
Table of Contents
Introduction
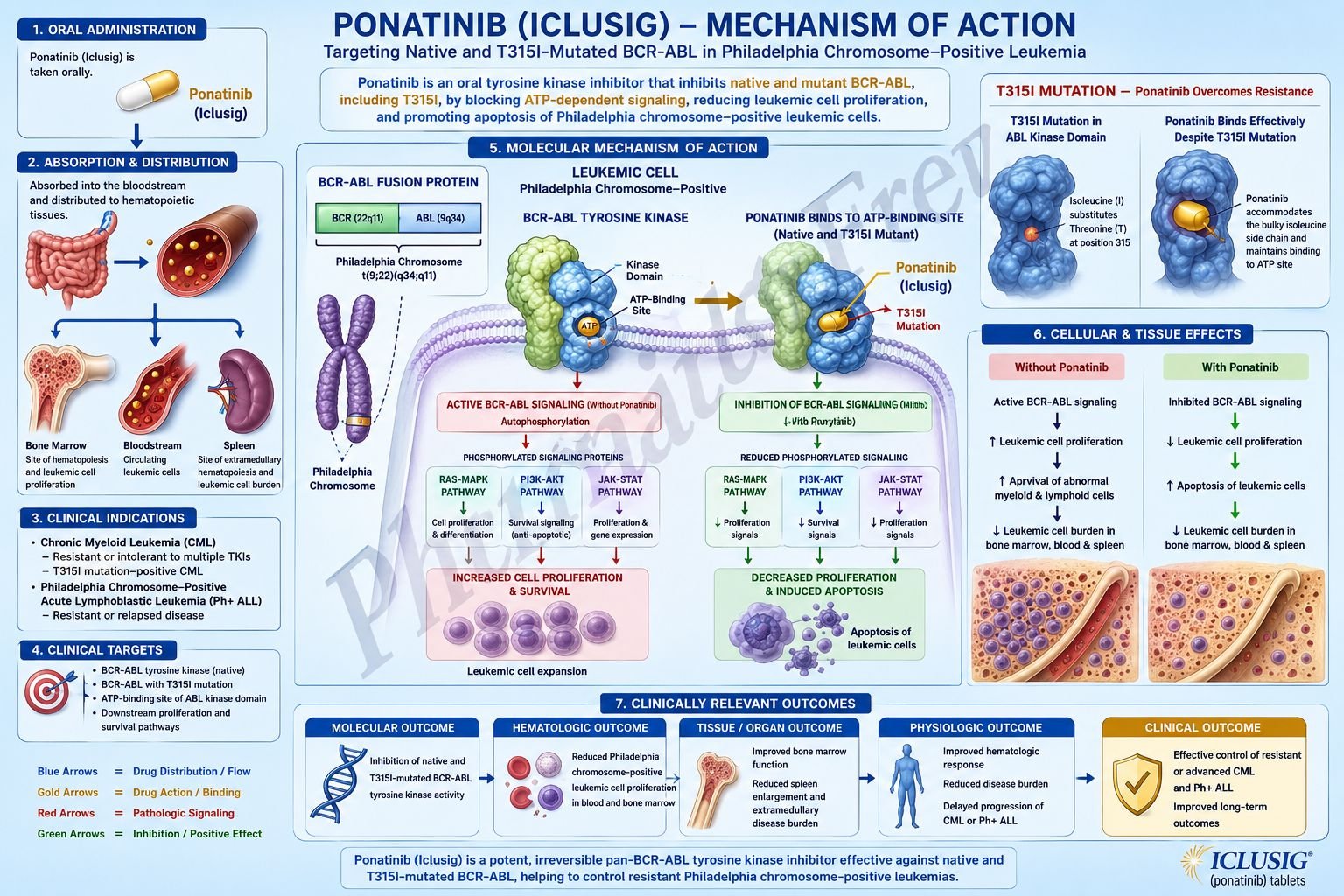
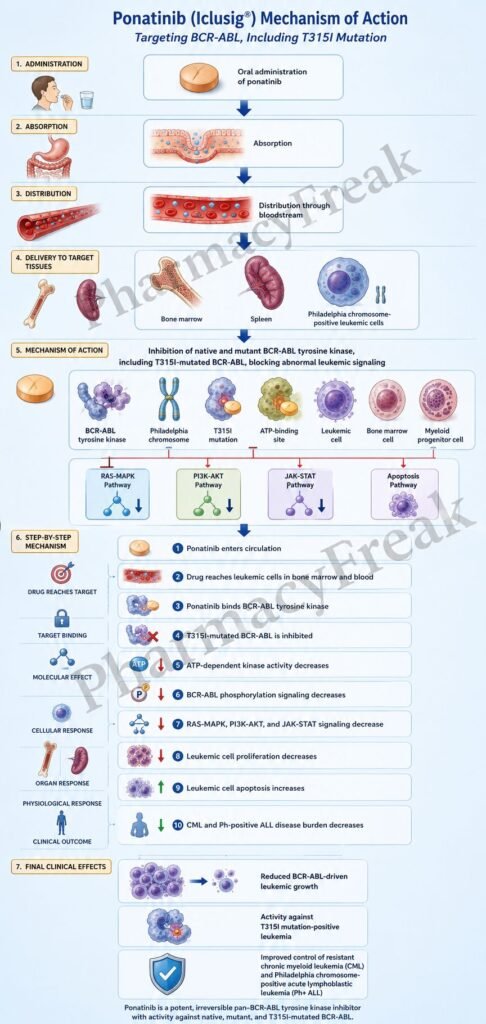
Ponatinib is an oral targeted anticancer drug used in selected Philadelphia chromosome-positive leukemias. It is marketed under the brand name Iclusig. Pharmacologically, ponatinib belongs to the BCR-ABL tyrosine kinase inhibitor class and is often described as a third-generation BCR-ABL inhibitor.
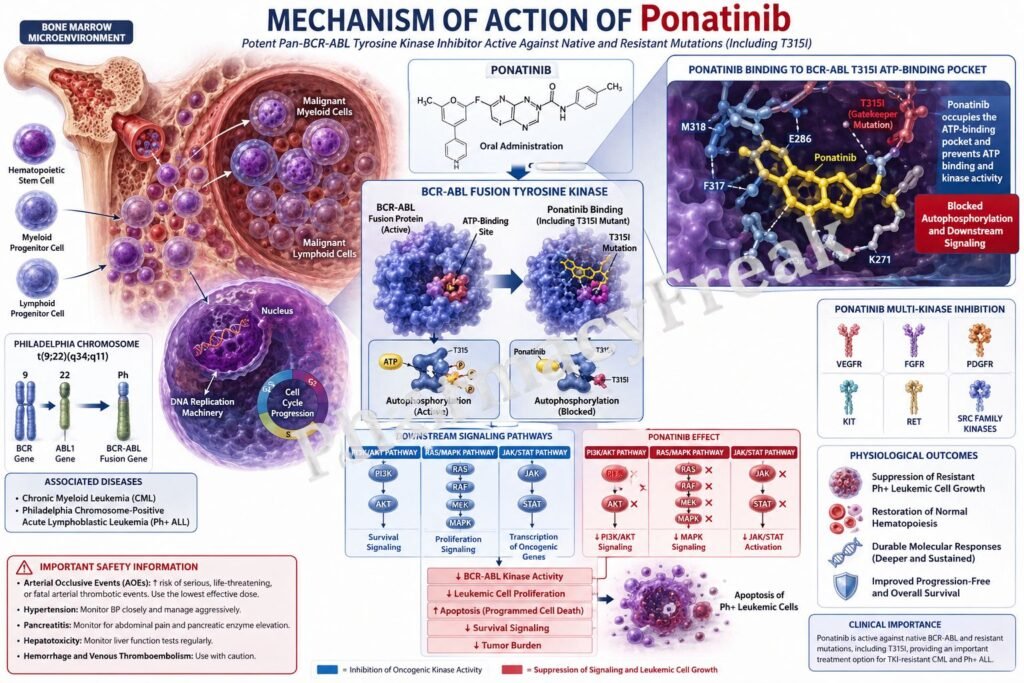
Philadelphia chromosome-positive chronic myeloid leukemia, or Ph+ CML, and Philadelphia chromosome-positive acute lymphoblastic leukemia, or Ph+ ALL, are driven by the abnormal BCR-ABL fusion kinase. This fusion kinase is produced by the t(9;22) chromosomal translocation, which forms the Philadelphia chromosome. The resulting BCR-ABL protein remains continuously active and stimulates uncontrolled cell growth, survival, and leukemic transformation.
