
Table of Contents
Introduction
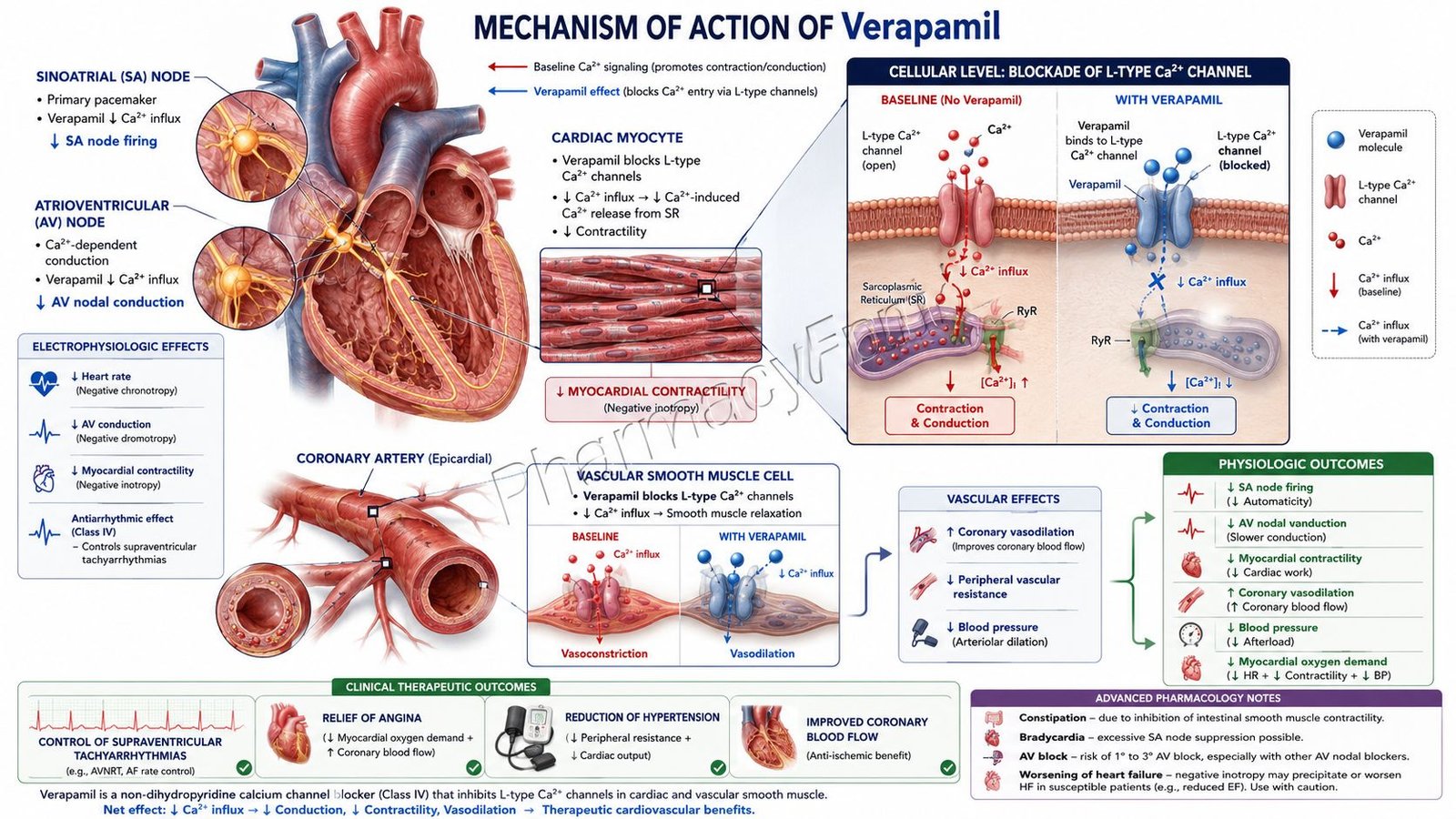
Verapamil is a non-dihydropyridine calcium channel blocker (CCB) that is widely used in the treatment of hypertension, angina pectoris, and supraventricular arrhythmias. Unlike dihydropyridine calcium channel blockers that primarily act on vascular smooth muscle, verapamil exerts significant effects on both cardiac muscle and the cardiac conduction system.
By inhibiting L-type calcium channels in the heart and blood vessels, verapamil reduces myocardial contractility, slows atrioventricular (AV) nodal conduction, decreases heart rate, and produces vasodilation. These combined actions make it particularly useful in conditions where control of heart rate and myocardial oxygen demand is required.
