
Table of Contents
Introduction
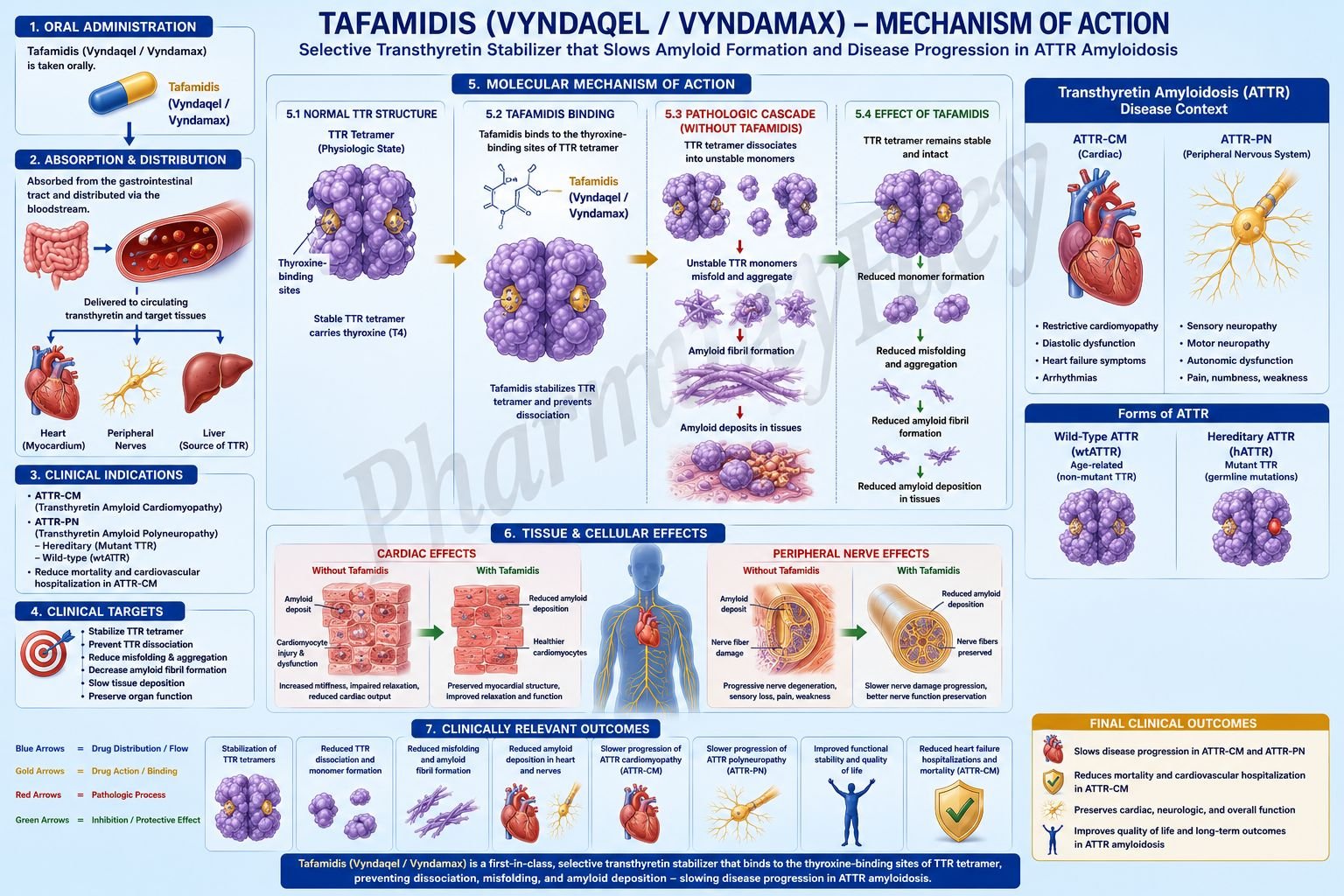
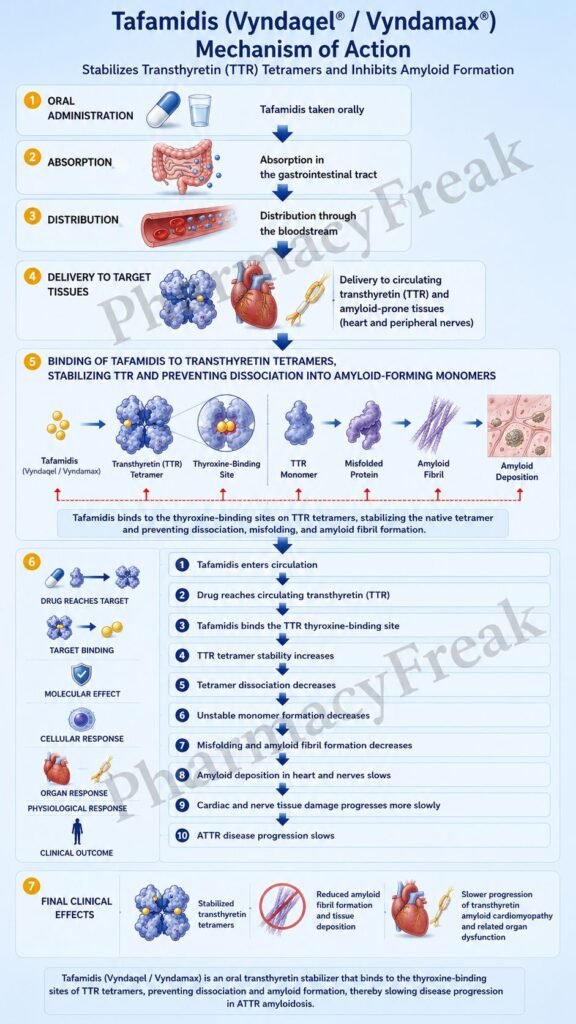
Tafamidis is an oral disease-modifying drug used for transthyretin amyloid cardiomyopathy, commonly abbreviated as ATTR-CM. It is marketed under the brand names Vyndaqel and Vyndamax. Pharmacologically, tafamidis is a transthyretin stabilizer.
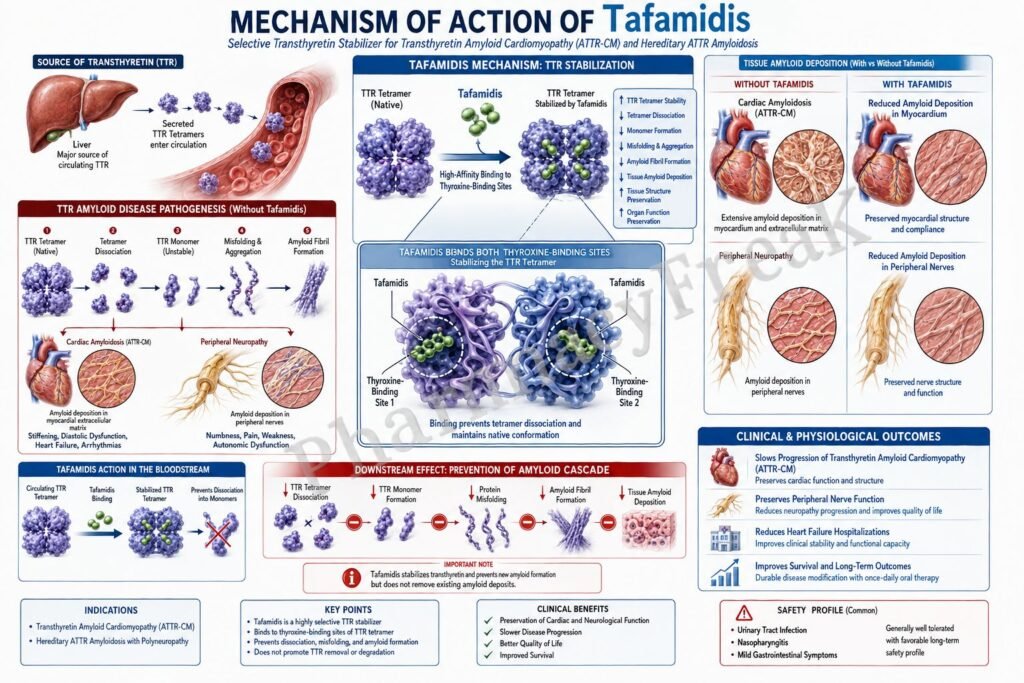
Transthyretin, or TTR, is a transport protein mainly produced by the liver. It normally circulates as a tetramer, meaning it is made of four protein subunits. TTR helps transport thyroxine and the retinol-binding protein–vitamin A complex. In transthyretin amyloidosis, the TTR tetramer becomes unstable, dissociates into monomers, misfolds, and forms amyloid fibrils that deposit in tissues.