Ponatinib is especially important because it inhibits native BCR-ABL and many mutant forms of BCR-ABL, including the T315I gatekeeper mutation. The T315I mutation causes resistance to several earlier BCR-ABL inhibitors such as imatinib, dasatinib, and nilotinib. Therefore, ponatinib has an important role in resistant or mutation-positive disease.
Current approved uses include selected adult patients with newly diagnosed Ph+ ALL in combination with chemotherapy, chronic phase CML with resistance or intolerance to at least two prior kinase inhibitors, accelerated or blast phase CML or Ph+ ALL when no other kinase inhibitors are indicated, and T315I-positive CML or Ph+ ALL. Ponatinib is not indicated and is not recommended for newly diagnosed chronic phase CML.
For exam purposes, ponatinib should be remembered as an oral third-generation BCR-ABL tyrosine kinase inhibitor active against T315I mutation, with major safety warnings for arterial occlusive events, venous thromboembolism, heart failure, and hepatotoxicity.
Mechanism of Action (Step-wise)
Step 1: Philadelphia chromosome creates BCR-ABL fusion kinase
In Ph+ CML and Ph+ ALL, a reciprocal translocation occurs between chromosomes 9 and 22. This creates the Philadelphia chromosome and forms the BCR-ABL fusion gene. The BCR-ABL gene produces an abnormal tyrosine kinase protein.
Step 2: BCR-ABL kinase becomes constitutively active
Normal ABL kinase activity is tightly regulated. In contrast, BCR-ABL remains continuously active without normal control. This means it keeps sending growth and survival signals even when the cell should not divide.
Step 3: Leukemic signaling pathways are activated
BCR-ABL activates several downstream pathways, including RAS/MAPK, PI3K/AKT, and JAK/STAT signaling. These pathways promote proliferation, reduce apoptosis, increase abnormal survival, and contribute to leukemic cell expansion.
Step 4: Earlier TKIs may fail due to resistance mutations
Some patients develop BCR-ABL mutations that reduce the binding of earlier tyrosine kinase inhibitors. The T315I mutation is especially important because it changes the ATP-binding region of BCR-ABL and blocks the activity of many older inhibitors.
Step 5: Ponatinib binds to the BCR-ABL kinase domain
Ponatinib binds to the kinase domain of BCR-ABL and inhibits its tyrosine kinase activity. It prevents the kinase from transferring phosphate groups from ATP to target proteins.
Step 6: Ponatinib inhibits native and mutant BCR-ABL
A key feature of ponatinib is activity against native BCR-ABL and multiple mutant forms, including T315I. This broad activity explains its role in resistant Ph+ leukemias where other BCR-ABL inhibitors may no longer work.
Step 7: BCR-ABL autophosphorylation decreases
BCR-ABL normally phosphorylates itself and downstream signaling proteins. Ponatinib reduces this phosphorylation. As phosphorylation decreases, leukemic signaling becomes weaker.
Step 8: Downstream survival signaling is suppressed
With BCR-ABL inhibited, downstream RAS/MAPK, PI3K/AKT, and JAK/STAT pathway activity decreases. This reduces uncontrolled leukemic cell growth and survival.
Step 9: Leukemic cell proliferation decreases
Ponatinib slows or stops the proliferation of Philadelphia chromosome-positive leukemic cells. This helps reduce leukemic burden in blood, bone marrow, and other involved tissues.
