
Table of Contents
Introduction
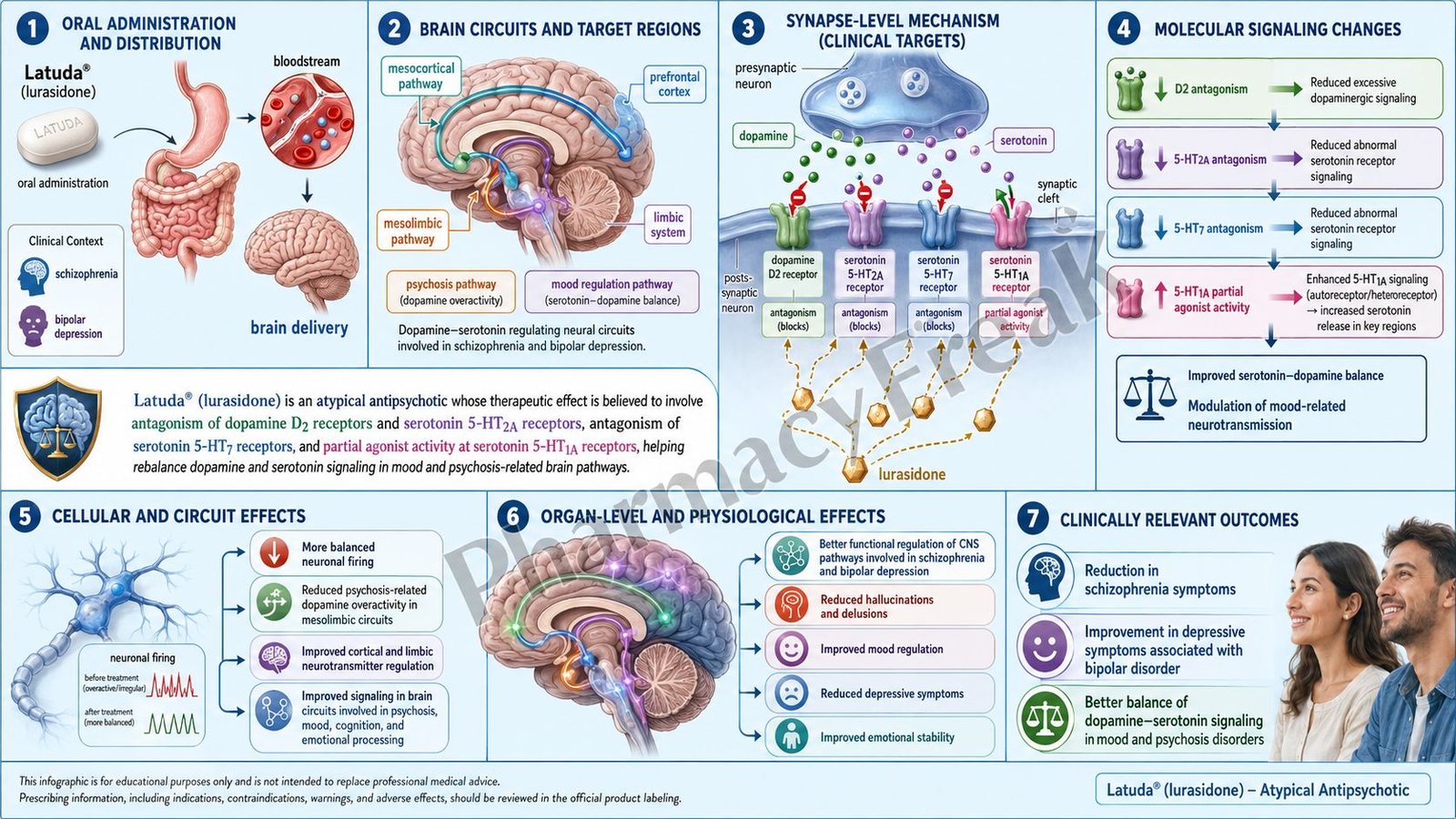
Latuda is the brand name of lurasidone hydrochloride, an oral atypical antipsychotic drug. It is mainly used for schizophrenia and depressive episodes associated with bipolar I disorder. Pharmacologically, lurasidone is classified as a second-generation antipsychotic, also called an atypical antipsychotic.
