
Table of Contents
Introduction
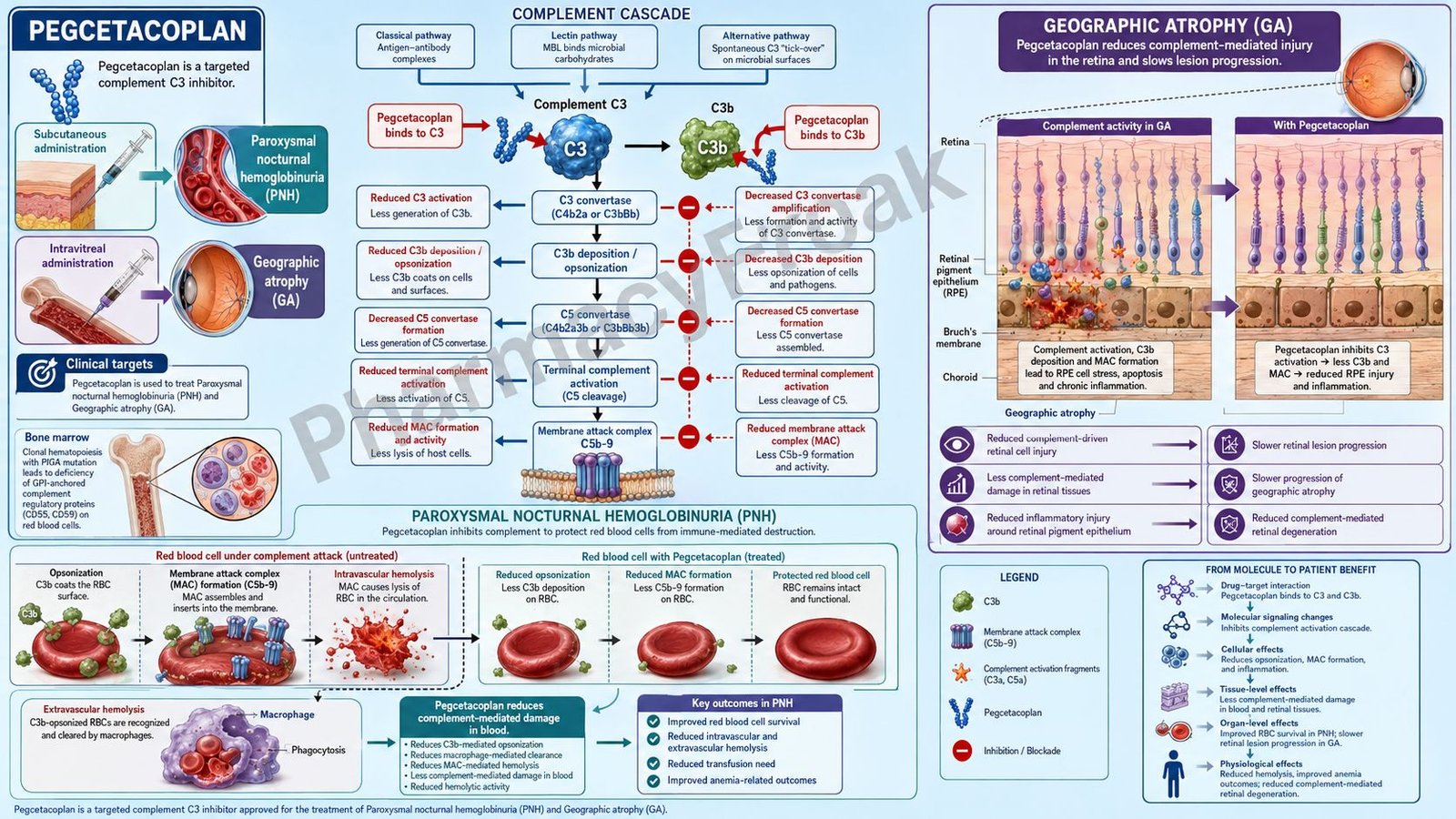
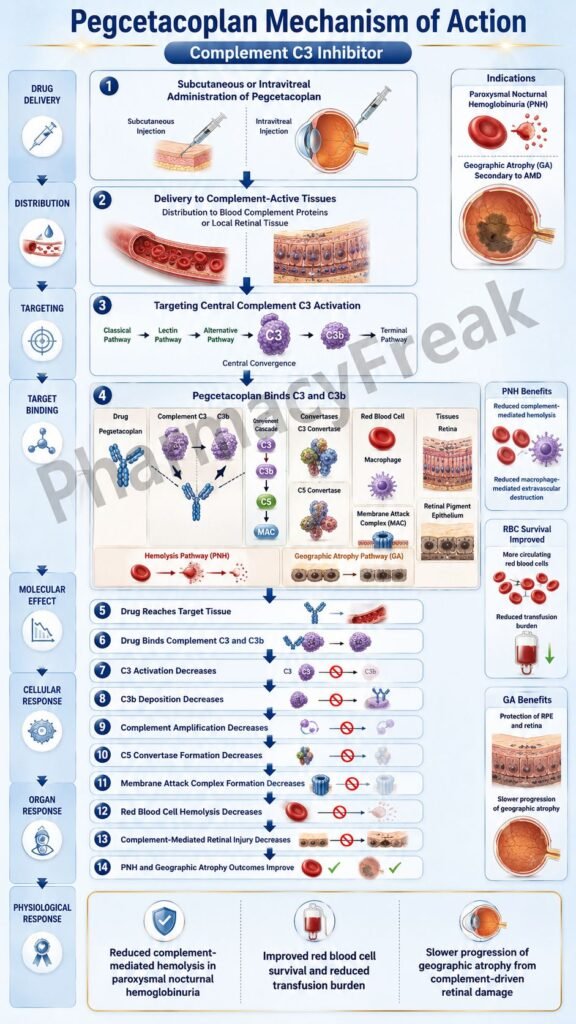
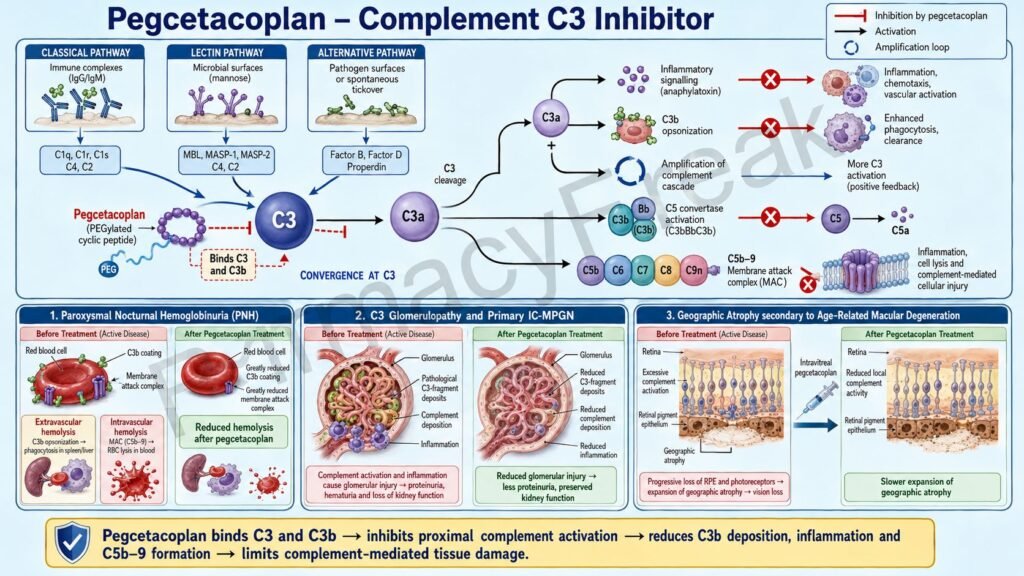
Pegcetacoplan is a targeted complement inhibitor used in diseases driven by abnormal activation of the complement system. It is marketed as Empaveli for systemic use and as Syfovre for intravitreal ophthalmic use. Empaveli is used for adult patients with paroxysmal nocturnal hemoglobinuria, commonly called PNH, and is also indicated for adults and pediatric patients aged 12 years and older with C3 glomerulopathy or primary immune-complex membranoproliferative glomerulonephritis to reduce proteinuria. Syfovre is used for geographic atrophy secondary to age-related macular degeneration. These products contain the same active drug, pegcetacoplan, but they differ in route, dose, formulation, and clinical indication.
