
Table of Contents
Introduction
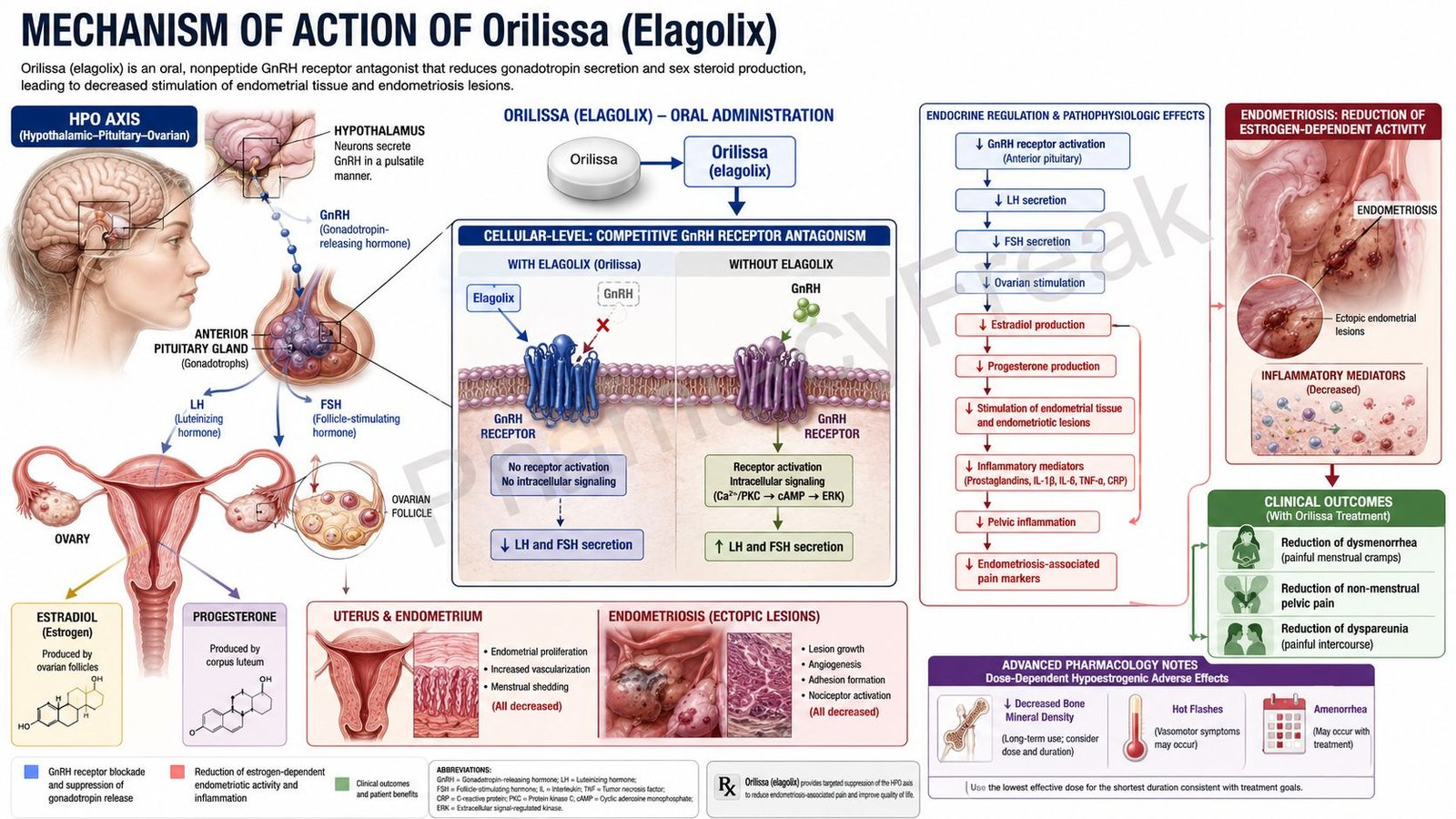
Orilissa is the brand name of elagolix, an oral nonpeptide gonadotropin-releasing hormone receptor antagonist used for the management of moderate to severe pain associated with endometriosis. Endometriosis is a chronic estrogen-dependent inflammatory disorder in which endometrial-like tissue grows outside the uterus, commonly on the ovaries, fallopian tubes, pelvic peritoneum, uterosacral ligaments, bowel, or bladder.
