
Table of Contents
Introduction
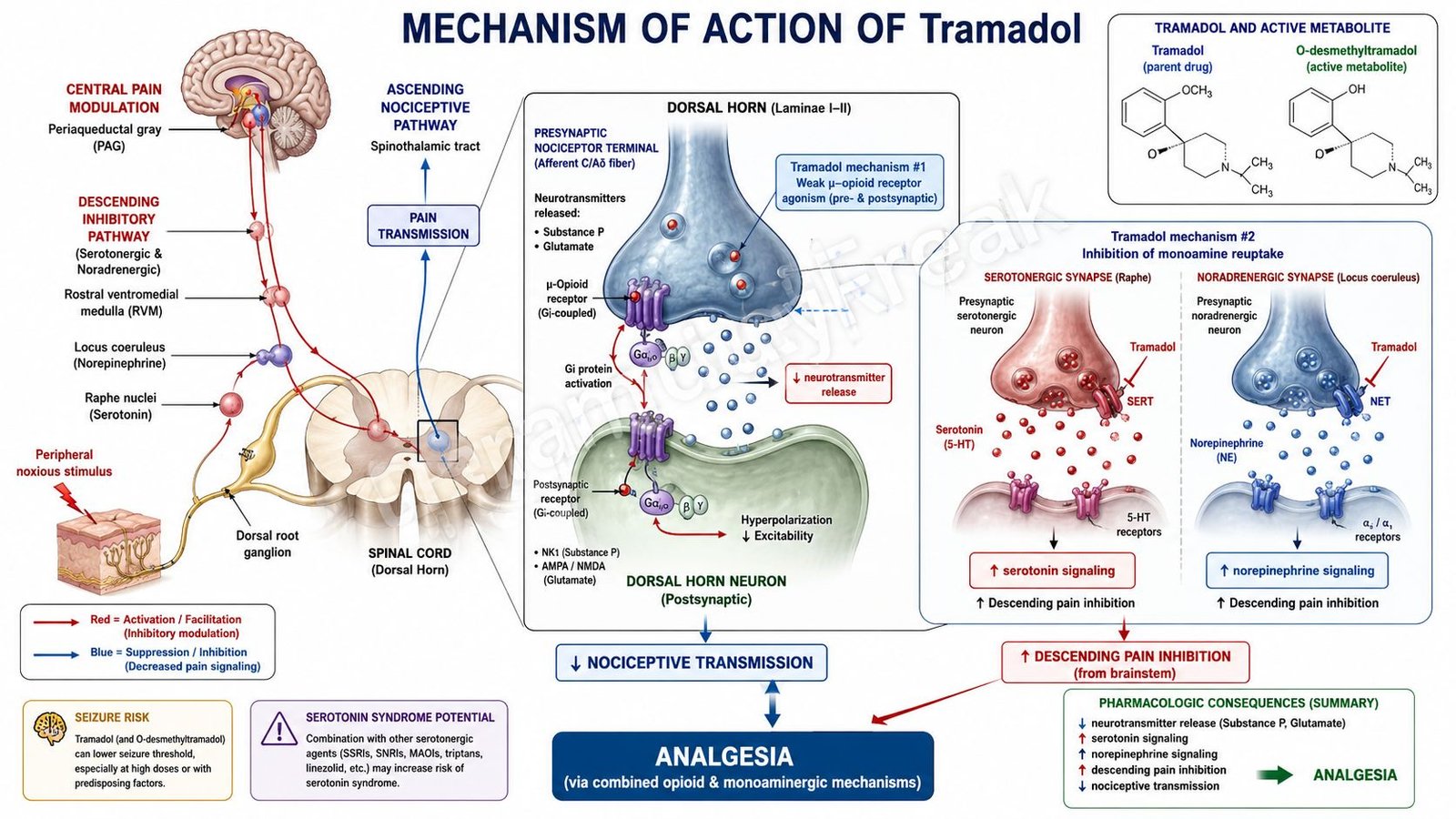
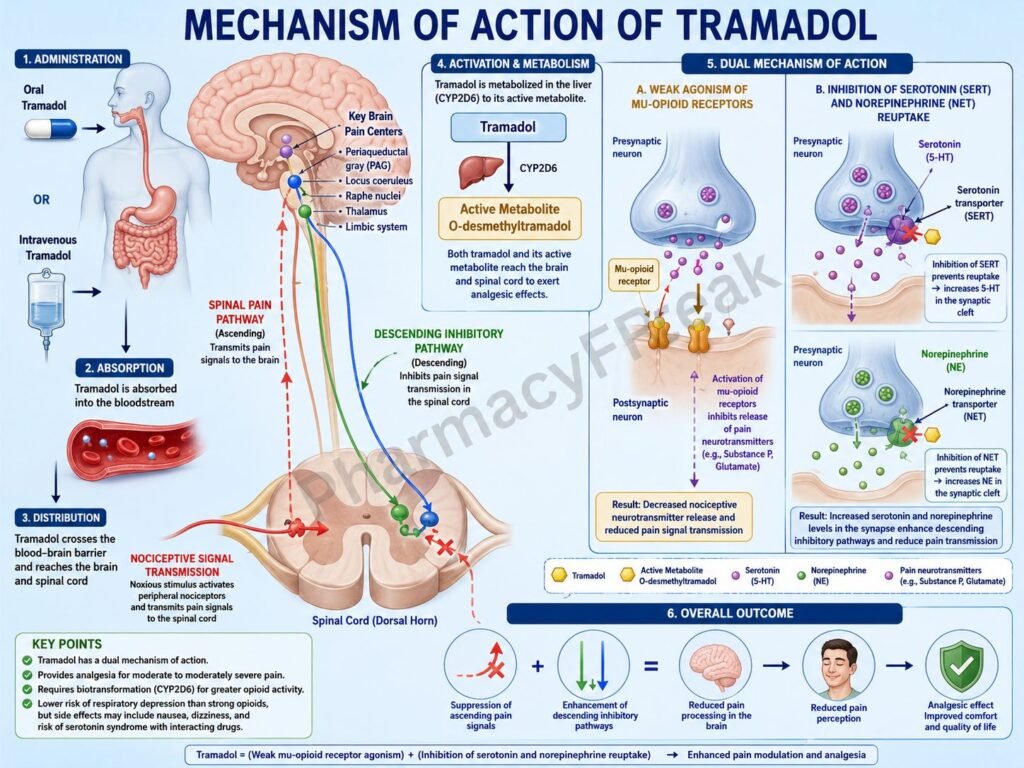
Tramadol is a centrally acting analgesic used for the management of moderate to moderately severe pain. It has a unique dual mechanism of action, functioning as both a weak μ-opioid receptor agonist and an inhibitor of norepinephrine and serotonin reuptake. This combination provides effective pain relief while producing less respiratory depression than many traditional opioids at therapeutic doses.