In ATTR-CM, amyloid fibrils deposit in the myocardium. This makes the heart walls stiff, impairs ventricular filling, causes restrictive cardiomyopathy, and eventually leads to heart failure. ATTR-CM may be hereditary due to TTR gene variants or wild-type, which usually occurs with aging.
Tafamidis works by binding to transthyretin at its thyroxine-binding sites and stabilizing the TTR tetramer. By slowing tetramer dissociation, tafamidis reduces the rate-limiting step in amyloid formation. Vyndaqel and Vyndamax are indicated for adults with cardiomyopathy of wild-type or hereditary transthyretin-mediated amyloidosis to reduce cardiovascular mortality and cardiovascular-related hospitalization.
For exam purposes, tafamidis should be remembered as an oral TTR tetramer stabilizer used in ATTR-CM. It does not remove existing amyloid deposits rapidly, but it slows further amyloid formation and disease progression.
Mechanism of Action (Step-wise)
Step 1: Transthyretin normally circulates as a tetramer
TTR is a plasma protein that normally exists as a stable tetramer. It transports thyroxine and retinol-binding protein. In healthy physiology, this tetrameric structure remains sufficiently stable and does not usually form amyloid fibrils.
Step 2: TTR tetramer instability starts amyloid formation
In transthyretin amyloidosis, the TTR tetramer becomes unstable. This instability may be caused by inherited TTR gene mutations or age-related instability of wild-type TTR. The unstable tetramer separates into individual monomers.
Step 3: Tetramer dissociation is the rate-limiting step
The dissociation of the TTR tetramer into monomers is considered the rate-limiting step in the amyloidogenic process. Once monomers are released, they can misfold, aggregate, and form amyloid fibrils.
Step 4: Misfolded TTR forms amyloid fibrils
Misfolded TTR monomers aggregate into oligomers and amyloid fibrils. These fibrils are insoluble protein deposits that accumulate extracellularly in organs such as the heart and peripheral nerves.
Step 5: Amyloid deposits damage the myocardium
In ATTR-CM, amyloid fibrils deposit in the heart muscle. This causes thickened ventricular walls, increased stiffness, impaired diastolic filling, reduced cardiac reserve, conduction abnormalities, and progressive heart failure symptoms.
Step 6: Tafamidis binds to the thyroxine-binding sites of TTR
Tafamidis selectively binds to TTR at the thyroxine-binding sites. This binding stabilizes the tetrameric form of transthyretin and reduces its tendency to dissociate into monomers.
Step 7: TTR tetramer dissociation slows down
By stabilizing the tetramer, tafamidis slows the release of unstable monomers. This is the central pharmacological action of tafamidis because monomer formation is the key early event in amyloidogenesis.
Step 8: Misfolding and amyloid fibril formation decrease
When fewer TTR monomers are released, less misfolded TTR is available to form amyloid fibrils. Therefore, tafamidis slows further amyloid deposition in tissues.
Step 9: Cardiac amyloid progression slows
In ATTR-CM, slowing amyloid deposition helps preserve cardiac function over time. Tafamidis does not act as an inotrope, diuretic, vasodilator, or beta-blocker. Its benefit comes from stabilizing the disease-driving protein.
Step 10: Heart failure progression is reduced
By reducing ongoing TTR amyloid formation, tafamidis helps slow progression of ATTR-CM. Clinically, this translates into reduced cardiovascular mortality and reduced cardiovascular-related hospitalization in appropriate adult patients.
