
Table of Contents
Introduction
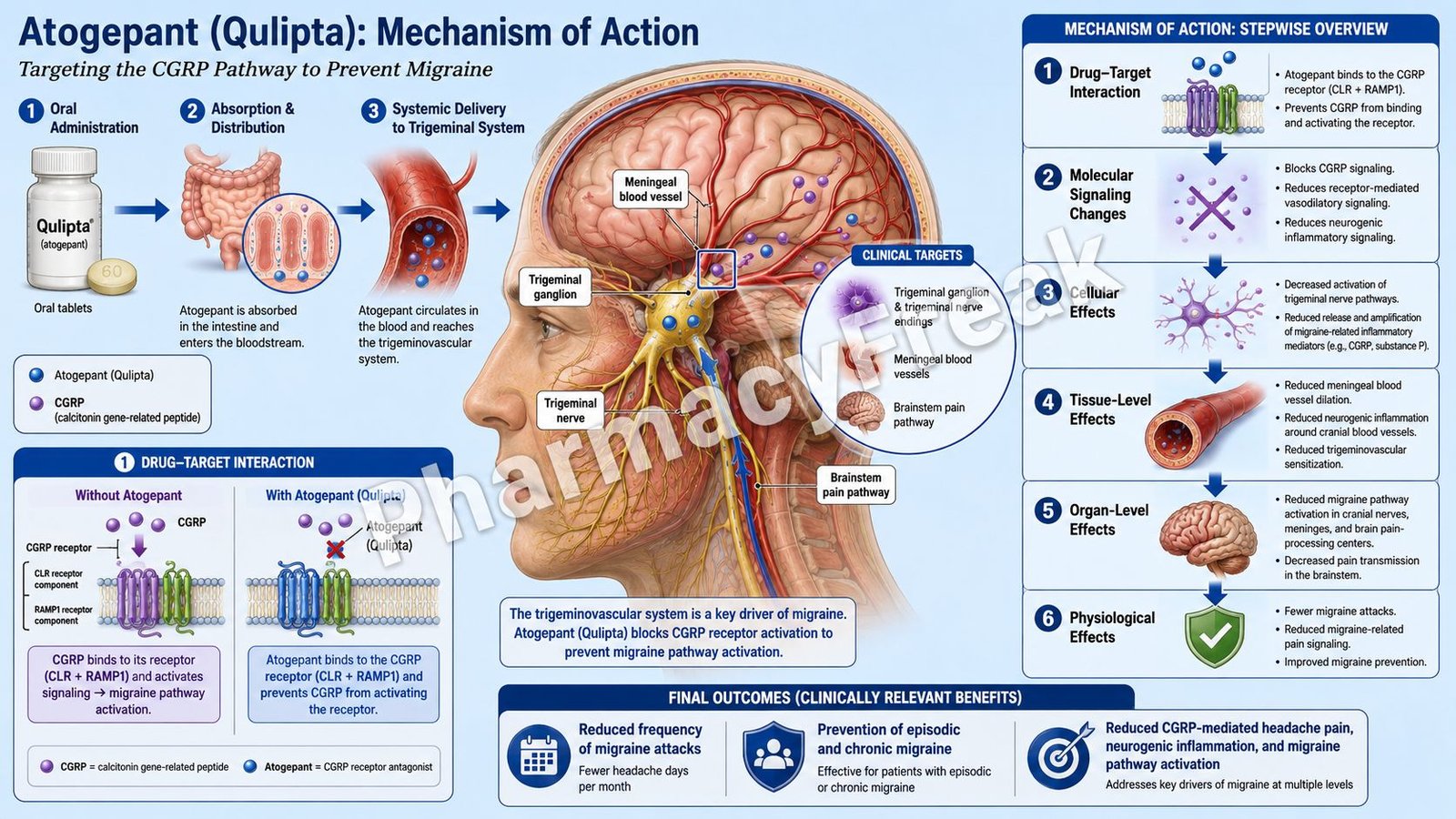
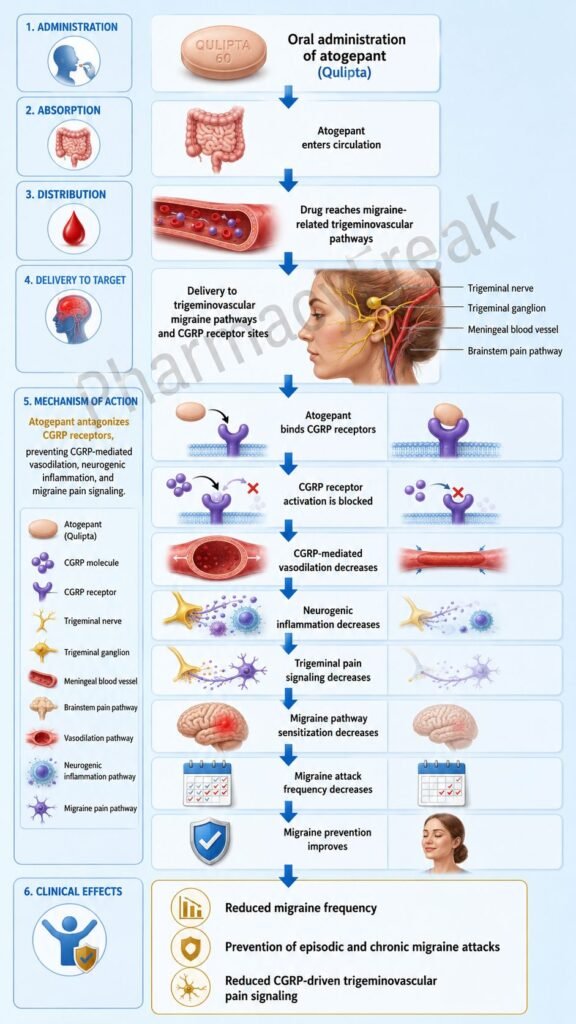
Atogepant is an oral migraine-preventive drug that belongs to the calcitonin gene-related peptide receptor antagonist class. Drugs in this class are commonly called gepants. Atogepant is marketed under the brand name Qulipta in the United States and Aquipta in some other regions.
Atogepant is used for the preventive treatment of migraine in adults. It is important to understand that atogepant is not primarily an acute painkiller like NSAIDs, triptans, or ergot derivatives. Instead, it is taken regularly to reduce the frequency of migraine attacks by blocking a key migraine pathway involving calcitonin gene-related peptide, commonly known as CGRP.
CGRP is a neuropeptide released from trigeminal sensory nerves during migraine attacks. It plays a major role in trigeminovascular activation, cranial vasodilation, neurogenic inflammation, and pain transmission. By blocking CGRP receptors, atogepant reduces migraine-related neuronal and vascular signaling without causing direct vasoconstriction. This makes it pharmacologically different from triptans, which act mainly as 5-HT1B/1D receptor agonists and can produce cranial vasoconstriction.
For exam purposes, atogepant should be remembered as an oral, once-daily, small-molecule CGRP receptor antagonist used for migraine prevention in adults.
Mechanism of Action (Step-wise)
Step 1: Migraine involves activation of the trigeminovascular system
During a migraine attack, trigeminal sensory nerves supplying the meninges and cranial blood vessels become activated. These nerves release neuropeptides, especially CGRP, into the trigeminovascular system.
Step 2: CGRP is released from trigeminal nerve endings
CGRP is one of the most important mediators in migraine pathophysiology. It is released from peripheral and central terminals of trigeminal neurons. During migraine, CGRP levels may rise and contribute to pain signaling, vasodilation, and sensitization of trigeminal pathways.
