
Table of Contents
Introduction
Upadacitinib is an oral Janus kinase inhibitor used in several immune-mediated inflammatory diseases. It is marketed under the brand name Rinvoq and is commonly classified as a selective JAK1 inhibitor, although it can affect other JAK enzymes at higher concentrations.
Upadacitinib is used in conditions such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondyloarthritis, atopic dermatitis, ulcerative colitis, Crohn’s disease, and selected pediatric inflammatory arthritis indications. Its role is especially important in patients who have an inadequate response or intolerance to conventional systemic therapy or biologic therapy, depending on the indication and local prescribing criteria. Current prescribing information describes Rinvoq/Rinvoq LQ as a JAK inhibitor with approved uses across multiple inflammatory diseases.
For pharmacy, medical, nursing, and competitive exam students, upadacitinib is important because it represents targeted oral immunomodulation. Unlike corticosteroids, which broadly suppress inflammation, upadacitinib blocks intracellular cytokine signaling through the JAK-STAT pathway. This reduces inflammatory gene transcription and helps control immune-mediated tissue damage.
The key pharmacological concept is inhibition of cytokine signaling, especially through JAK1-dependent pathways. Since many inflammatory cytokines use JAK enzymes to send signals into the cell, blocking this pathway reduces immune activation, inflammation, pain, swelling, skin lesions, and intestinal inflammation in suitable patients.