Pharmacologically, pegcetacoplan is a complement C3 inhibitor. Complement C3 is a central protein in the complement cascade because the classical, lectin, and alternative complement pathways all converge at C3 activation. When C3 is activated, it generates C3a, C3b, C5 convertase activity, and downstream terminal complement effects including membrane attack complex formation.
The major importance of pegcetacoplan is that it acts proximally in the complement cascade. By binding to C3 and C3b, pegcetacoplan reduces both upstream C3-mediated effects and downstream terminal complement activation. This makes it different from C5 inhibitors such as eculizumab and ravulizumab, which block terminal complement but do not directly block C3b-mediated opsonization.
For exam purposes, pegcetacoplan should be remembered as a pegylated peptide complement inhibitor that binds C3 and C3b, blocks C3 cleavage, reduces C3b deposition, decreases C5 convertase activity, and prevents downstream complement-mediated tissue injury.
Mechanism of Action (Step-wise)
Step 1: The complement system becomes activated
The complement system is part of innate immunity. It can be activated by the classical pathway, lectin pathway, or alternative pathway. Although these pathways begin differently, all of them converge on complement protein C3.
Step 2: C3 is cleaved into C3a and C3b
After complement activation, C3 convertase cleaves C3 into C3a and C3b. C3a acts as an inflammatory mediator, while C3b attaches to cell surfaces and acts as an opsonin. C3b also helps form C5 convertase, which pushes the cascade toward terminal complement activation.
Step 3: C5 convertase promotes terminal complement activation
C5 convertase cleaves C5 into C5a and C5b. C5a is a potent inflammatory mediator. C5b participates in the formation of the membrane attack complex, also called MAC or C5b-9. MAC can damage or lyse susceptible cells.
Step 4: Pegcetacoplan binds to C3 and C3b
Pegcetacoplan binds to complement protein C3 and its activation fragment C3b. By binding these targets, it regulates C3 cleavage and reduces generation of downstream complement effectors. This is the central molecular action of pegcetacoplan.
Step 5: C3 cleavage is inhibited
When pegcetacoplan binds C3, less C3 is available for activation by C3 convertase. This reduces formation of C3a and C3b. As a result, inflammation, opsonization, and downstream complement amplification decrease.
Step 6: C3b-mediated opsonization decreases
C3b normally marks cells for immune clearance. In diseases such as PNH, C3b deposition on red blood cells promotes extravascular hemolysis, mainly through phagocytic clearance in the liver and spleen. By reducing C3b deposition, pegcetacoplan decreases this C3-mediated cell destruction.
Step 7: C5 convertase activity decreases
Because C3b is needed for efficient C5 convertase formation, inhibition of C3 and C3b also reduces C5 convertase activity. This decreases cleavage of C5 and reduces downstream formation of C5a and C5b-9.
Step 8: Membrane attack complex formation decreases
Reduced C5b-9 formation means less terminal complement-mediated cell membrane damage. In PNH, this helps reduce intravascular hemolysis, which is the destruction of red blood cells inside blood vessels.
Step 9: In PNH, both extravascular and intravascular hemolysis are reduced
PNH red blood cells are vulnerable to complement-mediated destruction because they lack key complement-regulatory proteins such as CD55 and CD59. Pegcetacoplan acts proximally and controls both C3b-mediated extravascular hemolysis and terminal complement-mediated intravascular hemolysis.
Step 10: In C3G and primary IC-MPGN, glomerular complement injury decreases
In C3 glomerulopathy and primary immune-complex membranoproliferative glomerulonephritis, complement dysregulation causes deposition of C3 fragments in glomeruli. Pegcetacoplan inhibits C3 activation, decreases C3 glomerular fragment deposition, decreases C5 convertase activity, and reduces C5b-9 assembly. This helps reduce proteinuria and kidney inflammation.
Step 11: In geographic atrophy, local retinal complement injury is reduced
In geographic atrophy secondary to age-related macular degeneration, complement overactivation contributes to retinal pigment epithelial injury, photoreceptor loss, and lesion expansion. Intravitreal pegcetacoplan blocks C3 locally in the eye and slows progression of geographic atrophy lesions. It does not regenerate lost retinal tissue or cure age-related macular degeneration.