Step 3: CGRP binds to CGRP receptors
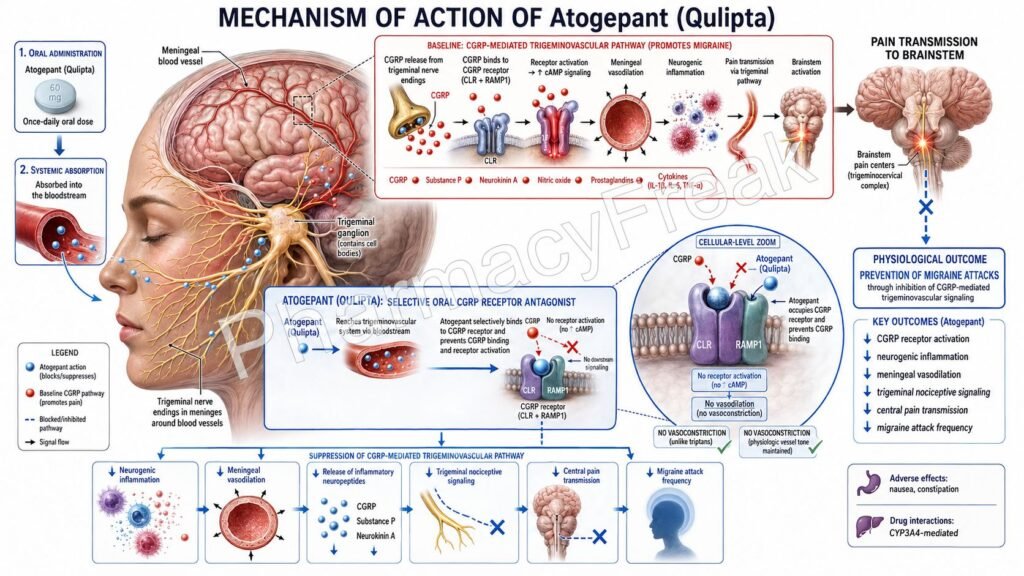
The CGRP receptor is a G protein-coupled receptor complex. It mainly consists of calcitonin receptor-like receptor, also called CLR, and receptor activity-modifying protein 1, called RAMP1. These receptors are found in areas relevant to migraine, including trigeminal ganglia, cranial blood vessels, and pain-processing pathways.
Step 4: CGRP receptor activation increases cAMP signaling
When CGRP binds to its receptor, it activates Gs protein signaling. This stimulates adenylyl cyclase and increases intracellular cyclic AMP. Increased cAMP contributes to relaxation of vascular smooth muscle, vasodilation, and enhanced pain signaling.
Step 5: CGRP promotes cranial vasodilation
CGRP is a potent vasodilator. In migraine, CGRP-mediated vasodilation of cranial and meningeal blood vessels is believed to contribute to headache generation and maintenance. Although migraine is not simply a vascular disease, trigeminovascular signaling is a central part of migraine biology.
Step 6: CGRP contributes to neurogenic inflammation
CGRP also promotes neurogenic inflammation around meningeal tissues. This can increase inflammatory mediator release, vascular permeability, and sensitization of pain fibers. These effects make trigeminal neurons more responsive to painful stimuli.
Step 7: CGRP supports peripheral and central sensitization
Repeated or sustained trigeminal activation can lead to sensitization. Peripheral sensitization increases the excitability of trigeminal nerve endings, while central sensitization increases pain processing in the brainstem and higher centers. This can worsen migraine symptoms and contribute to allodynia, where normally non-painful stimuli become painful.
Step 8: Atogepant blocks the CGRP receptor
Atogepant acts as a selective antagonist of the CGRP receptor. It binds to the receptor and prevents CGRP from activating it. This blocks CGRP-mediated downstream signaling without directly activating the receptor.
Step 9: cAMP-mediated migraine signaling is reduced
By blocking CGRP receptor activation, atogepant reduces CGRP-induced cAMP signaling. This helps reduce vasodilatory and nociceptive signaling associated with migraine pathophysiology.
Step 10: Trigeminovascular activation decreases
With CGRP receptor signaling blocked, the trigeminovascular system becomes less prone to migraine-related activation. This reduces the biological tendency for recurrent migraine attacks.
