Table of Contents
Introduction
Sulfonylureas are one of the oldest and most widely used classes of oral antidiabetic agents. They are particularly effective in patients with type 2 diabetes mellitus who have residual pancreatic beta-cell function.
They exert their effect by stimulating insulin secretion from pancreatic beta cells. Sulfonylureas are typically used in combination with other agents or as monotherapy in early-stage type 2 diabetes.
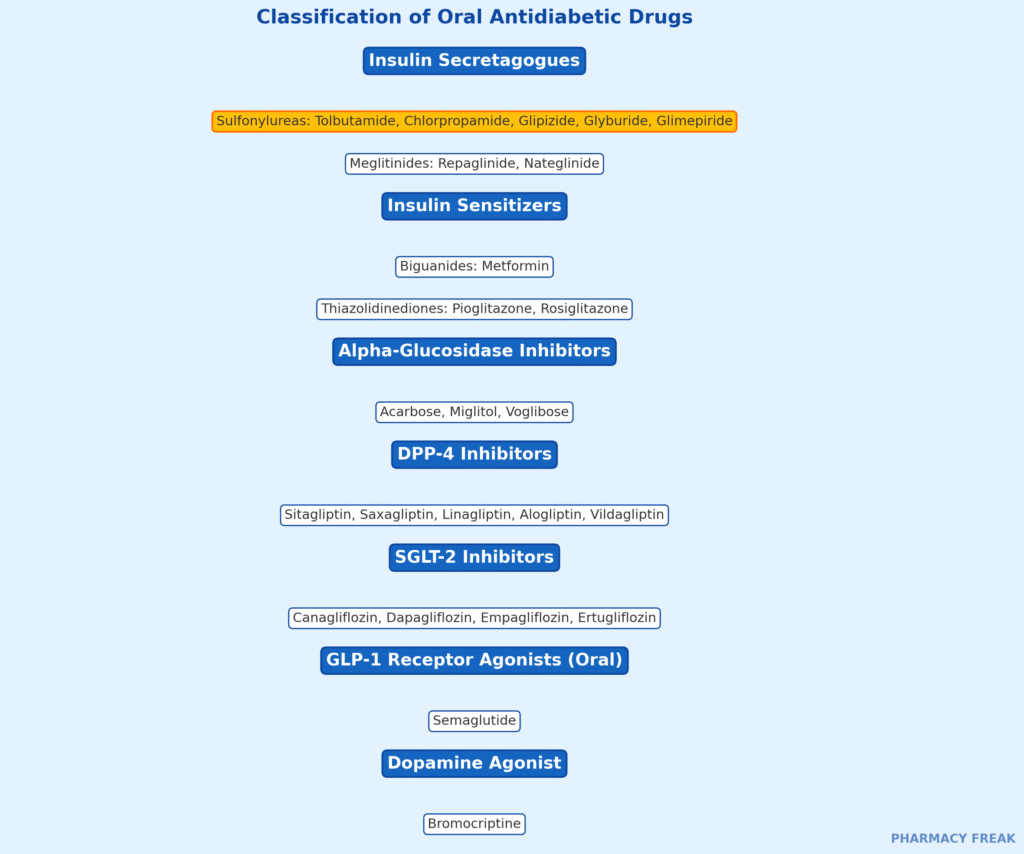
Common examples include:
- Glibenclamide (Glyburide)
- Glipizide
- Gliclazide
- Glimepiride
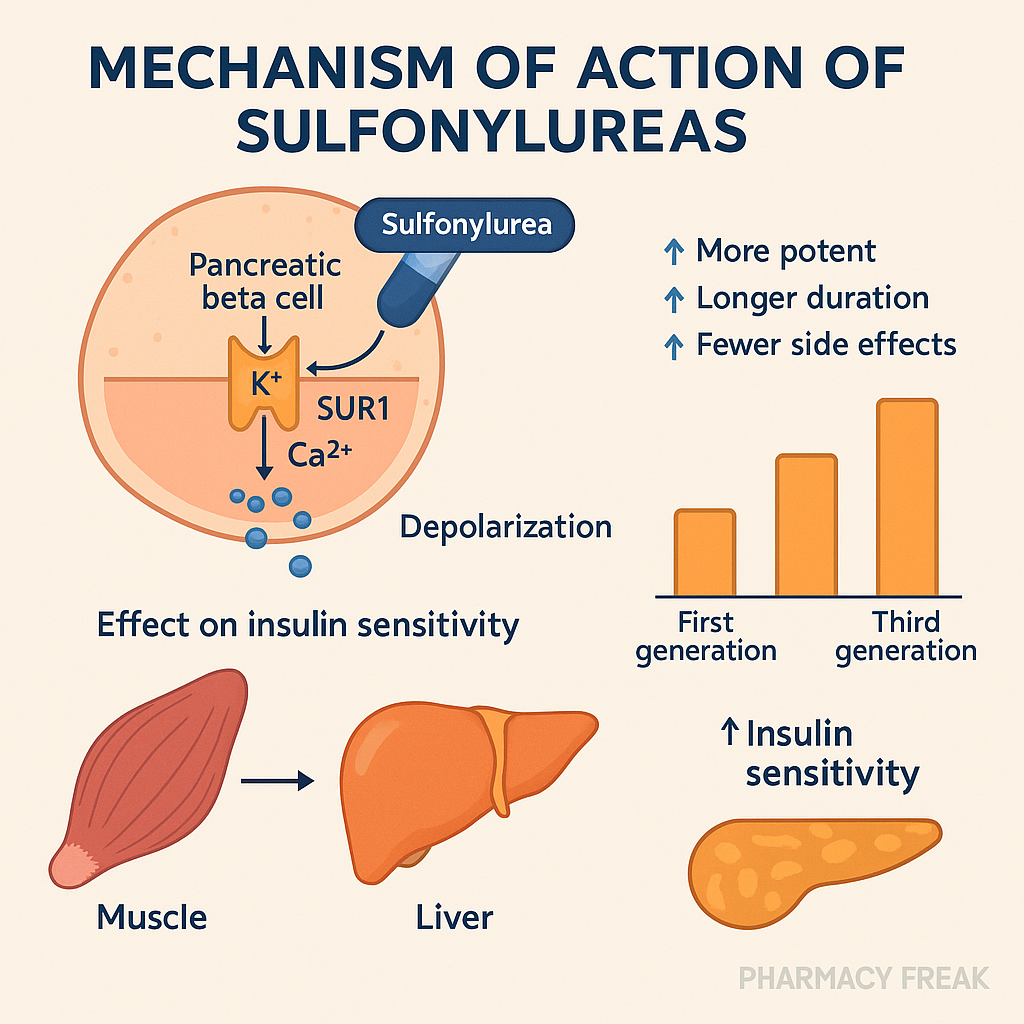
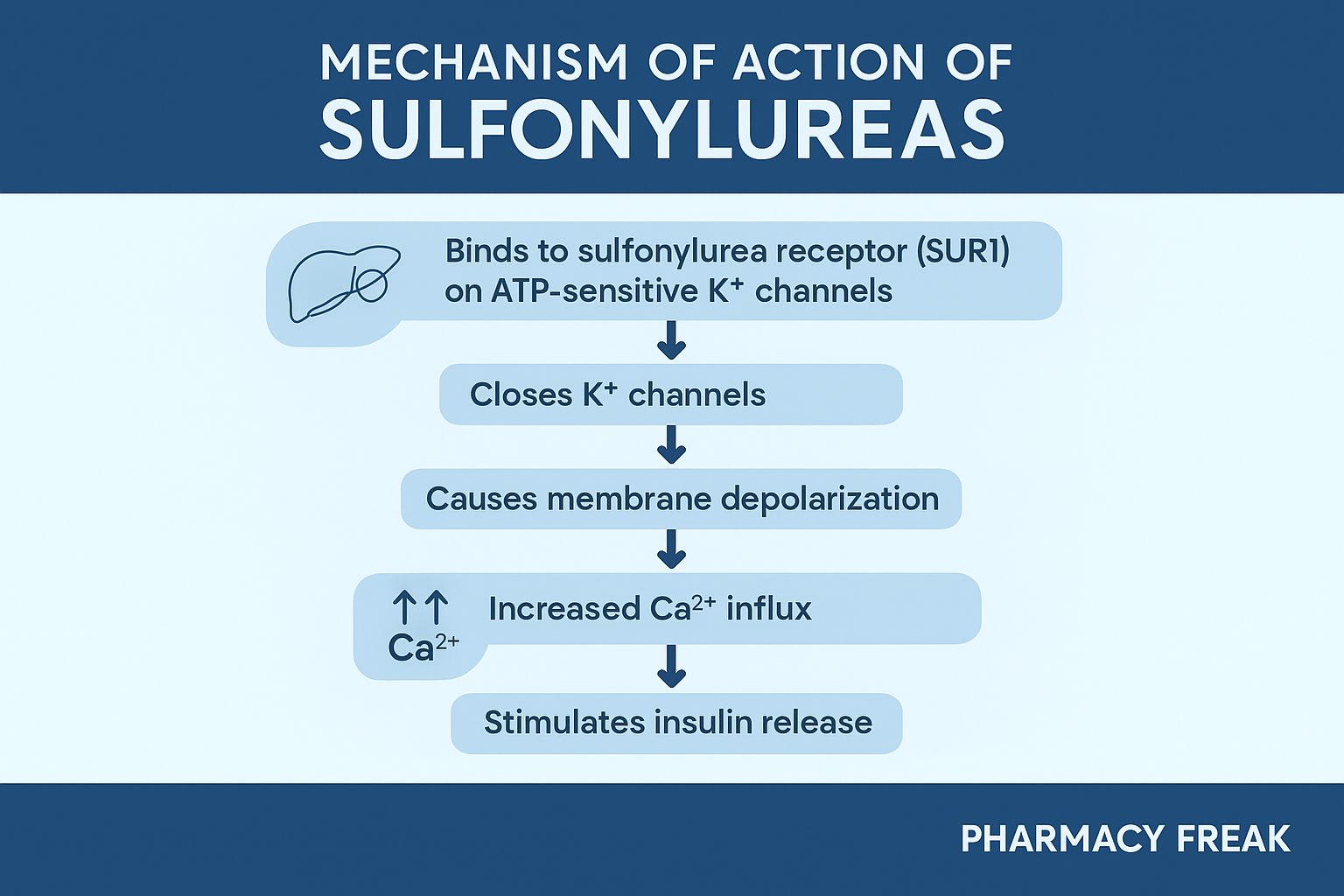
Stepwise Mechanism of Action of Sulfonylureas
- Binding to Sulfonylurea Receptor (SUR1):
Sulfonylureas bind to the sulfonylurea receptor 1 (SUR1), which is part of the ATP-sensitive potassium (K⁺-ATP) channel on pancreatic beta cells. - Inhibition of K⁺ Efflux:
Binding leads to closure of the K⁺-ATP channel, preventing potassium efflux from the beta cell. - Depolarization of the Cell Membrane:
The intracellular accumulation of potassium causes membrane depolarization. - Opening of Voltage-Gated Calcium Channels:
Depolarization leads to opening of voltage-gated Ca²⁺ channels, resulting in calcium influx into the cell. - Exocytosis of Insulin:
Increased intracellular calcium triggers the exocytosis of insulin-containing vesicles, leading to increased insulin release. - Glucose-Independent Action:
Unlike newer drugs, sulfonylureas stimulate insulin secretion independent of blood glucose levels, which increases the risk of hypoglycemia.
Pharmacokinetic Parameters of Sulfonylureas
| Drug | Onset | Duration | Metabolism | Excretion |
|---|---|---|---|---|
| Glipizide | Fast | 10–24 hrs | Hepatic | Renal |
| Glibenclamide | Moderate | 18–24 hrs | Hepatic | Renal/Biliary |
| Glimepiride | Fast | 24 hrs | Hepatic | Renal |
| Gliclazide | Moderate | 10–12 hrs | Hepatic | Renal |
Clinical Uses of Sulfonylureas
- Type 2 diabetes mellitus (especially early stage)
- Used in combination with metformin, DPP-4 inhibitors, or insulin
- Effective in patients with preserved beta-cell function
Adverse Effects of Sulfonylureas
- Hypoglycemia – most common and serious side effect
- Weight gain
- GI upset – nausea, bloating
- Allergic reactions – skin rash, photosensitivity
- Hyponatremia (rare, especially with chlorpropamide)
- Hepatotoxicity and cholestasis (rare)
Comparative Analysis: First vs Second Generation Sulfonylureas