These ectopic endometrial implants respond to ovarian hormones, especially estrogen. Estrogen promotes lesion growth, local inflammation, angiogenesis, nerve sensitization, fibrosis, and cyclic bleeding within ectopic tissue. This produces symptoms such as dysmenorrhea, non-menstrual pelvic pain, dyspareunia, painful bowel movements, painful urination, and infertility in some patients.
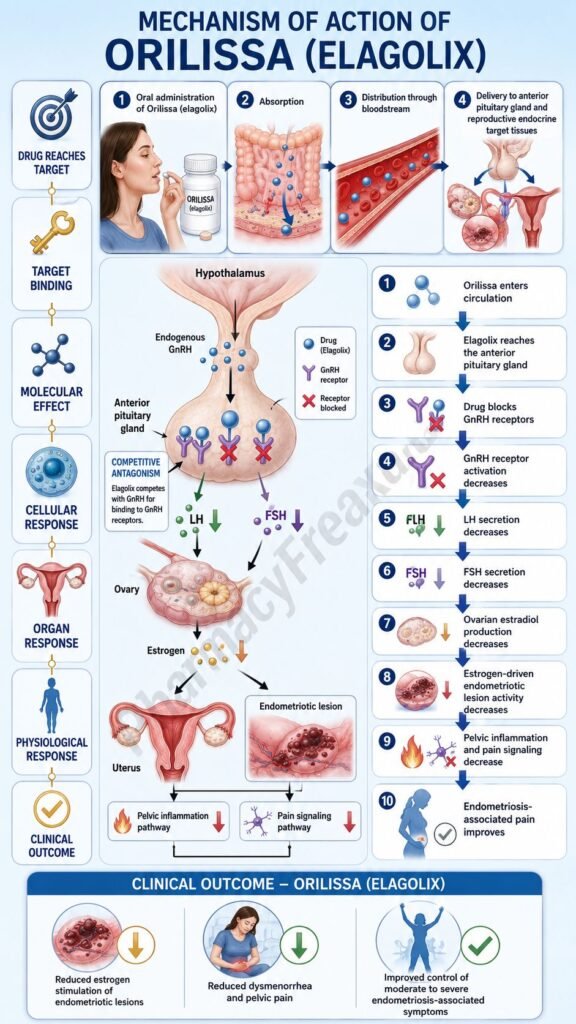
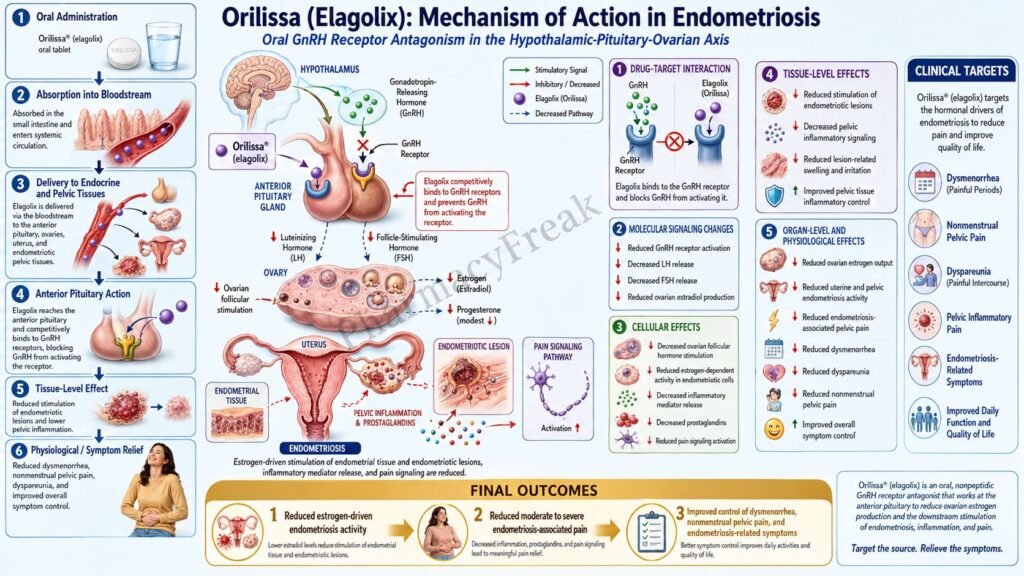
Elagolix works by blocking gonadotropin-releasing hormone receptors in the pituitary gland. This reduces secretion of luteinizing hormone and follicle-stimulating hormone, leading to a dose-dependent reduction in ovarian estrogen and progesterone production. Lower estrogen levels reduce stimulation of endometriotic lesions and help decrease endometriosis-associated pain.