Step 12: Final therapeutic outcome depends on disease
In PNH, the outcome is reduced hemolysis, improved anemia, and reduced transfusion requirement in appropriate patients. In C3G and primary IC-MPGN, the outcome is reduction in proteinuria. In geographic atrophy, the outcome is slowing of lesion growth rather than rapid visual restoration.
Pharmacokinetics
Pegcetacoplan is not an oral small-molecule drug. It is a pegylated peptide-based complement inhibitor. Empaveli is administered by subcutaneous infusion, while Syfovre is administered by intravitreal injection into the eye.
For PNH, Empaveli is given as 1,080 mg subcutaneously twice weekly. When switching from eculizumab, pegcetacoplan is started while continuing eculizumab for 4 weeks before eculizumab is discontinued. When switching from ravulizumab, pegcetacoplan is started no more than 4 weeks after the last ravulizumab dose.
For C3 glomerulopathy or primary immune-complex membranoproliferative glomerulonephritis, Empaveli is also administered subcutaneously, with adult dosing listed as 1,080 mg twice weekly and pediatric dosing adjusted according to body weight.
For geographic atrophy, Syfovre is given as 15 mg, or 0.1 mL of a 150 mg/mL solution, by intravitreal injection to each affected eye once every 25 to 60 days. It must be administered by a qualified physician using aseptic intravitreal injection technique.
After subcutaneous administration, pegcetacoplan has slow absorption, with median Tmax between 108 and 144 hours, or about 4.5 to 6 days. In PNH, steady-state serum concentrations are reached in about 4 to 6 weeks. In C3G or primary IC-MPGN, steady state is reached in about 4 to 8 weeks with twice-weekly subcutaneous infusion.
Pegcetacoplan has a small volume of distribution, consistent with a large pegylated molecule. Its effective half-life is about 8.6 days in PNH and around 10 days in C3G or primary IC-MPGN. It is expected to be metabolized into small peptides and amino acids through catabolic pathways rather than cytochrome P450 metabolism. Therefore, classic CYP-mediated drug interactions are not a major issue.
Clinical Uses
Pegcetacoplan is used in adult patients with paroxysmal nocturnal hemoglobinuria. PNH is an acquired clonal hematopoietic stem cell disorder in which blood cells lack complement-regulatory surface proteins. This makes red blood cells vulnerable to complement-mediated hemolysis.
Pegcetacoplan is also used in adults and pediatric patients aged 12 years and older with C3 glomerulopathy or primary immune-complex membranoproliferative glomerulonephritis to reduce proteinuria. This is an important current indication because it extends pegcetacoplan beyond hematology into complement-mediated kidney disease.
Pegcetacoplan is also used as Syfovre for geographic atrophy secondary to age-related macular degeneration. In this setting, it is injected into the eye and works locally by inhibiting complement C3 activity in the retina. It slows lesion growth but does not reverse existing atrophy.
In PNH, pegcetacoplan may be especially useful when C5 inhibitor therapy controls intravascular hemolysis but patients continue to have anemia due to C3-mediated extravascular hemolysis.
In kidney disease, its role is based on the concept that complement dysregulation drives glomerular C3 fragment deposition, inflammation, and proteinuria.
In ophthalmology, its role is disease modification in geographic atrophy, not acute visual improvement. Patients should be counseled that treatment aims to slow progression rather than restore lost retinal cells.
Adverse Effects
The most important systemic safety warning for Empaveli is serious and life-threatening infection caused by encapsulated bacteria. Important organisms include Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae type B. Vaccination against encapsulated bacteria is required before therapy when possible, and urgent treatment may require antibacterial prophylaxis. Empaveli is available only through a REMS program because of this risk.
Vaccination does not completely eliminate the risk of serious infection. Patients must be educated to seek urgent care for fever, headache with stiff neck, confusion, rash, shortness of breath, flu-like symptoms, or other signs of invasive bacterial infection.