Step 11: Migraine attack frequency is reduced
The final therapeutic outcome is prevention of migraine attacks. Atogepant reduces monthly migraine days in appropriate adult patients with episodic or chronic migraine. It does not cure migraine, but it reduces the likelihood and frequency of migraine attacks.
Step 12: Atogepant does not cause direct vasoconstriction
A clinically important point is that atogepant blocks CGRP signaling rather than constricting blood vessels. This distinguishes it from triptans and ergot alkaloids. Atogepant is used for prevention, while triptans are mainly used for acute migraine treatment.
Pharmacokinetics
Atogepant is given orally as a tablet and is usually administered once daily. It may be taken with or without food. This oral once-daily dosing is one of its major practical advantages compared with injectable CGRP monoclonal antibodies.
After oral administration, atogepant is absorbed relatively quickly. Peak plasma concentrations are reached in about 1 to 2 hours. It shows dose-proportional pharmacokinetics over the clinically relevant dose range and does not show significant accumulation with regular dosing.
Atogepant is highly protein bound in plasma. It has a relatively large apparent volume of distribution, indicating distribution beyond the central plasma compartment.
Atogepant is metabolized mainly by CYP3A4. This makes drug interactions clinically important. Strong CYP3A4 inhibitors can increase atogepant exposure and may require dose reduction. Examples include itraconazole, ketoconazole, clarithromycin, and some antiviral protease inhibitors. CYP3A4 inducers such as rifampin, carbamazepine, phenytoin, and St. John’s wort may reduce atogepant exposure and decrease efficacy.
Atogepant is also a substrate of transporters such as OATP1B1 and OATP1B3. OATP inhibitors can increase atogepant exposure and may require dose adjustment.
The elimination half-life of atogepant is approximately 11 hours, supporting once-daily dosing. Renal elimination plays a minor role compared with metabolism, but dose recommendations change in severe renal impairment. In severe renal impairment or end-stage renal disease, atogepant use depends on whether the patient is being treated for episodic or chronic migraine. For chronic migraine, use in severe renal impairment or end-stage renal disease is generally not recommended.
Atogepant should generally be avoided in severe hepatic impairment because drug exposure and liver-related safety concerns may increase.
Clinical Uses
Atogepant is approved for the preventive treatment of migraine in adults. It is used to reduce the number of migraine days and improve migraine control over time.
Atogepant is used in episodic migraine prevention. Episodic migraine generally refers to migraine occurring on fewer than 15 headache days per month. In this setting, atogepant may be used as a daily preventive option for patients who require prophylactic therapy.
Atogepant is also used in chronic migraine prevention. Chronic migraine generally refers to headache occurring on 15 or more days per month for more than 3 months, with migraine features on a significant number of those days. For chronic migraine, atogepant is used to reduce monthly migraine days and improve disease burden.
Atogepant is especially useful for patients who need migraine prevention but may not tolerate or prefer traditional preventive drugs such as topiramate, beta-blockers, tricyclic antidepressants, valproate, or injectable CGRP monoclonal antibodies.
It is not used for immediate relief of an ongoing migraine attack. Other drugs, such as NSAIDs, acetaminophen, triptans, lasmiditan, or acute-use gepants like ubrogepant and rimegepant, may be used for acute migraine treatment depending on the patient.
Adverse Effects
The most common adverse effects of atogepant are nausea, constipation, and fatigue or somnolence. These are generally mild to moderate but may affect adherence in some patients.
Constipation is an exam-relevant adverse effect because CGRP has physiological roles in the gastrointestinal tract. Inhibition of CGRP signaling may contribute to reduced gastrointestinal motility in some patients.
Atogepant may also cause decreased appetite and dizziness. Some patients may experience weight loss, although this is not the primary purpose of the drug.
Hypersensitivity reactions can occur. Reported reactions include rash, pruritus, urticaria, facial edema, dyspnea, and rarely anaphylaxis. A clinically important point is that hypersensitivity reactions may occur days after administration. If a serious hypersensitivity reaction occurs, atogepant should be discontinued and appropriate treatment should be given.