Step 10: Apoptosis of leukemic cells increases
By blocking the abnormal survival signals produced by BCR-ABL, ponatinib promotes programmed cell death, or apoptosis, in susceptible leukemic cells.
Step 11: Hematologic, cytogenetic, and molecular responses may occur
The clinical result may include normalization of blood counts, reduction of Philadelphia chromosome-positive cells, and reduction of BCR-ABL transcript levels. Molecular monitoring is especially important in CML management.
Step 12: Ponatinib also inhibits other kinases
Ponatinib is not limited only to BCR-ABL. It can also inhibit other kinases, including VEGFR, PDGFR, FGFR, SRC family kinases, KIT, RET, TIE2, and FLT3. However, the most important exam-relevant mechanism is inhibition of BCR-ABL, especially T315I-mutated BCR-ABL.
Pharmacokinetics
Ponatinib is administered orally as tablets and is generally taken once daily. It may be taken with or without food. The tablets should be swallowed whole and should not be crushed, broken, cut, or chewed.
After oral administration, ponatinib is absorbed systemically. It has a long enough effective duration to support once-daily dosing. Ponatinib is highly protein bound and distributes into tissues.
Ponatinib is metabolized mainly by CYP3A4, with minor contributions from other pathways. Strong CYP3A inhibitors can increase ponatinib exposure and may increase toxicity. Examples include clarithromycin, ketoconazole, itraconazole, ritonavir, and similar strong inhibitors. Strong CYP3A inducers can reduce ponatinib exposure and may reduce efficacy. Examples include rifampin, carbamazepine, phenytoin, and St. John’s wort.
Ponatinib is eliminated mainly through feces, with a smaller renal contribution. Because hepatic metabolism is important, liver function monitoring is clinically necessary. Hepatotoxicity is one of the major warnings associated with ponatinib.
Dose modification is commonly required based on indication, response, adverse effects, and vascular risk. In chronic phase CML, response-based dose reduction is used to reduce long-term toxicity after achieving an appropriate molecular response. This reflects the balance between maintaining efficacy and reducing vascular risk.
Clinical Uses
Ponatinib is used in selected adult patients with Philadelphia chromosome-positive leukemias. Its use is especially important when disease is resistant to prior tyrosine kinase inhibitors or when the T315I mutation is present.
In chronic phase CML, ponatinib is used in adults with resistance or intolerance to at least two prior kinase inhibitors. It is not a preferred drug for newly diagnosed chronic phase CML because of its serious vascular and hepatic safety risks.
In accelerated phase or blast phase CML, ponatinib is used when no other kinase inhibitors are indicated. These phases are more aggressive than chronic phase disease and require specialist-directed therapy.
In Ph+ ALL, ponatinib may be used in combination with chemotherapy for newly diagnosed adult patients under an accelerated approval pathway based on measurable residual disease-negative complete remission after induction. Continued approval for this indication may depend on confirmation of clinical benefit.
Ponatinib is also used as monotherapy in Ph+ ALL when no other kinase inhibitors are indicated, and in T315I-positive Ph+ ALL.
In T315I-positive CML, whether chronic phase, accelerated phase, or blast phase, ponatinib is important because it can inhibit the T315I-mutated BCR-ABL kinase that resists many earlier agents.
Adverse Effects
The most important adverse effects of ponatinib are vascular and cardiovascular toxicities. It carries major warnings for arterial occlusive events, venous thromboembolic events, heart failure, and hepatotoxicity. These toxicities can be serious, life-threatening, or fatal.
Arterial occlusive events may include myocardial infarction, stroke, peripheral arterial disease, and other arterial blockages. Patients with cardiovascular risk factors such as hypertension, diabetes, hyperlipidemia, smoking history, or prior vascular disease require careful risk assessment.
Venous thromboembolic events may include deep vein thrombosis, pulmonary embolism, retinal vein occlusion, or other venous clots. Patients should be educated to report sudden chest pain, shortness of breath, unilateral leg swelling, vision changes, or neurological symptoms.