Mechanism of Action (Step-wise)
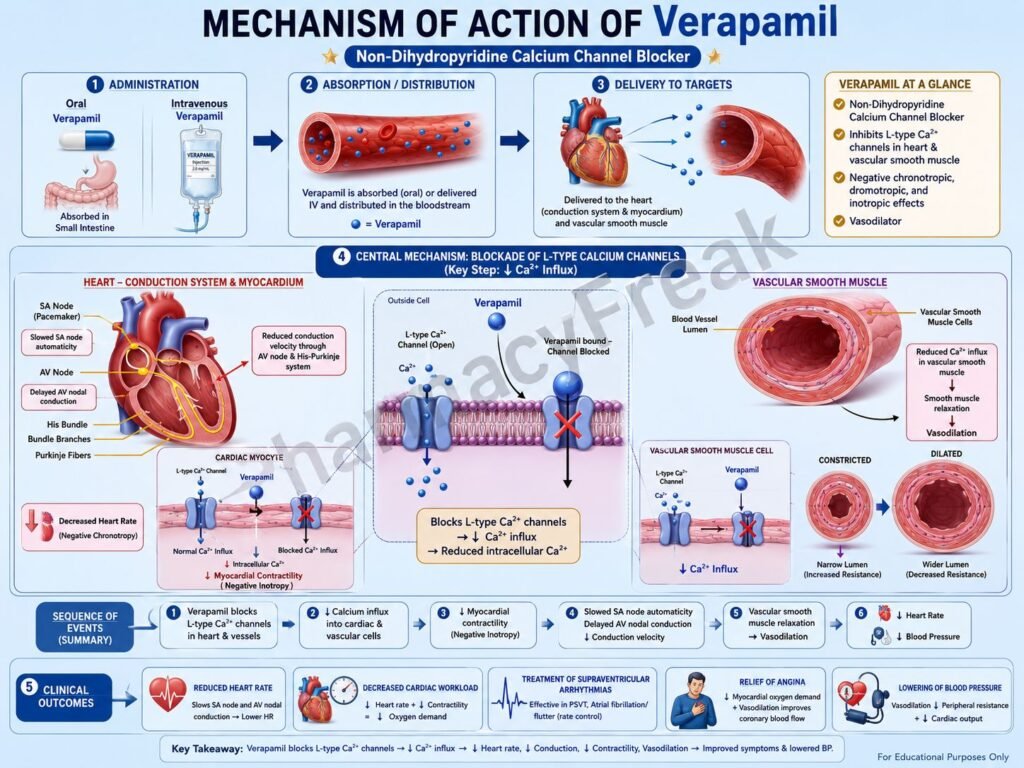
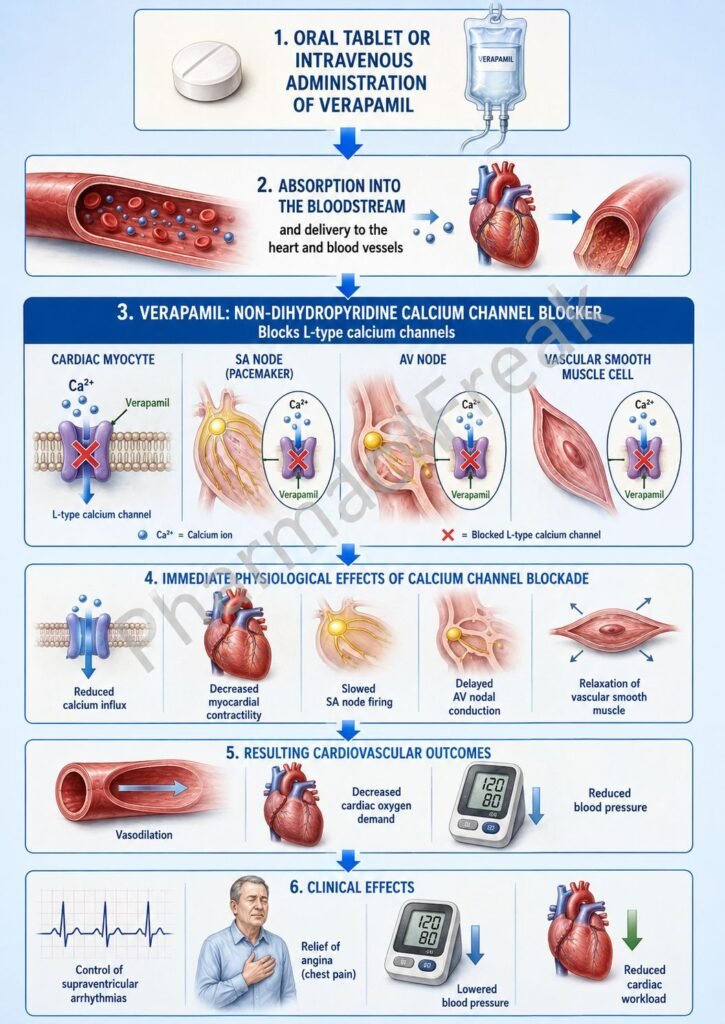
Verapamil acts primarily by blocking voltage-gated L-type calcium channels in cardiac tissue and vascular smooth muscle.
