
Table of Contents
Introduction
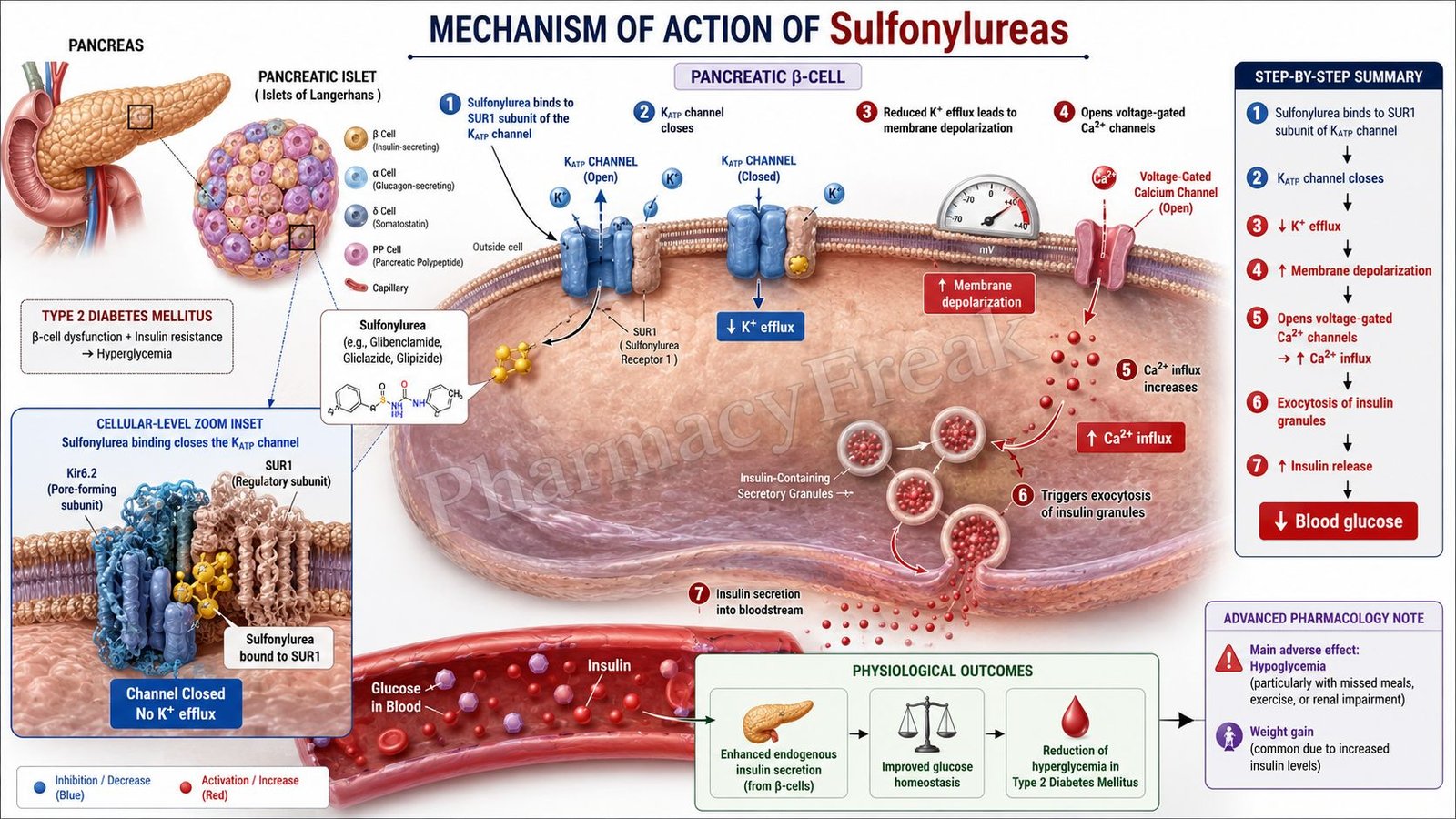
Sulfonylureas are oral antidiabetic drugs used primarily in the treatment of type 2 diabetes mellitus. They lower blood glucose levels by stimulating insulin secretion from pancreatic β-cells. Common sulfonylureas include glibenclamide (glyburide), glipizide, gliclazide, and glimepiride. These drugs are effective only when functional pancreatic β-cells are present.
