
Table of Contents
Introduction
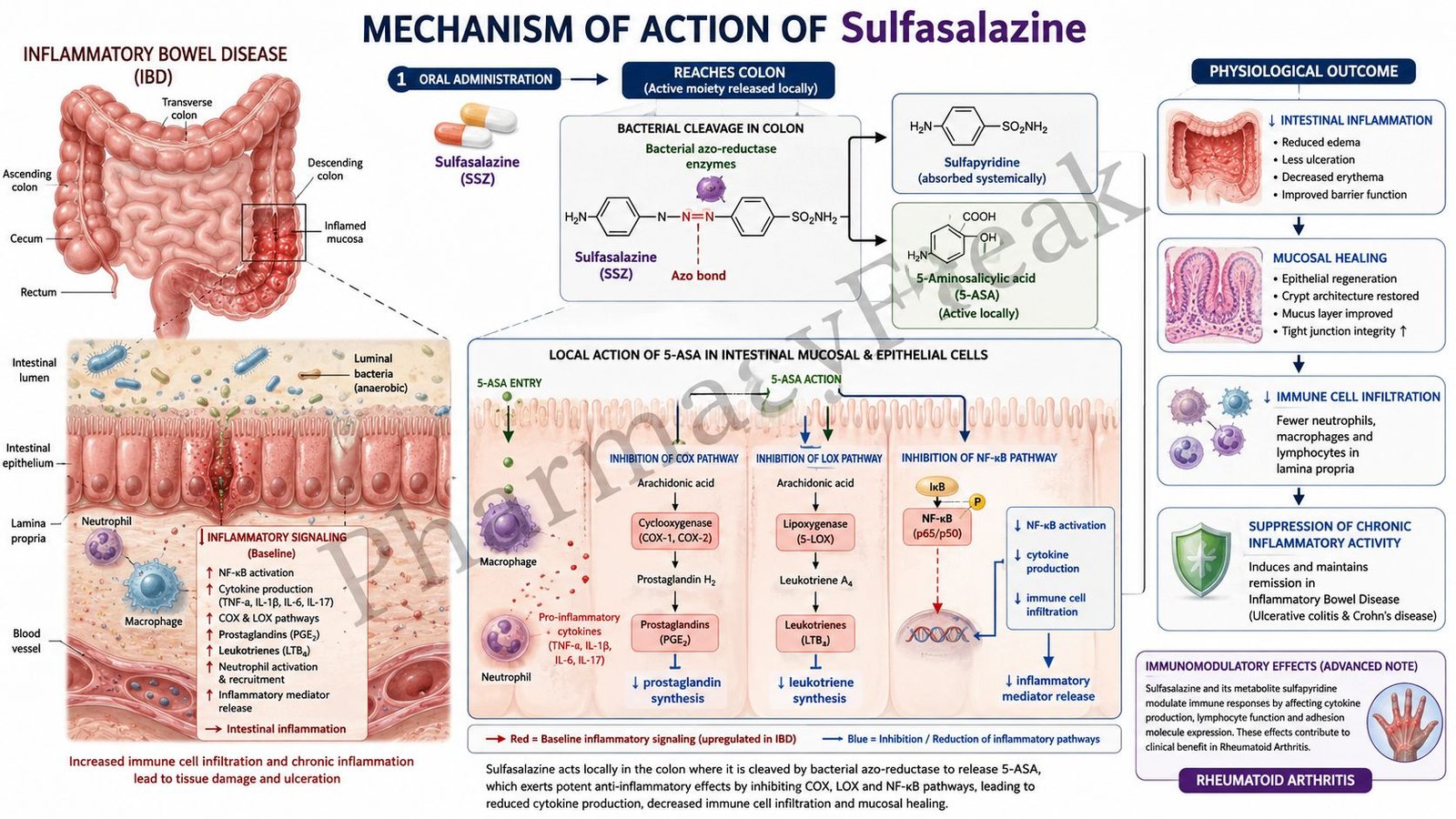
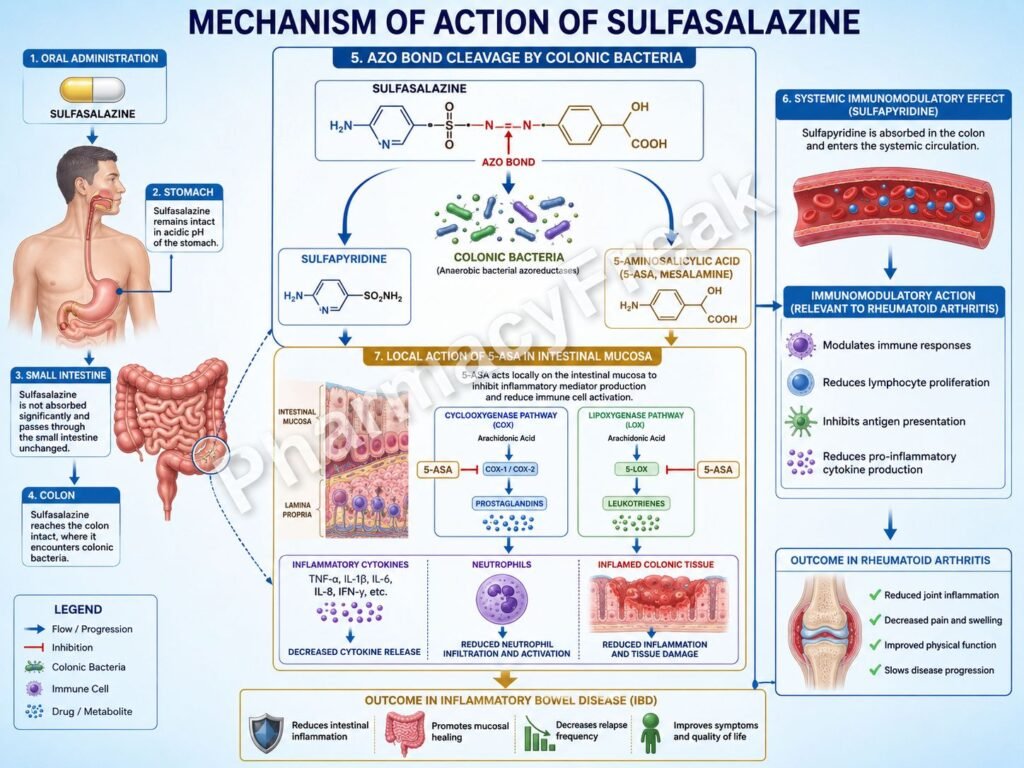
Sulfasalazine is a disease-modifying antirheumatic drug (DMARD) and anti-inflammatory agent used primarily in inflammatory bowel disease (IBD), rheumatoid arthritis, and other autoimmune disorders. It is a prodrug consisting of sulfapyridine linked to 5-aminosalicylic acid (5-ASA, mesalamine) by an azo bond. After reaching the colon, bacterial enzymes cleave the bond, releasing the active components that exert anti-inflammatory and immunomodulatory effects.