New-onset hypertension or worsening of pre-existing hypertension has been reported with CGRP antagonists, including atogepant. Blood pressure monitoring is important, especially in patients with cardiovascular risk factors or known hypertension.
Raynaud’s phenomenon may occur or worsen during treatment with CGRP antagonists. Patients with a history of Raynaud’s phenomenon should be monitored for worsening digital color changes, numbness, pain, or cold sensitivity.
Liver enzyme elevations can occur, although clinically significant hepatotoxicity is not common with atogepant at approved doses. Patients with severe hepatic impairment should generally avoid atogepant.
Pregnancy safety data in humans are limited. Based on animal data, fetal harm is possible. Atogepant should be used during pregnancy only when clearly needed and under specialist guidance. Safety and effectiveness in pediatric patients have not been established.
Comparative Analysis
Atogepant is part of the gepant class, which includes ubrogepant, rimegepant, and zavegepant. Gepants block CGRP receptor signaling, but their clinical roles differ.
Atogepant is mainly used as a preventive migraine drug. Ubrogepant is used for acute treatment of migraine attacks. Rimegepant can be used for acute treatment and also for prevention in some settings. Zavegepant is an intranasal CGRP receptor antagonist used for acute migraine treatment.
Compared with triptans, atogepant does not act through serotonin 5-HT1B/1D receptors and does not produce direct vasoconstriction. Triptans are primarily acute migraine drugs, while atogepant is a preventive drug. This difference is very important for exams.
Compared with ergot alkaloids such as ergotamine and dihydroergotamine, atogepant has a more selective CGRP receptor-based mechanism. Ergot drugs act on multiple serotonin, dopamine, and adrenergic receptors and have more vasoconstrictive adverse effects.
Compared with CGRP monoclonal antibodies such as erenumab, fremanezumab, galcanezumab, and eptinezumab, atogepant is a small-molecule oral drug. Monoclonal antibodies are usually given by subcutaneous or intravenous routes and have long half-lives. Atogepant has a shorter half-life and daily oral dosing.
Compared with topiramate, atogepant has a more migraine-specific mechanism. Topiramate has multiple mechanisms, including effects on voltage-gated sodium channels, GABA activity, glutamate receptors, and carbonic anhydrase. Topiramate may cause cognitive slowing, paresthesia, weight loss, kidney stones, and teratogenic risk. Atogepant mainly targets the CGRP pathway.
Compared with beta-blockers such as propranolol and metoprolol, atogepant does not reduce migraine by blocking adrenergic receptors. Beta-blockers are useful traditional preventive drugs but may be unsuitable in asthma, bradycardia, or certain cardiac conduction disorders. Atogepant offers a non-beta-blocker preventive option.
MCQs
- Atogepant belongs to which pharmacological class?
a) CGRP receptor antagonist
b) Beta-blocker
c) Triptan
d) Ergot alkaloid
Answer: a) CGRP receptor antagonist
- Qulipta contains which active drug?
a) Ubrogepant
b) Atogepant
c) Sumatriptan
d) Topiramate
Answer: b) Atogepant
- Atogepant is mainly used for:
a) Immediate relief of acute myocardial infarction
b) Preventive treatment of migraine in adults
c) Treatment of bacterial meningitis
d) Reversal of opioid overdose
Answer: b) Preventive treatment of migraine in adults
- CGRP stands for:
a) Central glucose regulatory protein
b) Calcitonin gene-related peptide
c) Calcium gated receptor peptide
d) Cortical glutamate release protein
Answer: b) Calcitonin gene-related peptide
- Atogepant prevents migraine mainly by blocking:
a) Dopamine D2 receptors
b) Muscarinic M3 receptors
c) CGRP receptors
d) Histamine H1 receptors
Answer: c) CGRP receptors
- The CGRP receptor is mainly associated with which receptor components?