1. Oral Administration and Systemic Distribution
Following oral or intravenous administration, verapamil enters systemic circulation and is distributed to the heart, blood vessels, and cardiac conduction system.
Its primary targets are:
- Cardiac myocytes
- Sinoatrial (SA) node
- Atrioventricular (AV) node
- Vascular smooth muscle cells
2. Blockade of L-Type Calcium Channels
During normal depolarization, L-type calcium channels allow calcium ions to enter cells.
Verapamil binds to and blocks these channels, reducing calcium influx into:
- Cardiac muscle cells
- SA nodal cells
- AV nodal cells
- Vascular smooth muscle cells
Reduced intracellular calcium decreases calcium-dependent cellular activity.
3. Reduction in Myocardial Contractility (Negative Inotropic Effect)
Calcium is essential for excitation-contraction coupling in cardiac muscle.
By reducing calcium entry into myocardial cells, verapamil decreases the interaction between actin and myosin filaments.
This leads to:
- Reduced force of cardiac contraction
- Decreased myocardial oxygen consumption
- Reduced cardiac workload
This effect contributes to its antianginal action.
4. Slowing of SA Node Automaticity (Negative Chronotropic Effect)
The SA node is the primary pacemaker of the heart.
Calcium influx contributes to pacemaker activity.
Verapamil reduces calcium entry into SA nodal cells, causing:
- Reduced spontaneous depolarization
- Decreased heart rate
- Slower impulse generation
This negative chronotropic effect is useful in tachyarrhythmias.
5. Slowing of AV Nodal Conduction (Negative Dromotropic Effect)
AV nodal conduction depends heavily on calcium influx.
Verapamil suppresses calcium entry into AV nodal cells, resulting in:
- Slower AV nodal conduction
- Increased AV nodal refractory period
- Reduced transmission of rapid atrial impulses to ventricles
This mechanism makes verapamil particularly effective in supraventricular tachycardias and atrial fibrillation with rapid ventricular response.
6. Relaxation of Vascular Smooth Muscle
Calcium is required for vascular smooth muscle contraction.
Blockade of calcium channels reduces intracellular calcium concentrations, resulting in:
- Smooth muscle relaxation
- Arterial vasodilation
- Reduced peripheral vascular resistance
- Lower blood pressure
The vasodilatory effect contributes to its antihypertensive activity.
7. Improvement in Coronary Blood Flow
Coronary arteries also undergo vasodilation following calcium channel blockade.
This results in:
- Increased coronary blood flow
- Improved oxygen delivery to myocardium
- Relief of coronary vasospasm
8. Final Therapeutic Effects
The combined actions of verapamil produce:
- Reduced heart rate
- Reduced myocardial contractility
- Slower AV nodal conduction
- Lower blood pressure
- Improved coronary perfusion
- Reduced myocardial oxygen demand
These effects explain its usefulness in hypertension, angina, and supraventricular arrhythmias.
Pharmacokinetics
Verapamil is well absorbed following oral administration.
- Oral bioavailability is approximately 20–35% due to significant first-pass hepatic metabolism.
- Peak plasma concentrations occur within 1–2 hours for immediate-release formulations.
- Extended-release formulations provide prolonged therapeutic effects.
- Verapamil is highly protein bound.
- It undergoes extensive hepatic metabolism.
- CYP3A4 is the primary enzyme involved in metabolism.
- The major active metabolite is norverapamil.
- Elimination occurs mainly through renal excretion of metabolites.
- The elimination half-life ranges from approximately 3–7 hours but may increase with repeated dosing.
Clinical Uses
Hypertension
Verapamil lowers blood pressure by reducing peripheral vascular resistance and cardiac workload.
Chronic Stable Angina
Reduction of myocardial oxygen demand improves symptoms of angina.
Vasospastic (Prinzmetal) Angina
Coronary vasodilation helps relieve coronary artery spasm.
Supraventricular Tachycardia (SVT)
Verapamil slows AV nodal conduction and can terminate certain re-entrant tachycardias.
Atrial Fibrillation
Used for ventricular rate control by slowing AV nodal conduction.
Atrial Flutter
Helps control ventricular response rate.
Hypertrophic Cardiomyopathy
May improve symptoms by reducing myocardial contractility and improving ventricular filling.