For exam purposes, Orilissa should be remembered as an oral GnRH receptor antagonist that directly and competitively blocks pituitary GnRH receptors, causing reversible, dose-dependent suppression of LH, FSH, estradiol, and progesterone. It is different from GnRH agonists such as leuprolide, which initially cause a flare before suppressing the hypothalamic-pituitary-gonadal axis.
Mechanism of Action (Step-wise)
Step 1: Normal GnRH is released from the hypothalamus
In normal reproductive physiology, the hypothalamus releases gonadotropin-releasing hormone, commonly called GnRH, in a pulsatile manner. GnRH travels through the hypothalamic-pituitary portal circulation and reaches the anterior pituitary gland.
Step 2: GnRH activates pituitary GnRH receptors
GnRH binds to GnRH receptors on anterior pituitary gonadotroph cells. This receptor stimulation promotes synthesis and release of two important gonadotropins: luteinizing hormone, or LH, and follicle-stimulating hormone, or FSH.
Step 3: LH and FSH stimulate ovarian hormone production
LH and FSH act on the ovaries. FSH supports follicular development and estrogen synthesis, while LH supports ovulation and corpus luteum function. Together, these hormones regulate ovarian production of estradiol and progesterone.
Step 4: Estrogen supports endometriosis lesion activity
Endometriosis is strongly estrogen-dependent. Estradiol promotes survival, proliferation, inflammation, and vascular support of ectopic endometrial-like implants. Higher estrogenic stimulation can worsen pelvic pain, dysmenorrhea, and lesion-related inflammation.
Step 5: Orilissa competitively blocks GnRH receptors
Elagolix competes with endogenous GnRH for GnRH receptor binding in the pituitary gland. By occupying these receptors, it blocks normal GnRH signaling. This is the central molecular action of Orilissa.
Step 6: LH and FSH secretion decrease
When pituitary GnRH receptors are blocked, gonadotroph cells release less LH and FSH. This occurs without the initial gonadotropin flare seen with GnRH agonists. This is an important exam point.
Step 7: Ovarian estradiol and progesterone levels decrease
Reduced LH and FSH stimulation leads to lower ovarian production of estradiol and progesterone. The suppression is dose-dependent. The 200 mg twice-daily regimen produces stronger estrogen suppression than the 150 mg once-daily regimen.
Step 8: Endometriosis implants receive less hormonal stimulation
With lower estradiol levels, ectopic endometrial tissue receives less proliferative and inflammatory support. This reduces lesion activity and decreases local inflammatory mediator production.
Step 9: Prostaglandin-mediated pain signaling decreases
Endometriosis lesions and surrounding inflammatory tissue can produce prostaglandins and cytokines that sensitize pelvic nerves. By reducing estrogen-driven lesion activity and inflammation, Orilissa indirectly reduces pain signaling.
Step 10: Dysmenorrhea and pelvic pain improve
The final therapeutic effect is reduction in endometriosis-associated pain, especially dysmenorrhea and non-menstrual pelvic pain. Higher-dose therapy may be considered when dyspareunia is a major symptom, but duration must be limited because of bone mineral density loss.
Step 11: Suppression is reversible after discontinuation
Because elagolix is a receptor antagonist rather than a depot agonist, its effects are generally reversible after the drug is stopped. Ovarian hormone production and menstrual cycles may return after discontinuation, although the timing varies among patients.
Step 12: Orilissa does not cure endometriosis
Orilissa reduces hormonal stimulation and pain symptoms, but it does not permanently remove endometriotic lesions. Symptoms may return after treatment is stopped, and long-term management may require medical, surgical, fertility-focused, or multidisciplinary care depending on the patient.