Common adverse effects with systemic pegcetacoplan include injection-site reactions, infections, diarrhea, abdominal pain, respiratory tract infection, viral infection, fatigue, pyrexia, cough, nausea, dizziness, headache, rash, arthralgia, and hypokalemia. Infusion-related reactions and hypersensitivity, including anaphylaxis and urticaria, may occur.
After discontinuation in PNH, patients may develop recurrence of hemolysis. Therefore, monitoring is required after stopping therapy. Laboratory and clinical monitoring may include lactate dehydrogenase, hemoglobin, bilirubin, symptoms of hemolysis, and thrombotic risk assessment.
Pegcetacoplan may interfere with some coagulation laboratory tests, especially assays using silica reagents, causing artificially prolonged activated partial thromboplastin time. This is an exam-relevant laboratory point.
For Syfovre, important ocular adverse effects include endophthalmitis, retinal detachment, retinal vasculitis with or without retinal vascular occlusion, neovascular age-related macular degeneration, intraocular inflammation, increased intraocular pressure, vitreous floaters, conjunctival hemorrhage, and ocular discomfort. Retinal vasculitis or retinal vascular occlusion may result in severe vision loss and requires discontinuation if it occurs.
Pregnancy data are limited. For systemic Empaveli, effective contraception is recommended for females of reproductive potential during treatment and for 40 days after the last dose, and breastfeeding should be discontinued during treatment and for 40 days after the last dose.
Comparative Analysis
Pegcetacoplan is most commonly compared with C5 inhibitors such as eculizumab and ravulizumab. Eculizumab and ravulizumab block complement C5, thereby preventing C5a formation and membrane attack complex formation. They are very effective against intravascular hemolysis in PNH but do not directly prevent C3b deposition on red blood cells.
Pegcetacoplan acts earlier at C3 and C3b. Because C3 is upstream of C5, pegcetacoplan reduces both C3b-mediated extravascular hemolysis and terminal complement-mediated intravascular hemolysis. This is the key pharmacological difference from C5 inhibitors.
Compared with proximal complement factor B or factor D inhibitors, pegcetacoplan directly targets C3, the central convergence point of all complement pathways. Factor B and factor D inhibitors mainly affect the alternative pathway amplification loop, while C3 inhibition has a broader complement-blocking effect.
Compared with corticosteroids or broad immunosuppressants used in some inflammatory kidney diseases, pegcetacoplan is more pathway-specific. It targets complement C3 activation rather than broadly suppressing many immune pathways.
In geographic atrophy, pegcetacoplan is compared with avacincaptad pegol, another complement inhibitor used for GA. Pegcetacoplan targets C3, while avacincaptad pegol targets C5. Both aim to slow GA progression, but they act at different complement levels.
Compared with anti-VEGF drugs used for wet AMD, pegcetacoplan has a different purpose. Anti-VEGF drugs treat neovascular AMD by blocking abnormal blood vessel growth and leakage. Pegcetacoplan treats geographic atrophy by inhibiting complement-mediated retinal injury. If neovascular AMD develops during Syfovre treatment, anti-VEGF therapy may be needed separately.
MCQs
- Pegcetacoplan primarily inhibits which complement protein?
a) C1q
b) C3
c) C5 only
d) Factor Xa
Answer: b) C3
- The systemic brand name of pegcetacoplan used in PNH is:
a) Empaveli
b) Syfovre
c) Soliris
d) Ultomiris
Answer: a) Empaveli
- Syfovre contains pegcetacoplan and is used for:
a) Wet AMD only
b) Geographic atrophy secondary to age-related macular degeneration
c) Acute bacterial conjunctivitis
d) Diabetic ketoacidosis
Answer: b) Geographic atrophy secondary to age-related macular degeneration
- Pegcetacoplan binds to:
a) C3 and C3b
b) C5a receptor only
c) VEGF-A only
d) TNF-alpha only
Answer: a) C3 and C3b
- In PNH, C3b opsonization mainly contributes to:
a) Extravascular hemolysis
b) Bronchodilation
c) Insulin secretion
d) Bone mineralization
Answer: a) Extravascular hemolysis
- In PNH, terminal complement-mediated membrane attack complex formation mainly contributes to:
a) Intravascular hemolysis
b) Gastric acid secretion
c) Dopamine release
d) Glucose uptake
Answer: a) Intravascular hemolysis
- Which statement best describes pegcetacoplan?