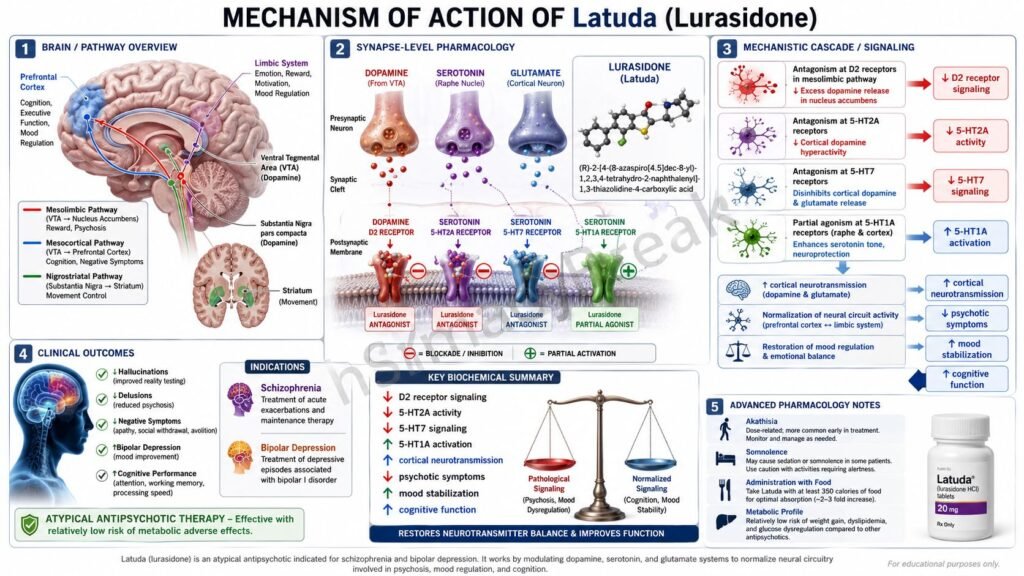
Lurasidone works by modulating dopamine and serotonin neurotransmission in the brain. The exact therapeutic mechanism in schizophrenia and bipolar depression is not fully established, but its clinical effects are believed to result mainly from dopamine D2 receptor antagonism and serotonin 5-HT2A receptor antagonism, with additional activity at serotonin 5-HT7 receptors and partial agonist activity at serotonin 5-HT1A receptors.
Schizophrenia is associated with abnormal dopaminergic signaling, especially excessive dopamine activity in the mesolimbic pathway, which contributes to positive symptoms such as hallucinations, delusions, and disorganized thinking. Bipolar depression involves complex dysregulation of dopamine, serotonin, glutamate, circadian rhythm, and mood-related neural networks.
For exam purposes, Latuda should be remembered as an atypical antipsychotic with D2 and 5-HT2A antagonism, important 5-HT7 antagonism, and 5-HT1A partial agonism. It has low affinity for histamine H1 and muscarinic M1 receptors, which helps explain its relatively lower tendency for sedation, anticholinergic effects, and weight gain compared with some other atypical antipsychotics.
Mechanism of Action (Step-wise)
Step 1: Dopamine dysregulation contributes to psychotic symptoms
In schizophrenia, excessive dopamine signaling in the mesolimbic pathway is strongly associated with positive psychotic symptoms. These symptoms include hallucinations, delusions, suspiciousness, and thought disorganization.
Step 2: Dopamine D2 receptors are activated excessively
Dopamine acts on D2 receptors in several brain regions. Excessive D2 receptor stimulation in the mesolimbic system contributes to psychosis. Blocking D2 receptors is a core mechanism shared by most effective antipsychotic drugs.