Pharmacokinetics
Orilissa is administered orally as tablets. The available tablet strengths are 150 mg and 200 mg. It may be taken with or without food, usually at approximately the same time each day.
The usual recommended dosing options are 150 mg once daily for up to 24 months or 200 mg twice daily for up to 6 months. The higher dose provides greater hormonal suppression but is associated with greater hypoestrogenic adverse effects, especially bone mineral density loss. In moderate hepatic impairment, the recommended dose is 150 mg once daily for up to 6 months, and the 200 mg twice-daily dose is not recommended.
Elagolix is rapidly absorbed after oral administration. Peak plasma concentrations are reached within about 1 hour. Food may reduce peak concentration but does not produce a clinically meaningful reduction in overall exposure, so it can be taken without regard to meals.
Elagolix is moderately protein bound and distributes systemically. It is metabolized by multiple pathways, including CYP3A metabolism, and is also affected by hepatic uptake transporters such as OATP1B1. Because of this, drug interactions are clinically important.
Strong OATP1B1 inhibitors that significantly increase elagolix exposure, such as cyclosporine and gemfibrozil, are contraindicated. Strong CYP3A inducers may reduce elagolix exposure and decrease effectiveness, while strong CYP3A inhibitors can increase exposure and may require caution depending on dose and duration.
Elagolix can also affect other drugs. It may reduce exposure to some medications metabolized by CYP3A and may increase exposure to others depending on transporter or enzyme effects. Hormonal contraceptive interactions are especially important because estrogen-containing contraceptives may reduce Orilissa efficacy, and progestin-containing contraceptives may have reduced contraceptive effectiveness.
No dose adjustment is required for renal impairment, including end-stage renal disease, but severe hepatic impairment is contraindicated because elagolix exposure increases significantly.
Clinical Uses
Orilissa is used for the management of moderate to severe pain associated with endometriosis in premenopausal adults. It is used to reduce pain symptoms rather than to cure the disease.
The major endometriosis-associated pain symptoms targeted by Orilissa include dysmenorrhea, non-menstrual pelvic pain, and dyspareunia. Dysmenorrhea refers to painful menstruation. Non-menstrual pelvic pain refers to chronic pelvic pain that occurs outside the menstrual period. Dyspareunia means pain during sexual intercourse.
The 150 mg once-daily regimen is commonly used when long-term symptom control is needed and bone safety is a concern. The 200 mg twice-daily regimen may be considered for more severe symptoms, especially dyspareunia, but it is limited to shorter treatment duration.
Orilissa is not a contraceptive. Patients of reproductive potential should use effective non-hormonal contraception during therapy and for 28 days after discontinuation. Pregnancy should be excluded before starting therapy, and the drug should be discontinued if pregnancy occurs.
Orilissa is not approved for infertility treatment, uterine fibroid bleeding, polycystic ovarian syndrome, adenomyosis alone, menopausal symptoms, or pediatric endometriosis. Elagolix is included in other products for uterine fibroid-related heavy menstrual bleeding, but Orilissa itself is specifically indicated for endometriosis-associated pain.
Adverse Effects
The most important adverse effect of Orilissa is dose- and duration-dependent bone mineral density loss. Lower estrogen levels reduce bone protection and can lead to decreased bone density. Bone loss may not be completely reversible after stopping therapy, so duration limits are important. Patients with known osteoporosis should not use Orilissa.
Hypoestrogenic adverse effects are common. These include hot flushes, night sweats, headache, insomnia, mood changes, vaginal dryness, decreased libido, and menstrual changes. Amenorrhea or reduced menstrual bleeding can occur because ovarian hormone levels are suppressed.
Reduced menstrual bleeding may make pregnancy harder to recognize. This is clinically important because Orilissa is contraindicated during pregnancy and may increase the risk of early pregnancy loss. Pregnancy testing should be performed if pregnancy is suspected.
Mood-related adverse effects are important. Depression, anxiety, mood changes, suicidal ideation, and suicidal behavior have been reported. Patients with a history of depression or mood disorder should be monitored carefully, and urgent medical attention is needed for suicidal thoughts or severe mood worsening.