Mechanism of Action (Step-wise)
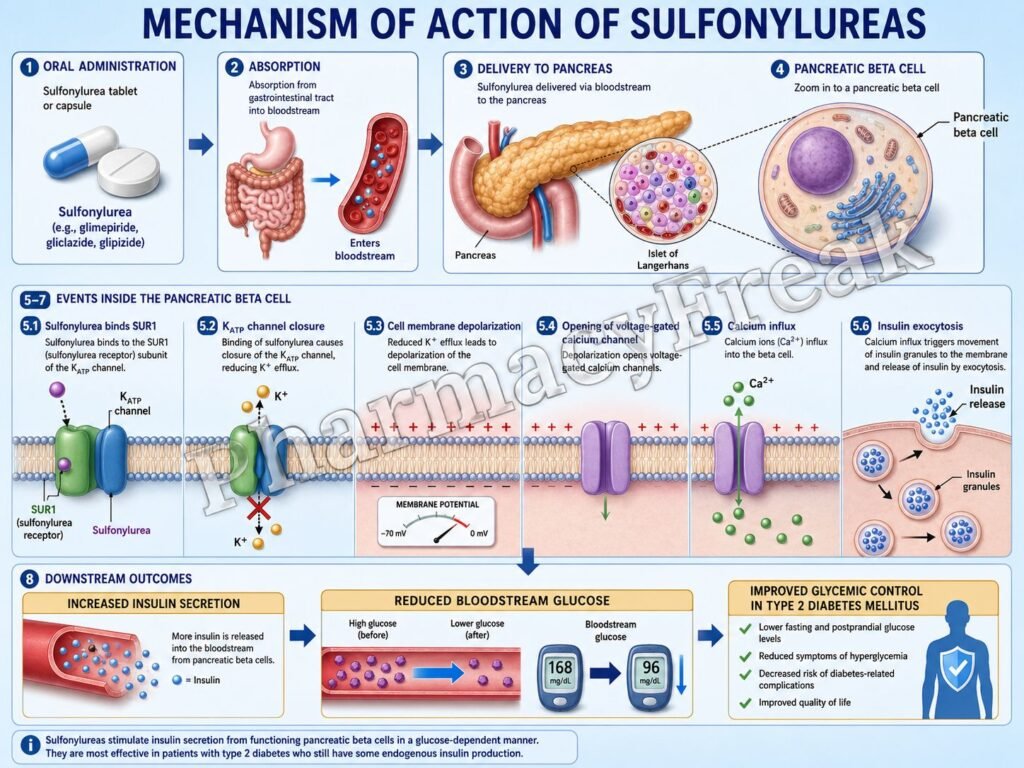
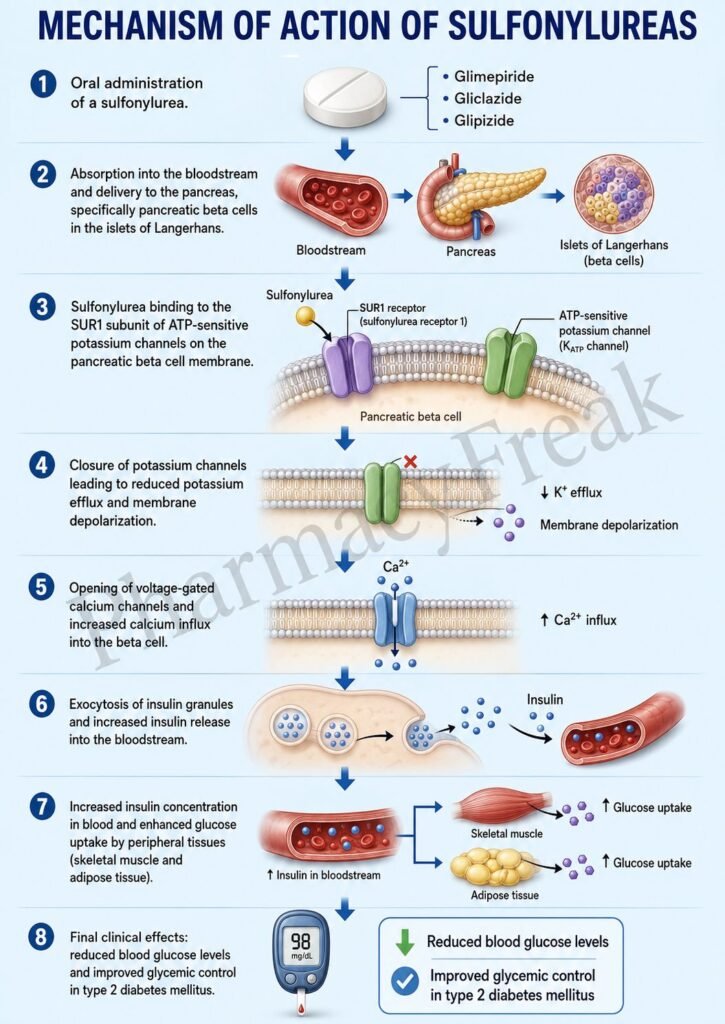
- Sulfonylureas reach pancreatic β-cells after absorption into the bloodstream.
- They bind to the sulfonylurea receptor-1 (SUR1) located on ATP-sensitive potassium (KATP) channels.
- SUR1 is a regulatory subunit of the KATP channel present on β-cell membranes.
- Binding of sulfonylureas causes closure of KATP channels.
- Potassium efflux from the β-cell decreases.
- The β-cell membrane becomes depolarized.
- Membrane depolarization opens voltage-gated calcium channels.
- Calcium influx into the β-cell increases.