Step 11: Tafamidis stabilizes both wild-type and variant TTR
Tafamidis can stabilize wild-type TTR and several variant TTR tetramers. This explains its use in both wild-type ATTR-CM and hereditary ATTR-CM.
Step 12: Tafamidis may lower total thyroxine without clinical hypothyroidism
Because tafamidis binds to the TTR thyroxine-binding site, it may reduce serum total thyroxine concentrations. However, thyroid-stimulating hormone usually does not change, and clinical hypothyroidism has not been observed as a corresponding effect.
Pharmacokinetics
Tafamidis is administered orally as soft gelatin capsules. Vyndaqel contains tafamidis meglumine 20 mg capsules, while Vyndamax contains tafamidis free acid 61 mg capsules. These products contain the same active moiety but are not substitutable on a milligram-per-milligram basis.
The recommended adult dosage is either Vyndaqel 80 mg orally once daily, given as four 20 mg capsules, or Vyndamax 61 mg orally once daily, given as one capsule. The capsules should be swallowed whole and should not be crushed or cut.
Tafamidis may be taken with or without food. A high-fat, high-calorie meal does not produce clinically significant changes in tafamidis pharmacokinetics. Peak plasma concentrations occur within about 4 hours after dosing.
Tafamidis is highly protein bound, with more than 99% plasma protein binding in vitro. It primarily binds to transthyretin, which is also its pharmacological target. The mean half-life is approximately 49 hours, supporting once-daily dosing.
The metabolism of tafamidis has not been fully characterized, but glucuronidation has been observed. After a single oral dose of tafamidis meglumine, most recovery occurs in feces, largely as unchanged drug, while a smaller proportion is recovered in urine, mainly as a glucuronide metabolite.
Tafamidis is not mainly dependent on CYP metabolism. However, it inhibits breast cancer resistance protein, or BCRP. Therefore, it may increase exposure to BCRP substrates such as rosuvastatin, methotrexate, and imatinib, increasing the risk of substrate-related toxicity.
No clinically significant pharmacokinetic differences have been observed based on age, race or ethnicity, or renal impairment. The effect of severe hepatic impairment is unknown, so caution is appropriate in patients with significant liver disease.
Clinical Uses
Tafamidis is used for the treatment of transthyretin amyloid cardiomyopathy in adults. This includes both wild-type ATTR-CM and hereditary ATTR-CM.
The main therapeutic goal is to reduce cardiovascular mortality and cardiovascular-related hospitalization. Tafamidis is not used for immediate symptom relief like a diuretic. Instead, it is a disease-modifying therapy that slows the underlying amyloidogenic process.
Wild-type ATTR-CM usually occurs in older adults and is not caused by an inherited TTR mutation. It can present with heart failure with preserved ejection fraction, increased ventricular wall thickness, atrial fibrillation, conduction disease, carpal tunnel syndrome, or unexplained cardiomyopathy.
Hereditary ATTR-CM occurs due to pathogenic variants in the TTR gene. Depending on the mutation, patients may have predominantly cardiac features, neurologic features, or mixed disease.
Tafamidis is most useful when ATTR-CM is diagnosed before very advanced cardiac failure. Because it slows progression rather than reversing end-stage structural damage, early recognition of ATTR-CM is clinically important.
Tafamidis is not a general treatment for all heart failure. It is specifically used when transthyretin-mediated amyloid cardiomyopathy is confirmed or strongly established by appropriate diagnostic testing.
Adverse Effects
Tafamidis is generally well tolerated compared with many cardiovascular and oncology drugs. In the major placebo-controlled ATTR-CM clinical trial, adverse event frequency in tafamidis-treated patients was similar to placebo, and similar proportions of treated and placebo patients discontinued study drug because of adverse events.
The current label lists no contraindications for Vyndaqel or Vyndamax. However, absence of listed contraindications does not mean that the drug should be used without clinical judgment. Patient selection, diagnosis confirmation, pregnancy considerations, lactation counseling, and drug interaction review remain important.
Tafamidis may cause fetal harm based on animal data. Pregnant women should be advised about potential fetal risk, and pregnancy planning should be considered in females of reproductive potential.