Heart failure can occur during ponatinib therapy. Symptoms such as dyspnea, edema, rapid weight gain, fatigue, or reduced exercise tolerance require evaluation.
Hepatotoxicity is another major warning. Liver function tests should be checked before and during treatment. Severe liver injury, liver failure, and death have been reported.
Myelosuppression is common and clinically important. Ponatinib can cause thrombocytopenia, neutropenia, and anemia. Complete blood counts should be monitored regularly.
Pancreatitis and elevated lipase can occur. Abdominal pain, nausea, vomiting, and elevated pancreatic enzymes require evaluation and may require dose interruption or discontinuation.
Other adverse effects include hypertension, rash, dry skin, abdominal pain, headache, fatigue, pyrexia, arthralgia, myalgia, constipation, diarrhea, nausea, vomiting, fluid retention, neuropathy, hemorrhage, and infections.
Ponatinib can cause embryo-fetal toxicity. Females of reproductive potential should use effective contraception during treatment and for the recommended period after the last dose.
Comparative Analysis
Ponatinib is commonly compared with imatinib, dasatinib, nilotinib, bosutinib, and asciminib.
Imatinib is a first-generation BCR-ABL inhibitor. It transformed CML treatment but is not effective against many resistant mutations, especially T315I. Ponatinib is more potent against multiple resistant BCR-ABL mutations and is active against T315I.
Dasatinib is a second-generation BCR-ABL inhibitor that also inhibits SRC family kinases. It is useful in many imatinib-resistant cases but is not effective against T315I. Dasatinib is especially associated with pleural effusion and pulmonary arterial hypertension.
Nilotinib is another second-generation BCR-ABL inhibitor. It is more potent than imatinib against many forms of BCR-ABL but is also not effective against T315I. Nilotinib is strongly associated with QT prolongation, metabolic abnormalities, and arterial vascular events.
Bosutinib is a BCR-ABL and SRC inhibitor. It is used in resistant or intolerant Ph+ CML but does not have the same T315I activity as ponatinib. Diarrhea and liver enzyme elevation are important adverse effects.
Asciminib is different because it is a STAMP inhibitor that binds the ABL myristoyl pocket rather than the ATP-binding site. It is useful in some previously treated chronic phase CML cases and has an indication for T315I-positive chronic phase CML. However, ponatinib remains a classic exam answer for T315I-positive BCR-ABL inhibition.
Compared with traditional chemotherapy, ponatinib is targeted therapy because it blocks the abnormal kinase driving Ph+ leukemia. However, targeted therapy does not mean mild therapy. Ponatinib has serious vascular, cardiac, hepatic, pancreatic, and hematologic toxicities.
MCQs
- Ponatinib belongs to which pharmacological class?
a) BCR-ABL tyrosine kinase inhibitor
b) PARP inhibitor
c) Proteasome inhibitor
d) Alkylating agent
Answer: a) BCR-ABL tyrosine kinase inhibitor
- The brand name of ponatinib is:
a) Iclusig
b) Tasigna
c) Sprycel
d) Gleevec
Answer: a) Iclusig
- Ponatinib is especially important because it inhibits which resistant BCR-ABL mutation?
a) T315I
b) EGFR T790M
c) KRAS G12C
d) JAK2 V617F
Answer: a) T315I
- The Philadelphia chromosome results from which translocation?
a) t(9;22)
b) t(8;14)
c) t(15;17)
d) t(11;14)
Answer: a) t(9;22)
- BCR-ABL has which abnormal activity?
a) Constitutive tyrosine kinase activity
b) Cyclooxygenase inhibition
c) Dopamine receptor stimulation
d) Acetylcholinesterase activation
Answer: a) Constitutive tyrosine kinase activity
- Ponatinib inhibits leukemic cell growth mainly by:
a) Blocking BCR-ABL phosphorylation signaling
b) Activating bacterial cell wall breakdown
c) Increasing insulin secretion
d) Blocking histamine H1 receptors
Answer: a) Blocking BCR-ABL phosphorylation signaling
- Which downstream pathways are commonly activated by BCR-ABL?