a) It blocks only the terminal C5 pathway
b) It acts proximally in the complement cascade by inhibiting C3/C3b
c) It is an oral anticoagulant
d) It is a dopamine receptor blocker
Answer: b) It acts proximally in the complement cascade by inhibiting C3/C3b
- Which infection risk is most important with systemic pegcetacoplan?
a) Serious infection with encapsulated bacteria
b) Dermatophyte infection only
c) Candida vaginitis only
d) Viral warts only
Answer: a) Serious infection with encapsulated bacteria
- Which organism is especially relevant to the boxed warning of Empaveli?
a) Neisseria meningitidis
b) Helicobacter pylori
c) Plasmodium vivax
d) Clostridioides difficile only
Answer: a) Neisseria meningitidis
- Before systemic pegcetacoplan therapy, patients should generally receive vaccination against:
a) Encapsulated bacteria
b) Only hepatitis A
c) Only rabies
d) Only varicella zoster in all cases
Answer: a) Encapsulated bacteria
- Pegcetacoplan is indicated in C3 glomerulopathy or primary IC-MPGN mainly to reduce:
a) Proteinuria
b) Blood glucose
c) Gastric acid
d) Serum cholesterol only
Answer: a) Proteinuria
- Syfovre is administered by which route?
a) Intravitreal injection
b) Oral tablet
c) Intramuscular depot only
d) Sublingual spray
Answer: a) Intravitreal injection
- Which serious ocular adverse effect has been reported with Syfovre?
a) Retinal vasculitis with or without retinal vascular occlusion
b) Mandatory cataract in every patient
c) Complete eyelash loss
d) Acute angle closure in all patients
Answer: a) Retinal vasculitis with or without retinal vascular occlusion
- Pegcetacoplan differs from eculizumab because pegcetacoplan:
a) Targets C3, while eculizumab targets C5
b) Targets VEGF, while eculizumab targets dopamine
c) Is an antibiotic, while eculizumab is an antiviral
d) Is used only for hypertension
Answer: a) Targets C3, while eculizumab targets C5
- Pegcetacoplan is expected to be metabolized mainly into:
a) Small peptides and amino acids by catabolic pathways
b) Active CYP3A4 metabolites only
c) Acetylcholine
d) Bile acids only
Answer: a) Small peptides and amino acids by catabolic pathways
FAQs
What is the mechanism of action of pegcetacoplan?
Pegcetacoplan binds to complement protein C3 and its activation fragment C3b. This inhibits C3 cleavage, reduces C3b deposition, decreases C5 convertase activity, and reduces downstream complement-mediated inflammation and cell injury.
What is the brand name of pegcetacoplan?
Pegcetacoplan is marketed as Empaveli for systemic subcutaneous use and as Syfovre for intravitreal ophthalmic use.
Why is C3 inhibition important?
C3 is the central convergence point of the classical, lectin, and alternative complement pathways. Inhibiting C3 blocks both upstream C3-mediated effects and downstream terminal complement activation.
How does pegcetacoplan help in PNH?
In PNH, pegcetacoplan reduces both C3b-mediated extravascular hemolysis and membrane attack complex-mediated intravascular hemolysis. This helps reduce red blood cell destruction and improves anemia in appropriate patients.
How is pegcetacoplan different from eculizumab?
Pegcetacoplan inhibits C3 and C3b, while eculizumab inhibits C5. Because pegcetacoplan acts upstream, it can reduce both C3-mediated extravascular hemolysis and terminal complement-mediated intravascular hemolysis.
What is the most important safety warning with Empaveli?
The most important warning is serious and life-threatening infection caused by encapsulated bacteria, including Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae type B.
What is pegcetacoplan used for in kidney disease?
Empaveli is used in adults and pediatric patients aged 12 years and older with C3 glomerulopathy or primary immune-complex membranoproliferative glomerulonephritis to reduce proteinuria.
Does Syfovre improve vision immediately?
No. Syfovre is used to slow the progression of geographic atrophy lesions secondary to age-related macular degeneration. It does not regenerate lost retinal cells or provide immediate visual restoration.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