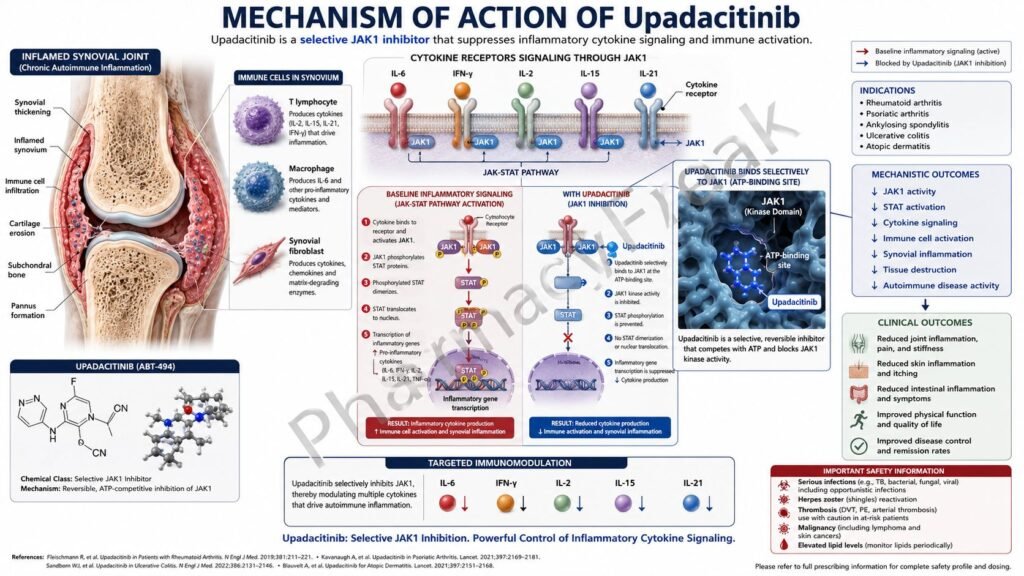
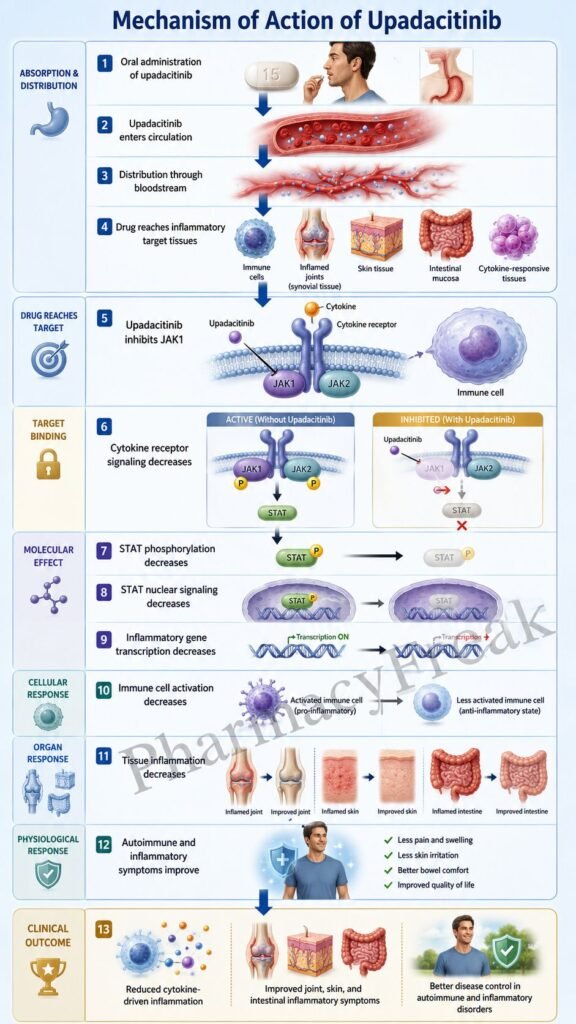
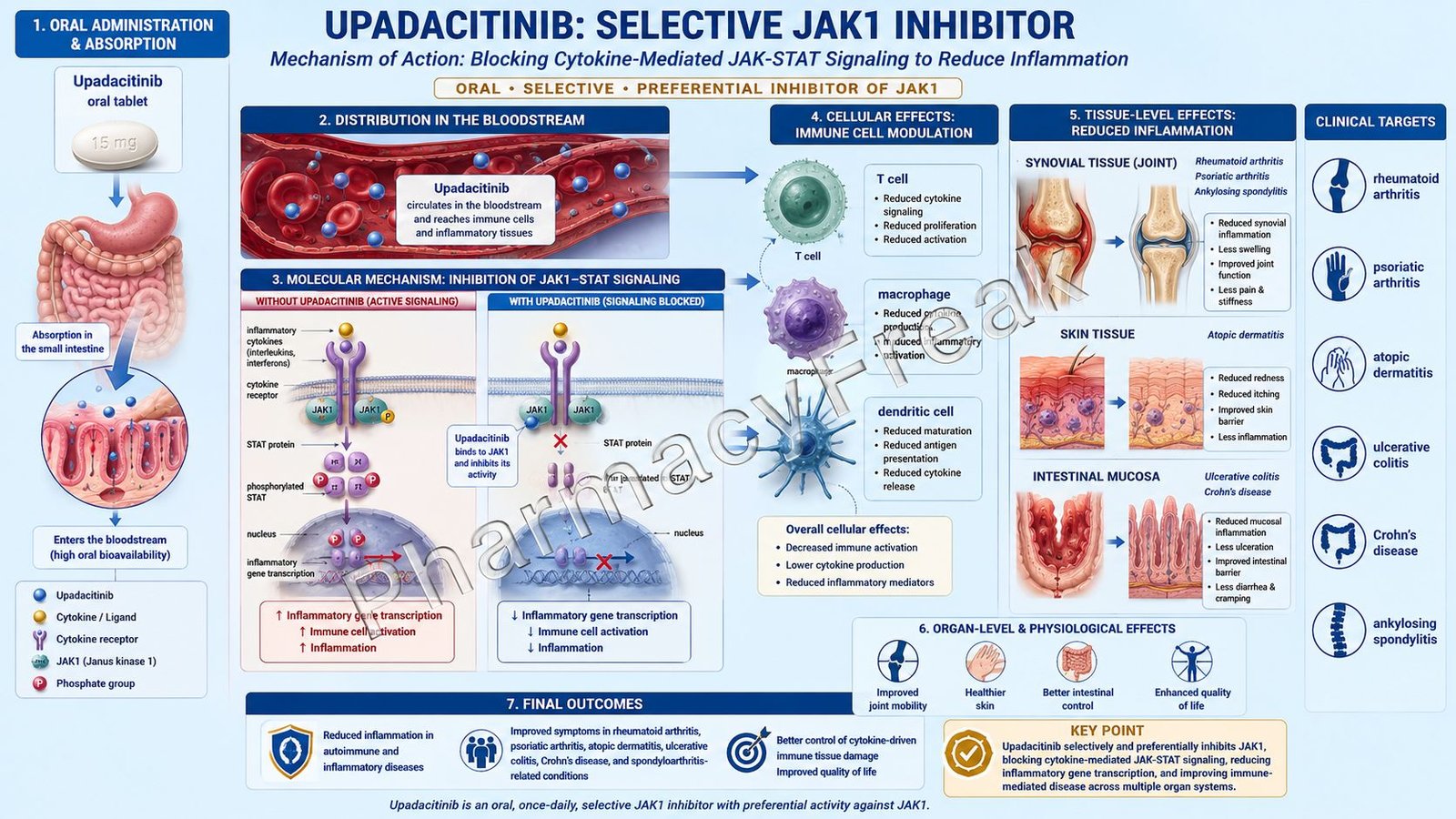
Mechanism of Action (Step-wise)
- Primary target: Janus kinase enzymes
Upadacitinib inhibits Janus kinase enzymes, especially JAK1. Janus kinases are intracellular tyrosine kinases associated with cytokine receptors.
There are four main JAK family members:
- JAK1
- JAK2
- JAK3
- TYK2
Upadacitinib shows greater inhibitory potency for JAK1 compared with JAK2, JAK3, and TYK2 in enzymatic and cellular assays, although the exact relationship between selective JAK inhibition and clinical effect is not fully established.
- Cytokines bind to cell-surface receptors
Inflammatory cytokines such as interleukins, interferons, and other immune mediators bind to receptors on immune cells and tissue cells. These receptors do not usually have intrinsic kinase activity. Instead, they depend on JAK enzymes attached to their intracellular portions.
When cytokines bind to their receptors, the associated JAK enzymes become activated.
- JAK activation normally phosphorylates STAT proteins
Activated JAK enzymes phosphorylate signal transducer and activator of transcription proteins, commonly called STAT proteins.
STAT proteins are important transcription factors. After phosphorylation, they dimerize and move into the nucleus, where they regulate inflammatory gene expression.