a) RAS/MAPK, PI3K/AKT, and JAK/STAT
b) COX-1 and COX-2 only
c) GABA and glycine pathways
d) Renin and angiotensin only
Answer: a) RAS/MAPK, PI3K/AKT, and JAK/STAT
- Which disease is an important approved use of ponatinib?
a) T315I-positive chronic myeloid leukemia
b) Essential hypertension
c) Bacterial pneumonia
d) Type 1 diabetes mellitus
Answer: a) T315I-positive chronic myeloid leukemia
- Ponatinib is not indicated and not recommended for:
a) Newly diagnosed chronic phase CML
b) T315I-positive CML
c) Resistant Ph+ ALL
d) Resistant chronic phase CML after at least two TKIs
Answer: a) Newly diagnosed chronic phase CML
- Which serious adverse effect is strongly associated with ponatinib?
a) Arterial occlusive events
b) Gingival hyperplasia only
c) Irreversible hearing loss in all patients
d) Severe hypoglycemia
Answer: a) Arterial occlusive events
- Which hepatic safety concern is important with ponatinib?
a) Hepatotoxicity
b) Complete protection from liver injury
c) Mandatory gallstone dissolution
d) Increased bile production only
Answer: a) Hepatotoxicity
- Ponatinib is metabolized mainly by:
a) CYP3A4
b) CYP2C19 only
c) Monoamine oxidase
d) Acetylcholinesterase
Answer: a) CYP3A4
- Strong CYP3A inducers may:
a) Reduce ponatinib exposure and effectiveness
b) Increase ponatinib absorption permanently
c) Convert ponatinib into aspirin
d) Eliminate all toxicity risk
Answer: a) Reduce ponatinib exposure and effectiveness
- Which laboratory monitoring is important during ponatinib therapy?
a) Complete blood counts and liver function tests
b) Only serum sodium every 5 years
c) No monitoring is needed
d) Blood group testing only
Answer: a) Complete blood counts and liver function tests
- Which drug is a first-generation BCR-ABL inhibitor commonly compared with ponatinib?
a) Imatinib
b) Olaparib
c) Bevacizumab
d) Rituximab
Answer: a) Imatinib
FAQs
What is the mechanism of action of ponatinib?
Ponatinib inhibits BCR-ABL tyrosine kinase activity. It blocks phosphorylation signaling from native and mutant BCR-ABL, including T315I, thereby reducing leukemic cell proliferation and promoting apoptosis.
What is the brand name of ponatinib?
The brand name of ponatinib is Iclusig.
Why is ponatinib important in T315I mutation?
The T315I mutation causes resistance to several earlier BCR-ABL inhibitors. Ponatinib was designed to inhibit BCR-ABL even when this mutation is present, making it useful in selected resistant Ph+ leukemias.
Which cancers is ponatinib used for?
Ponatinib is used in selected adult patients with Ph+ CML and Ph+ ALL, especially resistant disease, T315I-positive disease, or settings where no other kinase inhibitors are indicated. It is also approved with chemotherapy for newly diagnosed adult Ph+ ALL under an accelerated approval pathway.
Is ponatinib used for newly diagnosed chronic phase CML?
No. Ponatinib is not indicated and is not recommended for newly diagnosed chronic phase CML because safer alternatives are generally preferred and ponatinib has serious vascular and hepatic risks.
What is the most important adverse effect of ponatinib?
The most important toxicities include arterial occlusive events, venous thromboembolic events, heart failure, and hepatotoxicity. These can be serious or fatal.
How is ponatinib different from imatinib?
Imatinib is a first-generation BCR-ABL inhibitor and does not inhibit the T315I mutation. Ponatinib is a third-generation BCR-ABL inhibitor active against T315I and many resistant mutations, but it has greater concern for vascular toxicity.
Can ponatinib cause pancreatitis?
Yes. Ponatinib can cause pancreatitis and elevated lipase. Abdominal pain, nausea, vomiting, or significant lipase elevation should be evaluated promptly.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

