
Table of Contents
Introduction
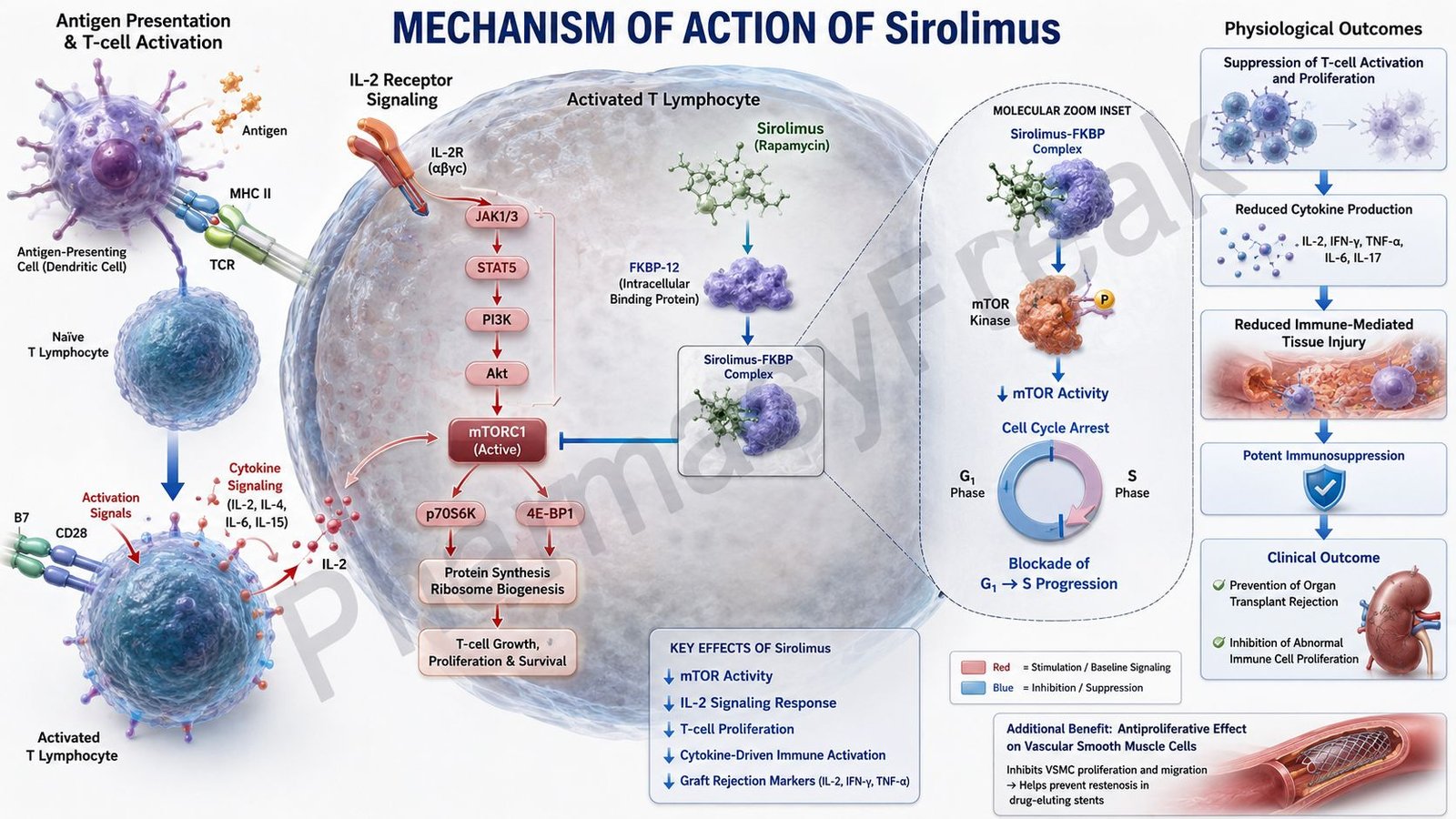
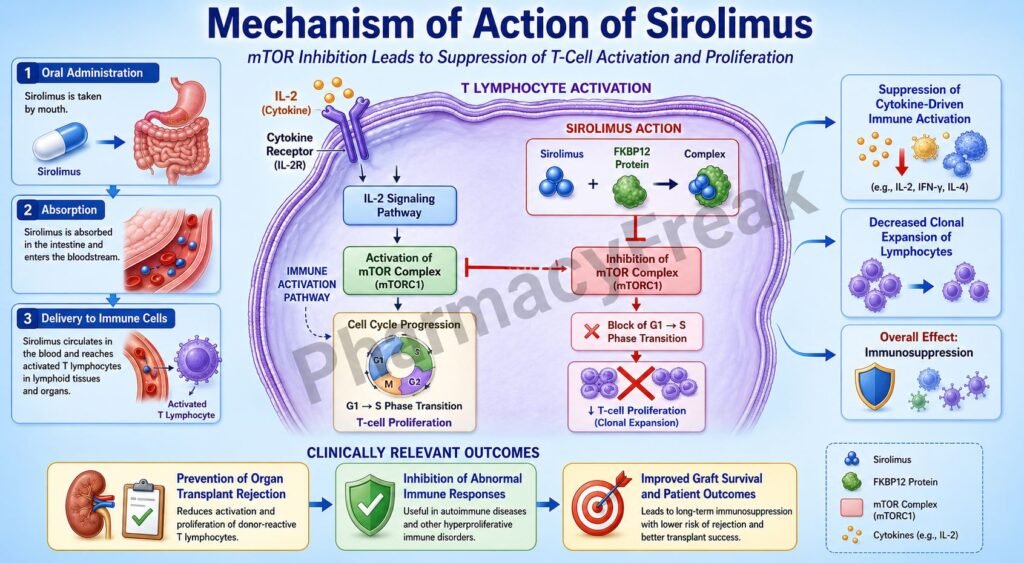
Sirolimus, also known as rapamycin, is an immunosuppressant drug primarily used in organ transplantation and certain proliferative disorders. It inhibits T-cell activation and proliferation by blocking the mammalian target of rapamycin (mTOR) pathway. Unlike calcineurin inhibitors, sirolimus does not inhibit interleukin-2 production but instead blocks the cellular response to interleukin-2.
Mechanism of Action (Step-wise)
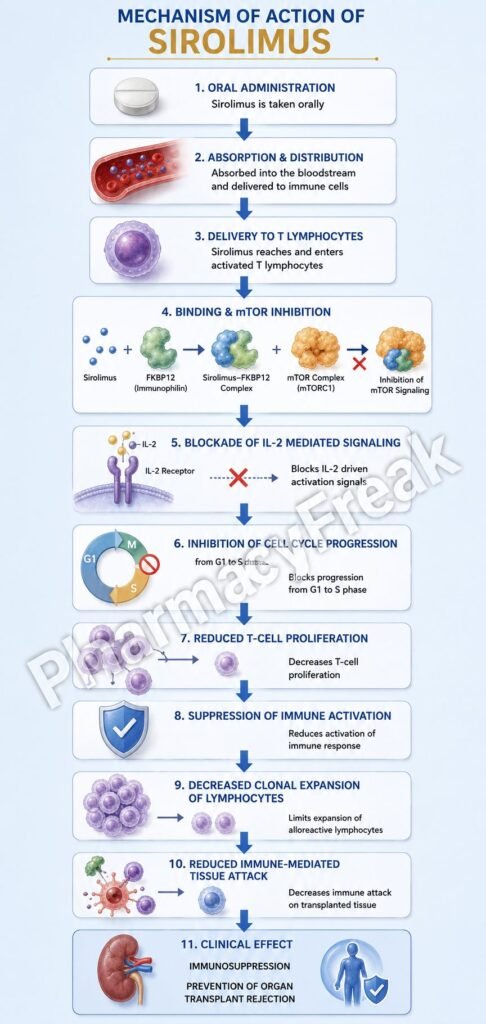
- Sirolimus enters immune cells, especially T lymphocytes.
- Inside the cell, sirolimus binds to the intracellular immunophilin FK-binding protein-12 (FKBP-12).
- The sirolimus-FKBP12 complex inhibits mammalian target of rapamycin (mTOR).
- mTOR is a kinase involved in cell cycle progression and protein synthesis.
- Normally, interleukin-2 (IL-2) stimulates mTOR signaling and promotes T-cell proliferation.
- Inhibition of mTOR blocks progression of T cells from the G1 phase to the S phase of the cell cycle.
- T-cell proliferation and clonal expansion decrease.
- B-cell proliferation and antibody production are also reduced.
- Sirolimus additionally inhibits smooth muscle proliferation, reducing risk of restenosis in coronary stents.
- The overall effect is suppression of immune activation and prevention of graft rejection.
A key exam point is that sirolimus binds FKBP-12 and inhibits mTOR, blocking IL-2-mediated T-cell proliferation.
Pharmacokinetics
Sirolimus is administered orally and undergoes hepatic metabolism mainly through CYP3A4. It has a long half-life and is highly protein bound. Elimination occurs primarily through feces.
Clinical Uses
Sirolimus is used for prevention of organ transplant rejection, especially in renal transplantation. It is also used in drug-eluting coronary stents and certain rare disorders such as lymphangioleiomyomatosis.
Adverse Effects
Common adverse effects include hyperlipidemia, thrombocytopenia, leukopenia, anemia, delayed wound healing, and mouth ulcers. Compared with calcineurin inhibitors, sirolimus has less nephrotoxicity but may increase infection risk due to immunosuppression.
Comparative Analysis
| Feature | Sirolimus | Tacrolimus | Cyclosporine |
|---|---|---|---|
| Main target | mTOR | Calcineurin | Calcineurin |
| Binding protein | FKBP-12 | FKBP-12 | Cyclophilin |
| IL-2 production | Not inhibited | Decreased | Decreased |
| T-cell proliferation | Blocked | Reduced | Reduced |
| Nephrotoxicity | Lower | Higher | Higher |
| Hyperlipidemia | Common | Less common | Moderate |
Sirolimus differs from tacrolimus and cyclosporine because it inhibits the response to IL-2 rather than IL-2 synthesis itself.
MCQs
- Sirolimus is also known as:
a) Tacrolimus
b) Rapamycin
c) Cyclosporine
d) Azathioprine
Answer: b) Rapamycin
- Sirolimus binds to which intracellular protein?
a) Cyclophilin
b) FKBP-12
c) Calmodulin
d) Albumin
Answer: b) FKBP-12
- The sirolimus-FKBP12 complex inhibits:
a) Calcineurin
b) mTOR
c) Acetylcholinesterase
d) Cyclooxygenase
Answer: b) mTOR
- mTOR is important for:
a) T-cell proliferation
b) Histamine synthesis
c) Cholesterol absorption
d) Calcium excretion
Answer: a) T-cell proliferation
- Sirolimus blocks progression of T cells from:
a) M phase to G1 phase
b) G1 phase to S phase
c) S phase to G2 phase
d) G2 phase to M phase
Answer: b) G1 phase to S phase
- Sirolimus mainly suppresses responses to:
a) Interleukin-2
b) Histamine
c) Dopamine
d) Acetylcholine
Answer: a) Interleukin-2
- Sirolimus is mainly used in:
a) Organ transplantation
b) Asthma
c) Diabetes mellitus
d) Epilepsy
Answer: a) Organ transplantation
- Compared with calcineurin inhibitors, sirolimus has:
a) Greater nephrotoxicity
b) Lower nephrotoxicity
c) No immunosuppressive effect
d) More calcium channel blockade
Answer: b) Lower nephrotoxicity
- A common adverse effect of sirolimus is:
a) Hyperlipidemia
b) Hypercalcemia
c) Severe bradycardia
d) Cataracts
Answer: a) Hyperlipidemia
- Sirolimus is metabolized mainly by:
a) CYP2D6
b) CYP3A4
c) MAO
d) Xanthine oxidase
Answer: b) CYP3A4
- Drug-eluting stents containing sirolimus work mainly by inhibiting:
a) Smooth muscle proliferation
b) Histamine release
c) Platelet aggregation only
d) Sodium transport
Answer: a) Smooth muscle proliferation
- Sirolimus differs from tacrolimus because it mainly inhibits:
a) IL-2 production
b) Response to IL-2
c) Dopamine synthesis
d) Acetylcholine release
Answer: b) Response to IL-2
FAQs
What is the mechanism of action of sirolimus?
Sirolimus binds FKBP-12 and inhibits mTOR, blocking IL-2-mediated T-cell proliferation.
Why is sirolimus used in organ transplantation?
Because it suppresses immune activation and helps prevent graft rejection.
How does sirolimus differ from tacrolimus?
Sirolimus blocks the response to IL-2, while tacrolimus inhibits IL-2 production.
What are common side effects of sirolimus?
Hyperlipidemia, thrombocytopenia, leukopenia, and delayed wound healing.
Why is sirolimus used in coronary stents?
Because it inhibits smooth muscle proliferation and reduces restenosis.
Does sirolimus cause nephrotoxicity?
It causes less nephrotoxicity than calcineurin inhibitors.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Immunosuppressant Drugs
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Immunopharmacology
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Immunosuppressant Drugs
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Organ Transplantation and Immunosuppression
https://accessmedicine.mhmedical.com