- Upadacitinib blocks JAK-mediated signaling
By inhibiting JAK enzymes, especially JAK1-related pathways, upadacitinib reduces phosphorylation and activation of STAT proteins.
This blocks the transmission of cytokine signals from the cell surface to the nucleus. The result is reduced expression of inflammatory genes, chemokines, adhesion molecules, and other immune mediators. Rinvoq’s mechanism is described as blocking JAK-STAT pathway signaling, thereby reducing pro-inflammatory processes.
- Reduced inflammatory cytokine activity
Many cytokines involved in autoimmune and inflammatory diseases signal through JAK pathways. By reducing JAK-STAT signaling, upadacitinib decreases immune cell activation, inflammatory cell recruitment, and tissue inflammation.
This is clinically useful in diseases such as rheumatoid arthritis, ulcerative colitis, Crohn’s disease, atopic dermatitis, and spondyloarthritis.
- Effect in rheumatoid arthritis and psoriatic arthritis
In rheumatoid arthritis and psoriatic arthritis, cytokine-driven inflammation causes synovitis, joint pain, swelling, stiffness, cartilage damage, and bone erosion.
Upadacitinib reduces cytokine signaling in immune cells and synovial tissue. This helps decrease joint inflammation, pain, morning stiffness, and disease activity.
- Effect in atopic dermatitis
In atopic dermatitis, cytokines involved in itch, skin inflammation, and barrier dysfunction activate JAK-dependent pathways.
By inhibiting these pathways, upadacitinib reduces inflammatory signaling in the skin, improving eczema lesions, pruritus, redness, and skin inflammation in suitable patients.
- Effect in inflammatory bowel disease
In ulcerative colitis and Crohn’s disease, dysregulated immune signaling causes chronic intestinal inflammation. Upadacitinib reduces inflammatory cytokine signaling in gut immune pathways, helping control mucosal inflammation, diarrhea, abdominal pain, and disease activity.
- Final therapeutic effect
The final therapeutic effect of upadacitinib is inhibition of JAK-STAT signaling, reduced inflammatory gene transcription, decreased cytokine-mediated immune activation, and clinical improvement in selected immune-mediated inflammatory diseases.
Pharmacokinetics
Upadacitinib is administered orally. It is available as extended-release tablets, and an oral solution formulation is also available for certain pediatric patients under Rinvoq LQ labeling.
Absorption:
Upadacitinib is absorbed after oral administration. The extended-release tablet is usually taken once daily, with or without food. Tablets should be swallowed whole and should not be split, crushed, or chewed.
Distribution:
Upadacitinib is moderately bound to plasma proteins. It distributes into tissues where it can inhibit intracellular JAK-mediated signaling in immune and inflammatory cells.
Metabolism:
Upadacitinib is metabolized mainly by CYP3A4, with a minor contribution from CYP2D6. This makes drug interactions clinically important. Strong CYP3A4 inhibitors may increase upadacitinib exposure, while strong CYP3A4 inducers may reduce exposure and decrease effectiveness.
Excretion:
Upadacitinib is eliminated through both fecal and urinary routes. A significant portion of the drug is eliminated as unchanged drug in feces and urine.
Half-life and duration:
The terminal half-life of upadacitinib is generally in the range of about 8 to 14 hours, supporting once-daily dosing for the extended-release formulation.
Special pharmacokinetic point:
Upadacitinib should generally be avoided in severe hepatic impairment. Drug interaction review is important before starting therapy, especially with strong CYP3A4 inhibitors, strong CYP3A4 inducers, and other immunosuppressive medicines.
Clinical Uses
- Rheumatoid arthritis:
Upadacitinib is used in adults with moderate to severe active rheumatoid arthritis, especially when response to other disease-modifying antirheumatic drugs is inadequate. - Psoriatic arthritis:
It is used in adults with active psoriatic arthritis to reduce joint inflammation, pain, stiffness, and disease activity. - Ankylosing spondylitis:
Upadacitinib is used in adults with active ankylosing spondylitis, where it helps reduce inflammatory back pain, stiffness, and axial inflammation. - Non-radiographic axial spondyloarthritis:
It is used in active non-radiographic axial spondyloarthritis with objective signs of inflammation. - Atopic dermatitis:
Upadacitinib is used in moderate to severe atopic dermatitis in suitable adults and adolescents when systemic therapy is appropriate. - Ulcerative colitis:
It is used in adults with moderately to severely active ulcerative colitis. - Crohn’s disease:
Upadacitinib is used in adults with moderately to severely active Crohn’s disease. - Pediatric inflammatory arthritis:
Certain pediatric formulations and indications include polyarticular juvenile idiopathic arthritis and related inflammatory arthritis settings depending on age, weight, and formulation. - Targeted oral alternative to injectable biologics:
Because upadacitinib is oral, it may be useful for patients who require targeted immune modulation but prefer oral therapy over injectable biologics.