Mechanism of Action (Step-wise)
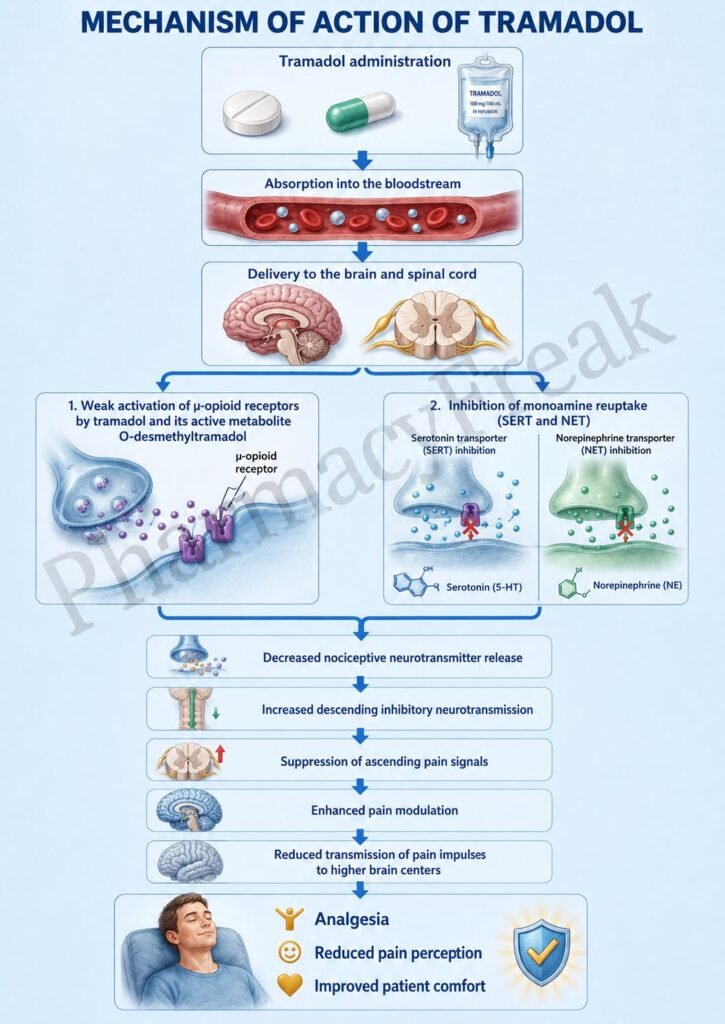
- Tramadol is administered orally, intravenously, or intramuscularly and enters the central nervous system.
- In the liver, tramadol is metabolized by CYP2D6 to an active metabolite, O-desmethyltramadol (M1).
- The M1 metabolite has a higher affinity for μ-opioid receptors than the parent drug.
- Tramadol and its metabolite bind to μ-opioid receptors in the brain and spinal cord.
- Activation of μ-opioid receptors inhibits adenylate cyclase activity.
- Intracellular cyclic AMP (cAMP) levels decrease.
- Potassium efflux increases and neuronal membranes become hyperpolarized.
- Calcium influx into presynaptic nerve terminals decreases.
- Release of pain neurotransmitters such as substance P and glutamate is reduced.
- Tramadol also inhibits norepinephrine reuptake by blocking norepinephrine transporters (NET).
- It inhibits serotonin reuptake by blocking serotonin transporters (SERT).
- Increased norepinephrine and serotonin concentrations enhance descending inhibitory pain pathways in the spinal cord.
- Pain signal transmission is suppressed at both spinal and supraspinal levels.
- The overall effect is analgesia through opioid and monoaminergic mechanisms.
A key exam point is that tramadol produces analgesia through weak μ-opioid receptor agonism and inhibition of serotonin and norepinephrine reuptake.
Pharmacokinetics
Tramadol is well absorbed after oral administration. It undergoes hepatic metabolism primarily through CYP2D6 and CYP3A4. The active metabolite contributes significantly to analgesic activity. Elimination occurs mainly through the kidneys. Dose adjustment may be required in renal or hepatic impairment.
Clinical Uses
Tramadol is used in:
- Moderate pain
- Chronic pain syndromes
- Postoperative pain
- Musculoskeletal pain
- Neuropathic pain (selected cases)
- Cancer-related pain (adjunctive use)
Adverse Effects
Common adverse effects include:
- Nausea
- Vomiting
- Dizziness
- Drowsiness
- Constipation
- Dry mouth
Serious adverse effects include:
- Seizures
- Serotonin syndrome
- Respiratory depression
- Dependence and misuse potential
Risk of serotonin syndrome increases when combined with SSRIs, SNRIs, MAO inhibitors, or other serotonergic drugs.
Comparative Analysis
| Feature | Tramadol | Morphine | Codeine |
|---|---|---|---|
| μ-opioid receptor agonism | Weak | Strong | Moderate |
| Norepinephrine reuptake inhibition | Yes | No | No |
| Serotonin reuptake inhibition | Yes | No | No |
| Seizure risk | Higher | Lower | Lower |
| Serotonin syndrome risk | Present | Minimal | Minimal |
| Respiratory depression | Less pronounced | Significant | Moderate |
Tramadol differs from morphine and codeine because it combines opioid receptor agonism with inhibition of norepinephrine and serotonin reuptake. This dual mechanism contributes to its analgesic effects but also increases the risk of serotonin syndrome and seizures.
MCQs
1. Tramadol primarily acts as a:
a) Pure opioid antagonist
b) Weak μ-opioid receptor agonist
c) NSAID
d) Local anesthetic
Answer: b) Weak μ-opioid receptor agonist
2. Tramadol also inhibits reuptake of:
a) Dopamine only
b) Serotonin and norepinephrine
c) Histamine and acetylcholine
d) GABA and glycine
Answer: b) Serotonin and norepinephrine
3. The active metabolite of tramadol is:
a) Morphine
b) O-desmethyltramadol
c) Norcodeine
d) Naloxone
Answer: b) O-desmethyltramadol
4. Activation of μ-opioid receptors causes:
a) Increased neurotransmitter release
b) Reduced neurotransmitter release
c) Increased calcium influx
d) Increased pain transmission
Answer: b) Reduced neurotransmitter release
5. Tramadol is commonly used for:
a) Moderate pain
b) Hypertension
c) Asthma
d) Hyperthyroidism
Answer: a) Moderate pain
6. Which neurotransmitter release is reduced by opioid receptor activation?
a) Substance P
b) Insulin
c) Histamine
d) Thyroxine
Answer: a) Substance P
7. A common adverse effect is:
a) Dizziness
b) Hypercalcemia
c) Polycythemia
d) Hyperthyroidism
Answer: a) Dizziness
8. A serious adverse effect associated with tramadol is:
a) Seizures
b) Cataracts
c) Hypernatremia
d) Glaucoma
Answer: a) Seizures
9. Tramadol increases risk of serotonin syndrome when combined with:
a) SSRIs
b) Antacids
c) Calcium supplements
d) Diuretics
Answer: a) SSRIs
10. Tramadol is metabolized primarily by:
a) CYP2D6 and CYP3A4
b) CYP1A2 only
c) Monoamine oxidase
d) Xanthine oxidase
Answer: a) CYP2D6 and CYP3A4
11. Compared with morphine, tramadol has:
a) Additional monoamine reuptake inhibition
b) Stronger opioid activity
c) No CNS effects
d) Greater respiratory depression
Answer: a) Additional monoamine reuptake inhibition
12. The analgesic effect of tramadol results from:
a) μ-opioid receptor activation and monoamine reuptake inhibition
b) Cyclooxygenase inhibition only
c) Calcium channel blockade
d) Histamine receptor antagonism
Answer: a) μ-opioid receptor activation and monoamine reuptake inhibition
FAQs
What is the mechanism of action of tramadol?
Tramadol acts as a weak μ-opioid receptor agonist and inhibits serotonin and norepinephrine reuptake, producing analgesia.
Why is tramadol considered different from traditional opioids?
Because it has a dual mechanism involving both opioid receptors and monoamine neurotransmitter pathways.
What is the active metabolite of tramadol?
O-desmethyltramadol (M1), which has stronger μ-opioid receptor activity.
What are common side effects of tramadol?
Nausea, dizziness, drowsiness, constipation, and vomiting.
Can tramadol cause serotonin syndrome?
Yes, especially when combined with SSRIs, SNRIs, MAO inhibitors, or other serotonergic medications.
Why can tramadol cause seizures?
Its monoaminergic activity lowers the seizure threshold, particularly at high doses or in susceptible patients.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung’s Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi KD. Essentials of Medical Pharmacology
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com