Breastfeeding is not recommended during tafamidis treatment because animal data suggest transfer into milk and potential risk to the breastfed infant.
A clinically important drug interaction is with BCRP substrates. Tafamidis can increase exposure to drugs such as rosuvastatin, methotrexate, and imatinib. Patients taking such drugs should be monitored for substrate-related toxicity.
Tafamidis may reduce total thyroxine levels without increasing TSH and without clinical hypothyroidism. This is an important exam point because it reflects competition or displacement at transthyretin thyroxine-binding sites rather than primary thyroid gland failure.
At approximately 2.2 times the steady-state peak plasma concentration at the recommended dose, tafamidis does not prolong QTc to a clinically relevant extent. Therefore, QT prolongation is not a major defining toxicity of tafamidis.
Safety and effectiveness in pediatric patients have not been established. Tafamidis is used for adult ATTR-CM, not routine pediatric cardiomyopathy.
Comparative Analysis
Tafamidis is commonly compared with acoramidis, diflunisal, patisiran, vutrisiran, inotersen, eplontersen, and supportive heart failure therapies.
Tafamidis and acoramidis are both TTR stabilizers. Both act by stabilizing the TTR tetramer and reducing dissociation into monomers. Tafamidis is a well-established oral TTR stabilizer for ATTR-CM, while acoramidis is another oral TTR stabilizer developed for ATTR-CM.
Diflunisal is a nonsteroidal anti-inflammatory drug that can also stabilize TTR tetramers. However, it is not preferred in many cardiac amyloidosis patients because NSAIDs can worsen renal function, fluid retention, gastrointestinal bleeding risk, and heart failure.
Patisiran and vutrisiran are RNA interference therapies that reduce hepatic production of transthyretin. They work upstream by lowering TTR synthesis, while tafamidis works downstream by stabilizing circulating TTR tetramers.
Inotersen and eplontersen are antisense oligonucleotide therapies that also reduce TTR production. Like RNA interference drugs, they reduce the amount of TTR available to form amyloid, while tafamidis stabilizes existing circulating TTR.
Compared with conventional heart failure drugs such as diuretics, ACE inhibitors, ARBs, beta-blockers, mineralocorticoid receptor antagonists, or SGLT2 inhibitors, tafamidis directly targets the amyloid disease mechanism. Diuretics may relieve congestion, but they do not stabilize TTR or slow amyloid formation.
Compared with chemotherapy used for light-chain amyloidosis, tafamidis is not used to treat AL amyloidosis. AL amyloidosis is caused by abnormal immunoglobulin light chains from plasma cells and requires a different treatment approach. This distinction is very important in exams and clinical practice.
MCQs
- Tafamidis belongs to which pharmacological class?
a) Transthyretin stabilizer
b) Beta-blocker
c) ACE inhibitor
d) Proteasome inhibitor
Answer: a) Transthyretin stabilizer
- The brand names of tafamidis include:
a) Vyndaqel and Vyndamax
b) Entresto and Jardiance
c) Iclusig and Tasigna
d) Soliris and Ultomiris
Answer: a) Vyndaqel and Vyndamax
- Tafamidis is mainly used for:
a) Transthyretin amyloid cardiomyopathy in adults
b) Acute myocardial infarction thrombolysis
c) Bacterial endocarditis
d) Pulmonary tuberculosis
Answer: a) Transthyretin amyloid cardiomyopathy in adults
- Transthyretin normally circulates mainly as a:
a) Tetramer
b) Single DNA strand
c) Lipid bilayer
d) Hemoglobin dimer
Answer: a) Tetramer
- The rate-limiting step in TTR amyloid formation is:
a) Dissociation of TTR tetramer into monomers
b) Sodium channel opening
c) Platelet aggregation
d) Cyclooxygenase activation
Answer: a) Dissociation of TTR tetramer into monomers
- Tafamidis binds to TTR at which site?