Adverse Effects
Common adverse effects of upadacitinib include:
- Upper respiratory tract infection
- Nasopharyngitis
- Nausea
- Cough
- Fever
- Headache
- Acne
- Herpes simplex infection
- Herpes zoster infection
- Increased creatine phosphokinase
- Increased liver enzymes
- Increased lipid levels
- Neutropenia
- Lymphopenia
- Anemia
- Abdominal discomfort
- Fatigue
Important serious adverse effects include:
- Serious infections
- Tuberculosis
- Opportunistic infections
- Herpes zoster
- Malignancy
- Lymphoma
- Non-melanoma skin cancer
- Major adverse cardiovascular events
- Thrombosis
- Pulmonary embolism
- Deep vein thrombosis
- Gastrointestinal perforation
- Hepatotoxicity
- Severe hypersensitivity reactions
- Embryo-fetal toxicity
- Laboratory abnormalities such as neutropenia, lymphopenia, anemia, and lipid elevation
Upadacitinib carries boxed warnings related to serious infections, mortality, malignancy, major adverse cardiovascular events, and thrombosis. These warnings are important exam points for all JAK inhibitors used in chronic inflammatory diseases.
Patients should be evaluated for tuberculosis before starting therapy. Live vaccines should generally be avoided during treatment. Complete blood count, liver enzymes, and lipid profile should be monitored according to clinical guidelines.
Upadacitinib should be used carefully in patients with chronic or recurrent infections, history of tuberculosis, cardiovascular risk factors, history of malignancy, thrombotic risk factors, liver disease, or concurrent immunosuppressive therapy.
Comparative Analysis
| Feature | Upadacitinib | Tofacitinib | Baricitinib | Adalimumab |
|---|---|---|---|---|
| Brand example | Rinvoq | Xeljanz | Olumiant | Humira |
| Drug class | JAK inhibitor | JAK inhibitor | JAK inhibitor | TNF-alpha inhibitor |
| Main target | Preferential JAK1 inhibition | JAK1/JAK3 inhibition, with JAK2 activity | JAK1/JAK2 inhibition | TNF-alpha |
| Route | Oral | Oral | Oral | Subcutaneous injection |
| Main pathway | JAK-STAT cytokine signaling | JAK-STAT cytokine signaling | JAK-STAT cytokine signaling | TNF-alpha inflammatory pathway |
| Common uses | RA, PsA, AD, UC, CD, axial SpA | RA, PsA, UC, others | RA, alopecia areata, others | RA, PsA, IBD, psoriasis, AS |
| Major safety concern | Serious infection, MACE, thrombosis, malignancy | Serious infection, MACE, thrombosis, malignancy | Serious infection, thrombosis, lab abnormalities | Serious infection, TB reactivation |
| Monitoring | CBC, LFT, lipids, infection screening | CBC, LFT, lipids, infection screening | CBC, renal function, lipids | TB, hepatitis, infection monitoring |
Upadacitinib, tofacitinib, and baricitinib are oral JAK inhibitors, but they differ in JAK selectivity and approved indications. Adalimumab is different because it is a monoclonal antibody that neutralizes TNF-alpha rather than blocking intracellular JAK-STAT signaling. Upadacitinib is especially remembered as a JAK1-preferential inhibitor with broad use in inflammatory arthritis, atopic dermatitis, and inflammatory bowel disease.
MCQs
- Upadacitinib is marketed under which brand name?
a) Humira
b) Rinvoq
c) Xeljanz
d) Olumiant
Answer: b) Rinvoq
- Upadacitinib belongs to which drug class?
a) TNF-alpha inhibitor
b) JAK inhibitor
c) Calcineurin inhibitor
d) IL-17 inhibitor
Answer: b) JAK inhibitor
- Upadacitinib is commonly described as preferentially inhibiting:
a) JAK1
b) CD20
c) TNF-alpha
d) IL-5 receptor
Answer: a) JAK1
- The major intracellular pathway inhibited by upadacitinib is:
a) JAK-STAT pathway
b) COX-prostaglandin pathway
c) GABA chloride pathway
d) Cholinergic pathway
Answer: a) JAK-STAT pathway
- JAK activation normally leads to phosphorylation of:
a) STAT proteins
b) Hemoglobin
c) Albumin
d) Insulin only
Answer: a) STAT proteins
- Upadacitinib reduces inflammation by:
a) Blocking cytokine signaling
b) Directly killing bacteria
c) Increasing histamine release
d) Stimulating insulin secretion
Answer: a) Blocking cytokine signaling
- Which condition can be treated with upadacitinib?