Mechanism of Action (Step-wise)
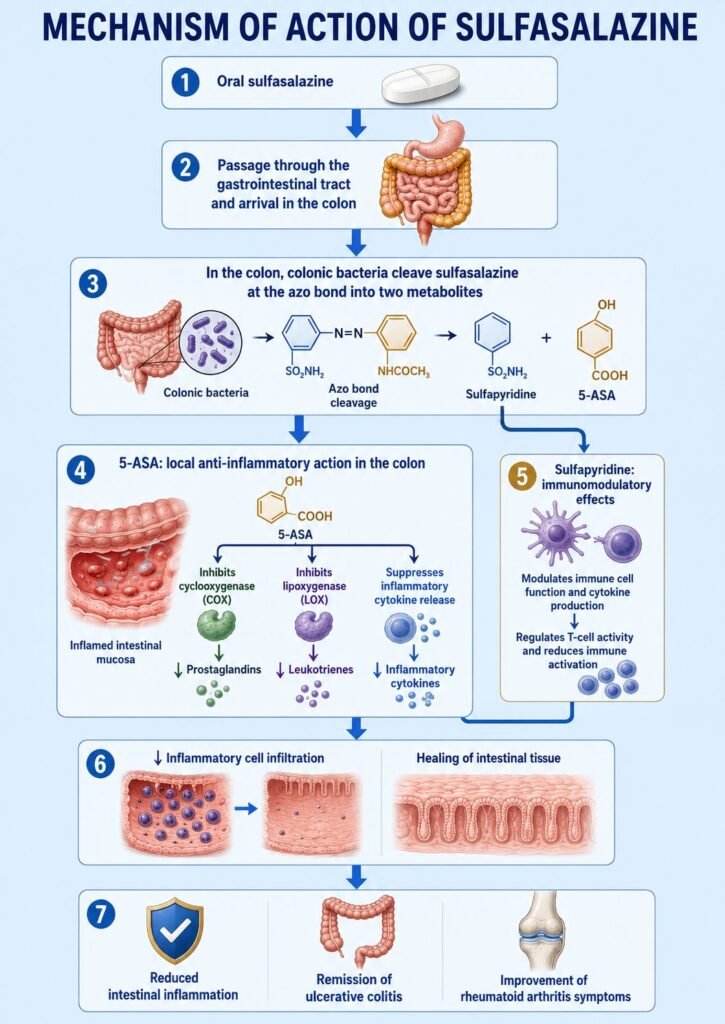
- Sulfasalazine is administered orally and passes largely unchanged through the small intestine.
- In the colon, bacterial azoreductase enzymes cleave the azo bond.
- This cleavage releases two active metabolites:
- Sulfapyridine
- 5-Aminosalicylic acid (5-ASA, mesalamine)
- 5-ASA acts locally on the intestinal mucosa.
- It inhibits cyclooxygenase (COX) and lipoxygenase pathways.
- Production of inflammatory mediators such as prostaglandins and leukotrienes decreases.
- 5-ASA also scavenges reactive oxygen species and free radicals within inflamed intestinal tissue.
- Sulfasalazine suppresses production of inflammatory cytokines including TNF-α, IL-1, and IL-6.
- Activation and proliferation of T lymphocytes are reduced.
- In rheumatoid arthritis, immune-mediated joint inflammation decreases.
- Leukocyte migration and inflammatory cell infiltration are inhibited.
- The overall effect is reduced intestinal inflammation and suppression of autoimmune inflammatory responses.
A key exam point is that sulfasalazine is converted in the colon to 5-ASA and sulfapyridine, leading to inhibition of prostaglandins, leukotrienes, and inflammatory cytokines.
Pharmacokinetics
Sulfasalazine is administered orally. Approximately 10–30% is absorbed from the small intestine, while the remainder reaches the colon where bacterial metabolism occurs. Sulfapyridine is absorbed systemically and metabolized in the liver, whereas much of the 5-ASA remains in the gut and acts locally. Elimination occurs primarily through urine.
Clinical Uses
Sulfasalazine is used in:
- Ulcerative colitis
- Crohn disease (selected cases)
- Rheumatoid arthritis
- Juvenile idiopathic arthritis
- Ankylosing spondylitis
- Other inflammatory arthritides
Adverse Effects
Common adverse effects include:
- Nausea
- Vomiting
- Headache
- Abdominal discomfort
- Rash
- Reversible oligospermia
Serious adverse effects may include:
- Agranulocytosis
- Hemolytic anemia
- Hepatotoxicity
- Stevens-Johnson syndrome
- Bone marrow suppression
Folic acid deficiency may occur with prolonged therapy.