Hepatic transaminase elevations can occur in a dose-dependent manner. Patients should be counseled to report symptoms of liver injury such as jaundice, dark urine, severe fatigue, nausea, vomiting, right upper abdominal pain, or unexplained itching.
Common adverse effects include hot flushes, night sweats, headache, nausea, insomnia, amenorrhea, anxiety, arthralgia, depression-related reactions, mood changes, and decreased menstrual bleeding.
Other possible adverse effects include decreased libido, vaginal dryness, irritability, dizziness, diarrhea, constipation, abdominal pain, fatigue, weight changes, and hypersensitivity reactions such as rash, angioedema, or anaphylaxis.
Important contraindications include pregnancy, known osteoporosis, severe hepatic impairment, use with strong OATP1B1 inhibitors expected to significantly increase elagolix concentrations, and known hypersensitivity to elagolix or product components.
Comparative Analysis
Orilissa is commonly compared with GnRH agonists, combined oral contraceptives, progestins, danazol, NSAIDs, and surgical management for endometriosis.
Compared with GnRH agonists such as leuprolide, Orilissa is a GnRH receptor antagonist. GnRH agonists initially stimulate receptors and cause a temporary flare of LH and FSH before downregulation occurs. Orilissa directly blocks receptors and suppresses gonadotropins without an initial flare.
Compared with combined oral contraceptives, Orilissa does not provide contraception and does not contain estrogen or progestin. Combined oral contraceptives suppress ovulation and stabilize endometrial tissue, while Orilissa reduces ovarian hormone production through pituitary GnRH receptor blockade.
Compared with progestins such as norethindrone acetate, medroxyprogesterone acetate, or dienogest, Orilissa works upstream at the pituitary gland. Progestins directly oppose estrogen effects on endometrial tissue and may cause decidualization and atrophy of endometriotic implants.
Compared with danazol, Orilissa has a more targeted hypothalamic-pituitary-gonadal axis mechanism and avoids many androgenic adverse effects. Danazol suppresses gonadotropins but can cause acne, hirsutism, voice deepening, lipid changes, and other androgenic effects.
Compared with NSAIDs, Orilissa targets the hormonal driver of endometriosis pain. NSAIDs reduce prostaglandin synthesis and may help dysmenorrhea, but they do not suppress ovarian estrogen production or directly reduce endometriosis lesion activity.
Compared with surgery, Orilissa is a medical therapy. Surgery can remove or ablate visible endometriotic lesions and treat adhesions or endometriomas, but recurrence is possible. Orilissa can reduce symptoms medically, but it does not physically remove lesions.
Compared with relugolix combination therapy used for some gynecologic indications, Orilissa is elagolix alone and does not include built-in estrogen/progestin add-back therapy. This is relevant because hypoestrogenic effects and bone loss are central limitations of Orilissa therapy.
MCQs
- Orilissa contains which active drug?
a) Relugolix
b) Elagolix
c) Leuprolide
d) Danazol
Answer: b) Elagolix
- Elagolix belongs to which pharmacological class?
a) GnRH receptor antagonist
b) GnRH receptor agonist
c) Aromatase inhibitor
d) Selective estrogen receptor modulator
Answer: a) GnRH receptor antagonist
- Orilissa is mainly used for:
a) Moderate to severe pain associated with endometriosis
b) Acute bacterial pelvic infection
c) Ovarian cancer chemotherapy
d) Emergency contraception
Answer: a) Moderate to severe pain associated with endometriosis
- Elagolix acts primarily at which site?
a) Pituitary GnRH receptors
b) Uterine beta receptors
c) Ovarian estrogen receptors only
d) Dopamine D2 receptors
Answer: a) Pituitary GnRH receptors
- Blocking pituitary GnRH receptors reduces secretion of:
a) LH and FSH
b) Insulin and glucagon
c) TSH and prolactin only
d) Cortisol and aldosterone
Answer: a) LH and FSH
- Reduced LH and FSH with Orilissa leads to decreased:
a) Ovarian estradiol and progesterone
b) Gastric acid secretion
c) Dopamine release
d) Platelet aggregation
Answer: a) Ovarian estradiol and progesterone
- Which statement best differentiates elagolix from leuprolide?