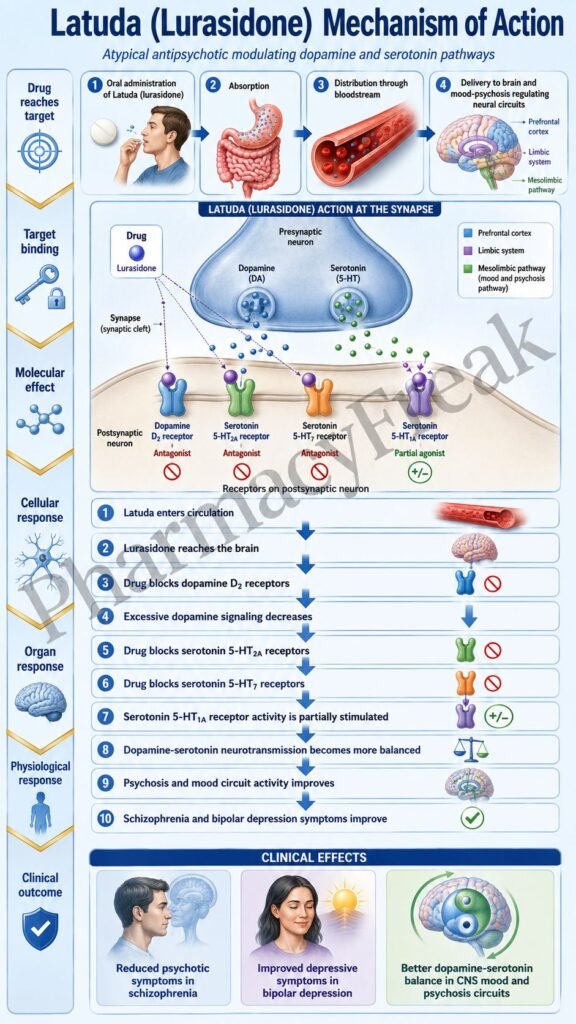
Step 3: Lurasidone blocks dopamine D2 receptors
Lurasidone acts as an antagonist at dopamine D2 receptors. By blocking D2 receptor signaling, it reduces excessive dopaminergic neurotransmission in psychosis-related pathways. This helps improve positive symptoms of schizophrenia.
Step 4: Serotonin 5-HT2A receptors influence dopamine pathways
Serotonin 5-HT2A receptors regulate dopamine release in different brain regions. Blocking 5-HT2A receptors can increase dopamine release in certain pathways, such as the nigrostriatal and mesocortical pathways.
Step 5: Lurasidone blocks serotonin 5-HT2A receptors
Lurasidone has antagonist activity at 5-HT2A receptors. This is one reason it is classified as an atypical antipsychotic. 5-HT2A antagonism may reduce the risk of extrapyramidal symptoms compared with strong D2 blockade alone and may help improve mood and cognitive-related symptoms.
Step 6: Balance between D2 and 5-HT2A effects produces atypical antipsychotic action
The combination of D2 antagonism and 5-HT2A antagonism helps reduce psychotic symptoms while limiting some motor adverse effects compared with older first-generation antipsychotics. However, extrapyramidal symptoms can still occur with lurasidone.
Step 7: 5-HT7 receptor antagonism may contribute to antidepressant effects
Lurasidone also has antagonist activity at serotonin 5-HT7 receptors. The 5-HT7 receptor is involved in mood regulation, cognition, circadian rhythm, and emotional processing. Blocking this receptor may contribute to the beneficial effects of lurasidone in bipolar depression.
Step 8: 5-HT1A partial agonism may support mood regulation
Lurasidone has partial agonist activity at serotonin 5-HT1A receptors. 5-HT1A receptor modulation is associated with anxiolytic and antidepressant-like effects in some pharmacological models. This may help explain its role in bipolar depression, although the full clinical mechanism is not completely established.
Step 9: Alpha-2C adrenergic antagonism may contribute to neurotransmitter modulation
Lurasidone also has antagonist activity at alpha-2C adrenergic receptors. This may influence norepinephrine and dopamine release in certain brain areas. The clinical importance of this effect is less central than D2 and serotonin receptor actions but may contribute to the overall pharmacological profile.
Step 10: Low H1 and M1 receptor affinity affects adverse effect profile
Lurasidone has low affinity for histamine H1 receptors and muscarinic M1 receptors. Therefore, it generally causes less antihistaminic sedation, anticholinergic dry mouth, constipation, urinary retention, blurred vision, and cognitive dulling than drugs with strong H1 or M1 blockade.
Step 11: Final therapeutic outcome in schizophrenia
In schizophrenia, lurasidone reduces positive symptoms mainly by D2 receptor blockade, while serotonin receptor modulation supports the atypical profile. It may also help with overall functioning, mood-related symptoms, and relapse control when taken consistently.
Step 12: Final therapeutic outcome in bipolar depression
In bipolar depression, lurasidone improves depressive symptoms through complex serotonin-dopamine modulation. Its 5-HT7 antagonism, 5-HT1A partial agonism, and D2/5-HT2A balance are considered important, although the exact antidepressant mechanism is not fully established.
Pharmacokinetics
Lurasidone is administered orally as film-coated tablets. It must be taken with food. A meal of at least 350 calories significantly increases absorption and helps achieve adequate drug exposure. Taking lurasidone without enough food can reduce absorption and may decrease clinical effectiveness.
After oral administration, lurasidone is absorbed and reaches peak plasma concentration in about 1 to 3 hours. It is highly protein bound, mainly to albumin and alpha-1-acid glycoprotein.
Lurasidone is metabolized mainly by CYP3A4. This is a very important exam point because strong CYP3A4 inhibitors and strong CYP3A4 inducers are contraindicated. Strong CYP3A4 inhibitors such as ketoconazole, clarithromycin, itraconazole, ritonavir, and some other protease inhibitors can greatly increase lurasidone exposure and toxicity. Strong CYP3A4 inducers such as rifampin, carbamazepine, phenytoin, and St. John’s wort can reduce lurasidone exposure and make treatment ineffective.
Moderate CYP3A4 inhibitors may require dose adjustment. Grapefruit and grapefruit juice are often avoided because they may increase drug exposure through CYP3A4 inhibition.
Lurasidone is eliminated mainly through feces, with a smaller amount eliminated in urine. Dose adjustment may be required in moderate to severe renal impairment and moderate to severe hepatic impairment.
The elimination half-life supports once-daily dosing. Because lurasidone is used for chronic psychiatric disorders, steady adherence is important. Abrupt discontinuation may lead to symptom recurrence or clinical worsening, so changes should be medically supervised.
Clinical Uses
Latuda is used for the treatment of schizophrenia in adults and adolescents aged 13 to 17 years. In schizophrenia, it helps reduce hallucinations, delusions, disorganized thinking, and other psychotic symptoms.
Latuda is also used for depressive episodes associated with bipolar I disorder. It may be used as monotherapy in adults and pediatric patients aged 10 to 17 years with bipolar depression.
In adults with bipolar depression, lurasidone may also be used as adjunctive therapy with lithium or valproate. This means it can be added when a mood stabilizer alone is not sufficient.
Lurasidone is not approved for the treatment of dementia-related psychosis. Like other antipsychotics, it carries a boxed warning for increased mortality in elderly patients with dementia-related psychosis.
It is also not a general sleep medicine, anxiety medicine, or antidepressant for all depressive disorders. Its approved psychiatric uses are specific and should be guided by diagnosis, age, patient risk factors, and clinical monitoring.
Adverse Effects
Common adverse effects of lurasidone include somnolence, akathisia, extrapyramidal symptoms, nausea, vomiting, restlessness, insomnia, and sedation. Akathisia is especially exam-relevant and presents as inner restlessness with an inability to sit still.
Extrapyramidal symptoms may include tremor, rigidity, bradykinesia, dystonia, and parkinsonism. These occur because D2 receptor blockade can affect the nigrostriatal dopamine pathway.
Tardive dyskinesia is a serious long-term risk with antipsychotic drugs. It presents as involuntary repetitive movements, often involving the face, lips, tongue, jaw, trunk, or limbs. The risk increases with longer duration and cumulative exposure.