Adverse Effects
Common adverse effects include:
- Constipation
- Dizziness
- Headache
- Fatigue
- Flushing
- Peripheral edema
- Nausea
Important adverse effects include:
- Bradycardia
- Hypotension
- AV block
- Worsening heart failure
- Sinus node suppression
- Excessive negative inotropic effects
- Gingival hyperplasia (rare)
Intravenous administration may occasionally cause significant hypotension or severe bradyarrhythmias.
Comparative Analysis
| Drug | Class | Primary Site of Action | Major Clinical Use | Important Limitation |
|---|---|---|---|---|
| Verapamil | Non-dihydropyridine CCB | Heart and vessels | Arrhythmias, angina, hypertension | Bradycardia, AV block |
| Diltiazem | Non-dihydropyridine CCB | Heart and vessels | Arrhythmias, angina, hypertension | Bradycardia |
| Amlodipine | Dihydropyridine CCB | Vascular smooth muscle | Hypertension, angina | Peripheral edema |
| Nifedipine | Dihydropyridine CCB | Vascular smooth muscle | Hypertension | Reflex tachycardia |
| Metoprolol | Beta-blocker | Heart | Hypertension, arrhythmias | Bronchospasm risk in susceptible patients |
Verapamil differs from dihydropyridine calcium channel blockers because it has stronger effects on cardiac conduction and contractility. While amlodipine and nifedipine primarily cause vasodilation, verapamil significantly slows heart rate and AV nodal conduction, making it useful in arrhythmias.
MCQs
1. Verapamil belongs to which class of drugs?
a) Beta-blockers
b) ACE inhibitors
c) Non-dihydropyridine calcium channel blockers
d) ARBs
Answer: c) Non-dihydropyridine calcium channel blockers
2. Verapamil primarily blocks:
a) Sodium channels
b) Potassium channels
c) L-type calcium channels
d) Chloride channels
Answer: c) L-type calcium channels
3. The antiarrhythmic action of verapamil is mainly due to:
a) Sodium channel blockade
b) AV nodal conduction slowing
c) Increased sympathetic activity
d) Potassium channel activation
Answer: b) AV nodal conduction slowing
4. Verapamil produces which cardiac effect?
a) Positive chronotropic effect
b) Negative chronotropic effect
c) Positive inotropic effect
d) Increased automaticity
Answer: b) Negative chronotropic effect
5. Which node is most affected by verapamil?
a) Purkinje fibers
b) Bundle of His
c) AV node
d) Ventricular myocardium
Answer: c) AV node
6. A common adverse effect of verapamil is:
a) Constipation
b) Hyperglycemia
c) Nephrotoxicity
d) Ototoxicity
Answer: a) Constipation
7. Verapamil decreases myocardial oxygen demand by:
a) Increasing contractility
b) Increasing heart rate
c) Reducing heart rate and contractility
d) Stimulating sympathetic activity
Answer: c) Reducing heart rate and contractility
8. Which enzyme primarily metabolizes verapamil?
a) CYP2D6
b) CYP2C19
c) CYP1A2
d) CYP3A4
Answer: d) CYP3A4
9. Verapamil is useful in:
a) Supraventricular tachycardia
b) Tuberculosis
c) Parkinson disease
d) Epilepsy
Answer: a) Supraventricular tachycardia
10. Excessive verapamil therapy may cause:
a) Bradycardia
b) Hyperthyroidism
c) Polycythemia
d) Hyperkalemia
Answer: a) Bradycardia
FAQs
What is the mechanism of action of verapamil?
Verapamil blocks L-type calcium channels in the heart and blood vessels, reducing calcium influx, slowing AV nodal conduction, decreasing heart rate, and producing vasodilation.
Is verapamil a calcium channel blocker?
Yes. Verapamil is a non-dihydropyridine calcium channel blocker with significant effects on the heart and vascular smooth muscle.
Why is verapamil used in supraventricular tachycardia?
It slows conduction through the AV node and increases AV nodal refractoriness, helping terminate or control supraventricular tachyarrhythmias.
How does verapamil help in angina?
Verapamil decreases myocardial oxygen demand by reducing heart rate, contractility, and afterload while improving coronary blood flow.
What is the most common adverse effect of verapamil?
Constipation is one of the most common adverse effects associated with verapamil therapy.
Can verapamil cause bradycardia?
Yes. Excessive suppression of SA and AV nodal activity may lead to bradycardia and conduction abnormalities.
Why should verapamil be used cautiously in heart failure?
Because of its negative inotropic effect, verapamil can worsen systolic heart failure in susceptible patients.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
Katzung Basic & Clinical Pharmacology
K.D. Tripathi Essentials of Medical Pharmacology
Harrison’s Principles of Internal Medicine