a) Elagolix is a GnRH antagonist without initial flare, while leuprolide is a GnRH agonist with initial flare
b) Elagolix is an antibiotic, while leuprolide is an antifungal
c) Elagolix stimulates estrogen production, while leuprolide blocks calcium channels
d) Both are NSAIDs
Answer: a) Elagolix is a GnRH antagonist without initial flare, while leuprolide is a GnRH agonist with initial flare
- The most important dose- and duration-related adverse effect of Orilissa is:
a) Bone mineral density loss
b) Severe hypoglycemia
c) Ototoxicity
d) Gingival hyperplasia
Answer: a) Bone mineral density loss
- Which condition is a contraindication to Orilissa?
a) Known osteoporosis
b) Mild seasonal allergy
c) Controlled acne
d) Mild headache
Answer: a) Known osteoporosis
- Orilissa is contraindicated during pregnancy because it may:
a) Increase the risk of early pregnancy loss
b) Improve fetal bone density
c) Treat morning sickness
d) Act as prenatal vitamin therapy
Answer: a) Increase the risk of early pregnancy loss
- Which contraception advice is correct for Orilissa?
a) Use effective non-hormonal contraception during treatment and for 28 days after stopping
b) Orilissa is a reliable contraceptive pill
c) No contraception is needed because ovulation is impossible in all patients
d) Use only estrogen-containing contraceptives to improve efficacy
Answer: a) Use effective non-hormonal contraception during treatment and for 28 days after stopping
- Which adverse effect is common with Orilissa due to estrogen suppression?
a) Hot flushes
b) Severe hypertension in all patients
c) Permanent hearing loss
d) Hypoglycemic coma
Answer: a) Hot flushes
- Which liver-related adverse effect may occur with Orilissa?
a) Hepatic transaminase elevation
b) Mandatory liver failure after one dose
c) Complete protection from hepatitis
d) Increased bile acid synthesis only
Answer: a) Hepatic transaminase elevation
- Which drug class can significantly increase elagolix exposure through OATP1B1 inhibition and is contraindicated?
a) Strong OATP1B1 inhibitors
b) Inhaled beta-2 agonists
c) Topical antifungals
d) Oral calcium supplements
Answer: a) Strong OATP1B1 inhibitors
- Which statement best describes Orilissa?
a) It competitively blocks pituitary GnRH receptors and lowers LH, FSH, estradiol, and progesterone
b) It directly blocks dopamine receptors in the brain
c) It inhibits bacterial DNA gyrase
d) It stimulates estrogen receptors in endometriosis lesions
Answer: a) It competitively blocks pituitary GnRH receptors and lowers LH, FSH, estradiol, and progesterone
FAQs
What is the mechanism of action of Orilissa?
Orilissa, or elagolix, competitively blocks GnRH receptors in the pituitary gland. This reduces LH and FSH secretion, lowers ovarian estradiol and progesterone production, and decreases estrogen-driven stimulation of endometriosis lesions.
What is the generic name of Orilissa?
The generic name of Orilissa is elagolix.
Is Orilissa a GnRH agonist or antagonist?
Orilissa is a GnRH receptor antagonist. It directly blocks GnRH receptors and does not cause the initial hormone flare seen with GnRH agonists such as leuprolide.
What is Orilissa used for?
Orilissa is used for the management of moderate to severe pain associated with endometriosis in premenopausal adults. It helps reduce symptoms such as dysmenorrhea, non-menstrual pelvic pain, and dyspareunia.
Does Orilissa cure endometriosis?
No. Orilissa does not cure endometriosis or permanently remove lesions. It reduces ovarian hormone stimulation and helps control pain while the patient is taking treatment.
Why is Orilissa treatment duration limited?
Treatment duration is limited because Orilissa causes dose- and duration-dependent bone mineral density loss. Bone loss may not be completely reversible after stopping therapy.
Can Orilissa be used as contraception?
No. Orilissa is not a contraceptive. Effective non-hormonal contraception should be used during treatment and for 28 days after stopping the drug.
What are the common adverse effects of Orilissa?
Common adverse effects include hot flushes, night sweats, headache, nausea, insomnia, amenorrhea, anxiety, mood changes, arthralgia, and depression-related symptoms.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