- Increased intracellular calcium triggers exocytosis of insulin-containing granules.
- Insulin secretion from pancreatic β-cells rises.
- Increased circulating insulin promotes glucose uptake by muscle and adipose tissue.
- Hepatic glucose production decreases.
- Blood glucose levels fall.
- The overall effect is enhanced endogenous insulin release and improved glycemic control.
A key exam point is that sulfonylureas close ATP-sensitive potassium channels in pancreatic β-cells, leading to insulin release.
Pharmacokinetics
Sulfonylureas are administered orally and are generally well absorbed. Most undergo hepatic metabolism and renal excretion. The duration of action varies among agents, with newer drugs such as glimepiride having a lower risk of prolonged hypoglycemia than older agents.
Clinical Uses
Sulfonylureas are used in:
- Type 2 diabetes mellitus
- Combination therapy with metformin
- Patients with preserved pancreatic β-cell function
They are not effective in type 1 diabetes mellitus because insulin-producing β-cells are absent.
Adverse Effects
Common adverse effects include:
- Hypoglycemia
- Weight gain
- Nausea
- Dizziness
Serious adverse effects may include:
- Severe hypoglycemia
- Cholestatic jaundice
- Allergic reactions
- Hematological abnormalities (rare)
Comparative Analysis
| Feature | Sulfonylureas | Metformin | Meglitinides |
|---|---|---|---|
| Main action | Stimulate insulin release | Reduce hepatic glucose production | Stimulate insulin release |
| Target | SUR1 receptor | AMPK activation | SUR1 receptor |
| Requires β-cells | Yes | No | Yes |
| Hypoglycemia risk | High | Low | Moderate |
| Weight gain | Common | Neutral/weight loss | Mild |
| First-line therapy | No | Yes | No |
Sulfonylureas differ from metformin because they increase insulin secretion rather than improving insulin sensitivity. Compared with meglitinides, sulfonylureas have a longer duration of action and a higher risk of hypoglycemia.
MCQs
1. Sulfonylureas primarily act on:
a) Liver cells
b) Pancreatic β-cells
c) Skeletal muscle
d) Adipose tissue
Answer: b) Pancreatic β-cells
2. Sulfonylureas bind to:
a) GLUT4 receptors
b) SUR1 receptors
c) Insulin receptors
d) PPAR-γ receptors
Answer: b) SUR1 receptors
3. Sulfonylureas cause closure of:
a) Sodium channels
b) Calcium channels
c) ATP-sensitive potassium channels
d) Chloride channels
Answer: c) ATP-sensitive potassium channels
4. Closure of KATP channels causes:
a) Hyperpolarization
b) Depolarization
c) Repolarization
d) Apoptosis
Answer: b) Depolarization
5. Depolarization opens:
a) Potassium channels
b) Voltage-gated calcium channels
c) Chloride channels
d) Sodium pumps
Answer: b) Voltage-gated calcium channels
6. Increased intracellular calcium leads to:
a) Glucose synthesis
b) Insulin release
c) Glycogen breakdown
d) Lipolysis
Answer: b) Insulin release
7. Sulfonylureas are used in:
a) Type 1 diabetes
b) Type 2 diabetes
c) Diabetes insipidus
d) Gestational diabetes only
Answer: b) Type 2 diabetes
8. The most common serious adverse effect is:
a) Hypoglycemia
b) Hypercalcemia
c) Hypertension
d) Cataracts
Answer: a) Hypoglycemia
9. Sulfonylureas generally cause:
a) Weight loss
b) Weight gain
c) Severe dehydration
d) Hyperthyroidism
Answer: b) Weight gain
10. Which drug is a sulfonylurea?
a) Metformin
b) Glimepiride
c) Pioglitazone
d) Sitagliptin
Answer: b) Glimepiride
11. Sulfonylureas are ineffective when:
a) β-cells are absent
b) Glucose is elevated
c) Insulin resistance exists
d) Food is consumed
Answer: a) β-cells are absent
12. The final effect of sulfonylureas is:
a) Increased insulin secretion
b) Decreased insulin secretion
c) Increased glucagon secretion
d) Increased ketogenesis
Answer: a) Increased insulin secretion
FAQs
What is the mechanism of action of sulfonylureas?
Sulfonylureas close ATP-sensitive potassium channels in pancreatic β-cells, leading to insulin secretion.
Why do sulfonylureas require functioning β-cells?
Because their glucose-lowering effect depends on stimulating endogenous insulin release.
What receptor do sulfonylureas bind to?
They bind to the sulfonylurea receptor-1 (SUR1) on KATP channels.
What is the major adverse effect of sulfonylureas?
Hypoglycemia.
Do sulfonylureas cause weight gain?
Yes, weight gain is a common adverse effect because of increased insulin levels.
How do sulfonylureas differ from metformin?
Sulfonylureas stimulate insulin secretion, whereas metformin primarily reduces hepatic glucose production and improves insulin sensitivity.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung’s Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi KD. Essentials of Medical Pharmacology
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com