a) Thyroxine-binding sites
b) ATP-binding kinase site
c) Dopamine-binding site
d) Opioid receptor site
Answer: a) Thyroxine-binding sites
- The main molecular effect of tafamidis is:
a) Stabilization of the TTR tetramer
b) Direct amyloid fibril digestion
c) Complete inhibition of TTR synthesis
d) Direct beta-1 receptor blockade
Answer: a) Stabilization of the TTR tetramer
- In ATTR-CM, amyloid fibrils mainly deposit in the:
a) Myocardium
b) Gastric lumen
c) Synovial fluid only
d) Bone marrow only
Answer: a) Myocardium
- Vyndaqel 80 mg daily is given as:
a) Four 20 mg tafamidis meglumine capsules
b) One 61 mg capsule
c) One intravenous infusion
d) Two subcutaneous injections
Answer: a) Four 20 mg tafamidis meglumine capsules
- Vyndamax contains:
a) Tafamidis 61 mg
b) Tafamidis meglumine 20 mg only
c) Eculizumab 300 mg
d) Patisiran 10 mg
Answer: a) Tafamidis 61 mg
- Which statement about Vyndaqel and Vyndamax is correct?
a) They are not substitutable on a per mg basis
b) They are identical milligram-for-milligram products
c) Vyndaqel is intravenous and Vyndamax is inhaled
d) Both are beta-blockers
Answer: a) They are not substitutable on a per mg basis
- Which transporter interaction is clinically important with tafamidis?
a) BCRP inhibition
b) Irreversible P-glycoprotein destruction
c) Sodium-glucose cotransporter activation
d) Dopamine transporter stimulation
Answer: a) BCRP inhibition
- Tafamidis may increase exposure to which BCRP substrate?
a) Rosuvastatin
b) Acetaminophen only
c) Salbutamol
d) Amoxicillin
Answer: a) Rosuvastatin
- Tafamidis may lower total thyroxine levels mainly because it:
a) Binds to TTR thyroxine-binding sites
b) Destroys the thyroid gland
c) Inhibits TSH release completely
d) Blocks iodine absorption permanently
Answer: a) Binds to TTR thyroxine-binding sites
- Which statement best differentiates tafamidis from patisiran?
a) Tafamidis stabilizes TTR tetramers, while patisiran reduces TTR production using RNA interference
b) Tafamidis is an antibiotic, while patisiran is an antifungal
c) Tafamidis directly blocks beta receptors, while patisiran blocks calcium channels
d) Both are NSAIDs used for pain relief only
Answer: a) Tafamidis stabilizes TTR tetramers, while patisiran reduces TTR production using RNA interference
FAQs
What is the mechanism of action of tafamidis?
Tafamidis binds to transthyretin at thyroxine-binding sites and stabilizes the TTR tetramer. This slows tetramer dissociation into monomers, reducing misfolding and amyloid fibril formation.
What is the brand name of tafamidis?
Tafamidis is marketed as Vyndaqel and Vyndamax.
What is tafamidis used for?
Tafamidis is used in adults with transthyretin amyloid cardiomyopathy, including wild-type and hereditary ATTR-CM, to reduce cardiovascular mortality and cardiovascular-related hospitalization.
Does tafamidis remove existing amyloid deposits?
Tafamidis does not rapidly remove existing amyloid deposits. Its main role is to stabilize TTR and slow further amyloid formation and disease progression.
How is Vyndaqel different from Vyndamax?
Vyndaqel contains tafamidis meglumine 20 mg capsules, usually taken as four capsules once daily. Vyndamax contains tafamidis 61 mg capsules, usually taken as one capsule once daily. They are not substitutable on a milligram-per-milligram basis.
Can tafamidis be used for all types of amyloidosis?
No. Tafamidis is used for transthyretin-mediated amyloid cardiomyopathy. It is not a treatment for light-chain amyloidosis, which has a different cause and requires different therapy.
What is the most important drug interaction with tafamidis?
Tafamidis inhibits BCRP and may increase exposure to BCRP substrates such as rosuvastatin, methotrexate, and imatinib. Monitoring for substrate-related toxicity may be needed.
Does tafamidis affect thyroid tests?
Tafamidis may reduce total thyroxine concentration because it binds strongly to the TTR thyroxine-binding site. However, TSH usually remains unchanged, and clinical hypothyroidism has not been observed as a corresponding effect.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