a) Rheumatoid arthritis
b) Acute bacterial meningitis
c) Type 1 diabetes ketoacidosis
d) Malaria
Answer: a) Rheumatoid arthritis
- Upadacitinib is administered mainly by which route?
a) Oral
b) Intravenous
c) Intramuscular
d) Inhalational
Answer: a) Oral
- Which adverse effect is clinically important with upadacitinib?
a) Serious infection
b) Severe ototoxicity
c) Gingival hyperplasia
d) Hypocalcemia only
Answer: a) Serious infection
- Which viral infection may increase during upadacitinib therapy?
a) Herpes zoster
b) Rabies only
c) Measles only
d) Rotavirus only
Answer: a) Herpes zoster
- Which laboratory monitoring is important during upadacitinib therapy?
a) CBC, liver enzymes, and lipid profile
b) Blood group only
c) Serum calcium only
d) Visual acuity only
Answer: a) CBC, liver enzymes, and lipid profile
- Upadacitinib is mainly metabolized by:
a) CYP3A4
b) Acetylcholinesterase
c) Monoamine oxidase-B
d) Xanthine oxidase only
Answer: a) CYP3A4
- Which drug class should generally be avoided as live immunization during upadacitinib therapy?
a) Live vaccines
b) Oral iron
c) Antacids
d) Vitamin C
Answer: a) Live vaccines
- Upadacitinib differs from adalimumab because adalimumab targets:
a) TNF-alpha
b) JAK1
c) STAT proteins
d) CYP3A4
Answer: a) TNF-alpha
- Which statement about upadacitinib is correct?
a) It inhibits JAK-mediated cytokine signaling and reduces inflammatory gene transcription
b) It directly replaces insulin
c) It blocks bacterial cell wall synthesis
d) It acts as a rescue bronchodilator
Answer: a) It inhibits JAK-mediated cytokine signaling and reduces inflammatory gene transcription
FAQs
- What is upadacitinib used for?
Upadacitinib is used in several immune-mediated inflammatory diseases, including rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, non-radiographic axial spondyloarthritis, atopic dermatitis, ulcerative colitis, Crohn’s disease, and selected pediatric inflammatory arthritis indications.
- What is the mechanism of action of upadacitinib?
Upadacitinib inhibits Janus kinase enzymes, especially JAK1-related signaling. This reduces phosphorylation of STAT proteins, decreases inflammatory gene transcription, and suppresses cytokine-mediated immune activation.
- Is upadacitinib a biologic?
No. Upadacitinib is not a biologic monoclonal antibody. It is an oral small-molecule JAK inhibitor.
- Why is upadacitinib called a JAK1 inhibitor?
Upadacitinib shows greater inhibitory potency for JAK1 than for JAK2, JAK3, and TYK2 in laboratory assays. However, the exact clinical relationship between JAK selectivity, effectiveness, and safety is not completely established.
- How does upadacitinib reduce inflammation?
It blocks JAK-STAT signaling used by many inflammatory cytokines. This reduces immune cell activation, inflammatory mediator production, and tissue inflammation.
- What are common side effects of upadacitinib?
Common side effects include upper respiratory tract infection, nausea, cough, fever, acne, headache, herpes infections, increased liver enzymes, lipid changes, and blood count abnormalities.
- What are serious risks of upadacitinib?
Serious risks include serious infections, tuberculosis, opportunistic infections, malignancy, major adverse cardiovascular events, thrombosis, gastrointestinal perforation, liver abnormalities, and blood cell count suppression.
- Why is TB screening needed before upadacitinib?
Upadacitinib suppresses immune signaling, which can increase the risk of tuberculosis reactivation. Patients should be screened for latent or active TB before starting therapy.
- Can live vaccines be given with upadacitinib?
Live vaccines are generally avoided during upadacitinib therapy because immune suppression may increase infection risk from live vaccines.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