Neuroleptic malignant syndrome is a rare but life-threatening adverse reaction. It may present with high fever, severe muscle rigidity, altered mental status, autonomic instability, elevated creatine kinase, and possible renal failure. It requires urgent discontinuation and emergency treatment.
Lurasidone can cause metabolic changes such as hyperglycemia, diabetes mellitus, dyslipidemia, and weight gain. However, compared with some atypical antipsychotics such as olanzapine and clozapine, lurasidone is generally considered to have a relatively lower metabolic burden.
Hyperprolactinemia may occur due to D2 receptor blockade in the tuberoinfundibular pathway. This may lead to galactorrhea, menstrual irregularities, sexual dysfunction, infertility, or gynecomastia.
Orthostatic hypotension and syncope may occur, especially during initiation or dose escalation. Falls can occur due to somnolence, postural hypotension, and motor instability.
Other important warnings include leukopenia, neutropenia, seizures, body temperature dysregulation, dysphagia, and possible cognitive or motor impairment. Patients should avoid driving or operating machinery until they know how the drug affects them.
Lurasidone carries a boxed warning for increased mortality in elderly patients with dementia-related psychosis and suicidal thoughts and behaviors in pediatric and young adult patients treated for bipolar depression.
Comparative Analysis
Lurasidone is commonly compared with other atypical antipsychotics such as risperidone, quetiapine, olanzapine, aripiprazole, ziprasidone, and cariprazine.
Compared with risperidone, lurasidone has lower tendency for prolactin elevation in many patients, although hyperprolactinemia can still occur. Risperidone has strong D2 and 5-HT2A antagonism and is more commonly associated with prolactin-related adverse effects.
Compared with quetiapine, lurasidone usually causes less sedation and less weight gain because it has low H1 receptor affinity. Quetiapine has strong antihistaminic activity and is more sedating, especially at lower doses.
Compared with olanzapine, lurasidone has a more favorable metabolic profile. Olanzapine is strongly associated with weight gain, increased appetite, hyperglycemia, and dyslipidemia. Lurasidone still requires metabolic monitoring, but metabolic effects are generally less prominent.
Compared with aripiprazole, lurasidone is a D2 antagonist, while aripiprazole is a partial D2 agonist. Aripiprazole is often associated with akathisia but tends to cause less prolactin elevation. Lurasidone also commonly causes akathisia and extrapyramidal symptoms.
Compared with ziprasidone, lurasidone has less emphasis on QT prolongation but still requires clinical judgment in patients with cardiac risk factors. Both should be taken with food for proper absorption, but ziprasidone generally requires a larger meal than lurasidone.
Compared with first-generation antipsychotics such as haloperidol and chlorpromazine, lurasidone has atypical serotonin-dopamine activity and generally lower risk of severe extrapyramidal symptoms than high-potency typical antipsychotics. However, movement disorders remain clinically important.
MCQs
- Latuda contains which active drug?
a) Quetiapine
b) Lurasidone
c) Risperidone
d) Olanzapine
Answer: b) Lurasidone
- Lurasidone belongs to which pharmacological class?
a) Atypical antipsychotic
b) Benzodiazepine
c) Mood stabilizer anticonvulsant
d) Tricyclic antidepressant
Answer: a) Atypical antipsychotic
- The main receptor action responsible for antipsychotic efficacy of lurasidone is:
a) Dopamine D2 receptor antagonism
b) Muscarinic M1 receptor activation
c) Beta-1 receptor blockade
d) NMDA receptor activation
Answer: a) Dopamine D2 receptor antagonism
- Lurasidone also blocks which serotonin receptor important for atypical antipsychotic action?
a) 5-HT2A receptor
b) 5-HT3 receptor only
c) 5-HT4 receptor only
d) 5-HT6 receptor only
Answer: a) 5-HT2A receptor
- Which receptor activity may contribute to the antidepressant effect of lurasidone in bipolar depression?
a) 5-HT7 antagonism
b) Nicotinic receptor activation
c) H2 receptor blockade only
d) GABA-A channel opening
Answer: a) 5-HT7 antagonism
- Lurasidone has partial agonist activity at which serotonin receptor?