a) CLR and RAMP1
b) GABA-A and NMDA
c) COX-1 and COX-2
d) ACE and AT1
Answer: a) CLR and RAMP1
- Activation of CGRP receptors commonly increases which intracellular second messenger?
a) cAMP
b) cGMP only
c) IP3 only
d) Calcium carbonate
Answer: a) cAMP
- Which statement about atogepant is correct?
a) It directly constricts cranial arteries like triptans
b) It blocks CGRP receptor signaling without direct vasoconstriction
c) It is an irreversible opioid receptor antagonist
d) It inhibits cyclooxygenase irreversibly
Answer: b) It blocks CGRP receptor signaling without direct vasoconstriction
- Which adverse effect is commonly associated with atogepant?
a) Constipation
b) Severe hypoglycemia
c) Ototoxicity
d) Gingival hyperplasia
Answer: a) Constipation
- Atogepant is metabolized mainly by:
a) CYP3A4
b) CYP2C19 only
c) Monoamine oxidase
d) Acetylcholinesterase
Answer: a) CYP3A4
- Which drug interaction may increase atogepant exposure?
a) Strong CYP3A4 inhibitor
b) Penicillin V
c) Oral iron supplement
d) Inhaled salbutamol
Answer: a) Strong CYP3A4 inhibitor
- Which warning is associated with CGRP antagonists such as atogepant?
a) New-onset or worsening hypertension
b) Irreversible hearing loss in all patients
c) Mandatory neutropenia
d) Severe insulin overdose
Answer: a) New-onset or worsening hypertension
- Which condition may newly occur or worsen with atogepant therapy?
a) Raynaud’s phenomenon
b) Cataract formation within 24 hours
c) Acute appendicitis
d) Hyperthyroidism
Answer: a) Raynaud’s phenomenon
- Which drug is most appropriately compared with atogepant as another gepant?
a) Ubrogepant
b) Warfarin
c) Propranolol
d) Amitriptyline
Answer: a) Ubrogepant
- Which statement best differentiates atogepant from sumatriptan?
a) Atogepant is a preventive CGRP receptor antagonist, while sumatriptan is an acute 5-HT1B/1D agonist
b) Atogepant is an antibiotic, while sumatriptan is an antifungal
c) Both are irreversible COX inhibitors
d) Sumatriptan is used only for migraine prevention and never for acute attacks
Answer: a) Atogepant is a preventive CGRP receptor antagonist, while sumatriptan is an acute 5-HT1B/1D agonist
FAQs
What is the mechanism of action of atogepant?
Atogepant is a CGRP receptor antagonist. It blocks CGRP from activating its receptor in the trigeminovascular system, reducing migraine-related vasodilation, neurogenic inflammation, and pain pathway sensitization.
Is atogepant used for acute migraine attacks?
Atogepant is mainly used for preventive treatment of migraine in adults. It is taken regularly to reduce migraine frequency, not as the primary drug for immediate relief of an ongoing attack.
What is the brand name of atogepant?
Atogepant is sold as Qulipta in the United States and as Aquipta in some other regions.
Does atogepant cause vasoconstriction?
No. Atogepant blocks CGRP receptor signaling and does not directly cause vasoconstriction. This makes it different from triptans and ergot derivatives.
What are the common adverse effects of atogepant?
The common adverse effects include nausea, constipation, fatigue, somnolence, decreased appetite, and dizziness.
Which enzyme metabolizes atogepant?
Atogepant is metabolized mainly by CYP3A4. Strong CYP3A4 inhibitors can increase atogepant exposure, while CYP3A4 inducers can reduce its effectiveness.
Can atogepant worsen blood pressure?
Yes. New-onset hypertension or worsening of pre-existing hypertension has been reported with CGRP antagonists, including atogepant. Blood pressure monitoring may be needed.
How is atogepant different from CGRP monoclonal antibodies?
Atogepant is an oral small-molecule CGRP receptor antagonist taken daily. CGRP monoclonal antibodies are injectable or intravenous biologic drugs with much longer half-lives.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology

