
b) Hemoglobin and albumin
c) Troponin and myosin only
d) Insulin and glucagon
Answer: a) p70 S6 kinase and 4E-BP1
- Everolimus can cause arrest mainly in which phase of the cell cycle?
a) G1 phase
b) M phase
c) G2 phase only
d) Cytokinesis only
Answer: a) G1 phase
- Everolimus is used with exemestane in which cancer?
a) HR-positive, HER2-negative advanced breast cancer
b) Acute leukemia only
c) Prostate infection
d) Hodgkin lymphoma only
Answer: a) HR-positive, HER2-negative advanced breast cancer
- Everolimus is useful in tuberous sclerosis complex because TSC mutations cause:
a) Increased mTOR pathway activation
b) Complete absence of insulin receptors
c) Bacterial toxin production
d) Increased acetylcholine release
Answer: a) Increased mTOR pathway activation
- Which adverse effect is very common and exam-important with everolimus?
a) Stomatitis
b) Ototoxicity
c) Gingival hyperplasia
d) Severe bradycardia
Answer: a) Stomatitis
- Which pulmonary toxicity is associated with everolimus?
a) Non-infectious pneumonitis
b) Acute pulmonary embolism only
c) Asthma cure
d) Bronchodilation
Answer: a) Non-infectious pneumonitis
- Everolimus is mainly metabolized by:
a) CYP3A4
b) CYP2D6
c) Acetylcholinesterase
d) Monoamine oxidase-B
Answer: a) CYP3A4
- Everolimus is also a substrate of:
a) P-glycoprotein
b) Hemoglobin
c) Albumin receptor only
d) Insulin transporter
Answer: a) P-glycoprotein
- In transplant patients, everolimus helps prevent rejection by:
a) Inhibiting cytokine-driven T-cell proliferation
b) Increasing antibody formation
c) Stimulating T-cell clonal expansion
d) Directly killing bacteria
Answer: a) Inhibiting cytokine-driven T-cell proliferation
- Which metabolic adverse effect may occur with everolimus?
a) Hyperglycemia and hyperlipidemia
b) Severe hypocalcemia only
c) Complete absence of cholesterol
d) Acute insulin overdose
Answer: a) Hyperglycemia and hyperlipidemia
- Which statement about everolimus is correct?
a) It forms a complex with FKBP-12 and inhibits mTORC1 signaling
b) It blocks bacterial ribosomes
c) It is a direct insulin analog
d) It is a rescue bronchodilator
Answer: a) It forms a complex with FKBP-12 and inhibits mTORC1 signaling
FAQs
- What is everolimus used for?
Everolimus is used in selected cancers, tuberous sclerosis complex-related conditions, and transplant rejection prophylaxis. Its uses include advanced HR-positive, HER2-negative breast cancer with exemestane, neuroendocrine tumors, advanced renal cell carcinoma, TSC-associated renal angiomyolipoma, TSC-associated subependymal giant cell astrocytoma, and prevention of kidney or liver transplant rejection.
- What is the mechanism of action of everolimus?
Everolimus binds to FKBP-12 and forms a complex that inhibits mTORC1. This reduces downstream signaling through proteins such as p70 S6 kinase and 4E-BP1, leading to reduced protein synthesis, cell growth, proliferation, angiogenesis, and immune cell activation.
- Is everolimus chemotherapy?
Everolimus is not traditional cytotoxic chemotherapy. It is a targeted mTOR inhibitor that affects intracellular signaling pathways involved in cell growth and survival.
- Why is everolimus used in cancer?
Many cancers depend on abnormal PI3K/AKT/mTOR signaling for growth and survival. Everolimus inhibits mTORC1, reducing protein synthesis, cell-cycle progression, angiogenesis, and tumor proliferation.
- Why is everolimus used in tuberous sclerosis complex?
Tuberous sclerosis complex can involve overactivation of the mTOR pathway due to TSC1 or TSC2 mutations. Everolimus inhibits mTORC1 and helps control abnormal growth in selected TSC-related lesions.
- What are common side effects of everolimus?
Common side effects include stomatitis, mouth ulcers, rash, fatigue, diarrhea, nausea, infections, hyperglycemia, hyperlipidemia, anemia, and decreased appetite.
- What is the most important oral adverse effect of everolimus?
Stomatitis or mouth ulcers are very common and clinically important. Preventive oral care and early treatment are important during therapy.
- Can everolimus cause lung toxicity?
Yes. Everolimus can cause non-infectious pneumonitis, which may present with cough, breathlessness, hypoxia, or lung infiltrates.
- Which drugs interact with everolimus?
Strong CYP3A4 or P-glycoprotein inhibitors can increase everolimus levels, while strong CYP3A4 inducers can reduce levels. Drug interaction review is important before starting therapy.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