Comparative Analysis
| Feature | Sulfasalazine | Mesalamine | Methotrexate |
|---|---|---|---|
| Drug class | DMARD / 5-ASA prodrug | 5-ASA derivative | DMARD |
| Activation by colonic bacteria | Yes | No | No |
| Main use in IBD | Yes | Yes | Limited |
| Rheumatoid arthritis use | Yes | No | Yes |
| Cytokine suppression | Moderate | Mild | Strong |
| Bone marrow suppression risk | Present | Rare | Significant |
Sulfasalazine differs from mesalamine because it is a prodrug that requires bacterial activation and also possesses systemic immunomodulatory effects useful in rheumatoid arthritis. Compared with methotrexate, sulfasalazine is generally less immunosuppressive but is frequently used as part of combination DMARD therapy.
MCQs
1. Sulfasalazine is a combination of:
a) Prednisone and mesalamine
b) Sulfapyridine and 5-ASA
c) Methotrexate and folic acid
d) Sulfamethoxazole and trimethoprim
Answer: b) Sulfapyridine and 5-ASA
2. Sulfasalazine is activated primarily in the:
a) Stomach
b) Small intestine
c) Colon
d) Liver
Answer: c) Colon
3. The azo bond of sulfasalazine is cleaved by:
a) Pancreatic enzymes
b) Hepatic enzymes
c) Bacterial azoreductases
d) Renal enzymes
Answer: c) Bacterial azoreductases
4. The major anti-inflammatory intestinal metabolite is:
a) Sulfapyridine
b) Mesalamine (5-ASA)
c) Prednisolone
d) Acetylsalicylic acid
Answer: b) Mesalamine (5-ASA)
5. Sulfasalazine inhibits production of:
a) Prostaglandins and leukotrienes
b) Insulin and glucagon
c) Dopamine and serotonin
d) Histamine only
Answer: a) Prostaglandins and leukotrienes
6. Sulfasalazine is commonly used in:
a) Ulcerative colitis
b) Asthma
c) Hypertension
d) Epilepsy
Answer: a) Ulcerative colitis
7. Sulfasalazine is classified as:
a) DMARD
b) β blocker
c) Anticoagulant
d) Antiviral
Answer: a) DMARD
8. A common adverse effect is:
a) Headache
b) Hypercalcemia
c) Cataracts
d) Bradycardia
Answer: a) Headache
9. A serious adverse effect is:
a) Agranulocytosis
b) Hypernatremia
c) Hypoglycemia
d) Glaucoma
Answer: a) Agranulocytosis
10. Sulfasalazine may cause:
a) Reversible oligospermia
b) Permanent infertility
c) Hyperthyroidism
d) Hyperkalemia
Answer: a) Reversible oligospermia
11. Sulfasalazine suppresses production of:
a) TNF-α
b) Thyroxine
c) Cortisol
d) Insulin
Answer: a) TNF-α
12. Sulfasalazine improves rheumatoid arthritis mainly through:
a) Immunomodulatory effects
b) Dopamine blockade
c) Histamine release inhibition only
d) Calcium channel blockade
Answer: a) Immunomodulatory effects
FAQs
What is the mechanism of action of sulfasalazine?
Sulfasalazine is converted in the colon into 5-ASA and sulfapyridine, which reduce inflammatory mediator production and suppress immune responses.
Why is sulfasalazine used in ulcerative colitis?
Because 5-ASA acts locally in the colon to reduce mucosal inflammation.
How does sulfasalazine help rheumatoid arthritis?
It suppresses inflammatory cytokines and immune cell activation involved in joint inflammation.
What are the active metabolites of sulfasalazine?
5-Aminosalicylic acid (5-ASA) and sulfapyridine.
What are common side effects of sulfasalazine?
Nausea, headache, abdominal discomfort, and rash.
Why is folic acid supplementation often recommended with sulfasalazine?
Because long-term therapy may impair folate absorption and contribute to folate deficiency.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung’s Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi KD. Essentials of Medical Pharmacology
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com