a) 5-HT1A receptor
b) 5-HT2C receptor
c) 5-HT3 receptor
d) 5-HT6 receptor
Answer: a) 5-HT1A receptor
- Latuda should be taken:
a) With food of at least 350 calories
b) Only on an empty stomach
c) Only with grapefruit juice
d) By subcutaneous injection
Answer: a) With food of at least 350 calories
- Lurasidone is metabolized mainly by:
a) CYP3A4
b) CYP2C19 only
c) Monoamine oxidase
d) Acetylcholinesterase
Answer: a) CYP3A4
- Which drug combination is contraindicated with lurasidone?
a) Strong CYP3A4 inhibitor
b) Oral rehydration solution
c) Plain calcium supplement only
d) Topical antibiotic
Answer: a) Strong CYP3A4 inhibitor
- Which adverse effect is commonly associated with lurasidone?
a) Akathisia
b) Severe ototoxicity
c) Gingival hyperplasia
d) Bronchospasm in all patients
Answer: a) Akathisia
- Which serious adverse reaction is associated with all antipsychotics including lurasidone?
a) Neuroleptic malignant syndrome
b) Acute appendicitis
c) Irreversible deafness in all patients
d) Severe hypocalcemia only
Answer: a) Neuroleptic malignant syndrome
- Lurasidone is not approved for:
a) Dementia-related psychosis in elderly patients
b) Schizophrenia in adults
c) Bipolar depression in adults
d) Schizophrenia in adolescents aged 13 to 17 years
Answer: a) Dementia-related psychosis in elderly patients
- Low muscarinic M1 receptor affinity of lurasidone suggests lower risk of:
a) Anticholinergic effects
b) Dopamine blockade
c) Serotonin antagonism
d) CYP3A4 metabolism
Answer: a) Anticholinergic effects
- Compared with olanzapine, lurasidone generally has:
a) Lower metabolic burden
b) Higher severe weight gain risk in all patients
c) No antipsychotic activity
d) No dopamine receptor action
Answer: a) Lower metabolic burden
- Which clinical use is approved for Latuda?
a) Depressive episodes associated with bipolar I disorder
b) Acute bacterial meningitis
c) Parkinson’s disease psychosis only
d) Alzheimer’s dementia cure
Answer: a) Depressive episodes associated with bipolar I disorder
FAQs
What is the mechanism of action of Latuda?
Latuda, or lurasidone, works mainly by blocking dopamine D2 receptors and serotonin 5-HT2A receptors. It also blocks 5-HT7 receptors and partially stimulates 5-HT1A receptors, which may contribute to its effects in bipolar depression.
Is lurasidone a typical or atypical antipsychotic?
Lurasidone is an atypical, or second-generation, antipsychotic. It has both dopamine and serotonin receptor activity, unlike older typical antipsychotics that mainly block dopamine D2 receptors.
Why is Latuda used in schizophrenia?
Latuda reduces excessive dopamine D2 receptor signaling in brain pathways associated with psychosis. This helps improve hallucinations, delusions, and disorganized thinking.
Why is Latuda used in bipolar depression?
The exact mechanism in bipolar depression is not fully established. Its effects are thought to involve serotonin-dopamine modulation, especially 5-HT7 antagonism, 5-HT1A partial agonism, and D2/5-HT2A receptor activity.
Why should Latuda be taken with food?
Latuda should be taken with at least 350 calories of food because food significantly increases its absorption. Taking it without enough food may reduce drug exposure and decrease effectiveness.
What is the most common exam-relevant adverse effect of lurasidone?
Akathisia and extrapyramidal symptoms are very important exam points. Somnolence, nausea, and sedation are also common.
Does lurasidone cause weight gain?
Lurasidone can cause weight gain and metabolic changes, but it generally has a lower metabolic risk than some atypical antipsychotics such as olanzapine and clozapine.
Which drugs should be avoided with lurasidone?
Strong CYP3A4 inhibitors and strong CYP3A4 inducers are contraindicated because lurasidone is mainly metabolized by CYP3A4. Grapefruit products are also commonly avoided.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