| Feature | First Generation (e.g., Tolbutamide) | Second Generation (e.g., Glimepiride) |
|---|---|---|
| Potency | Lower | Higher |
| Half-life | Short | Longer |
| Side effects | More frequent | Less frequent |
| Dosing frequency | Multiple times daily | Once daily |
| Risk of hypoglycemia | Higher | Moderate |
Practice MCQs
Q1. Sulfonylureas lower blood glucose by:
a. Increasing glucose absorption
b. Enhancing insulin sensitivity
c. Stimulating insulin secretion ✅
d. Inhibiting gluconeogenesis
Q2. The receptor targeted by sulfonylureas is located on:
a. Alpha cells
b. Hepatocytes
c. Beta cells ✅
d. Muscle cells
Q3. The direct cellular effect of sulfonylureas is:
a. Opening potassium channels
b. Closing ATP-sensitive potassium channels ✅
c. Stimulating AMPK
d. Inhibiting alpha-glucosidase
Q4. What electrolyte movement is triggered by sulfonylureas?
a. Sodium influx
b. Potassium influx
c. Calcium influx ✅
d. Chloride efflux
Q5. What is the most serious side effect of sulfonylureas?
a. Hyperglycemia
b. Nausea
c. Hypoglycemia ✅
d. Tachycardia
Q6. Which sulfonylurea has the longest duration of action?
a. Tolbutamide
b. Glipizide
c. Glimepiride ✅
d. Gliclazide
Q7. Sulfonylureas should be used with caution in:
a. Asthma
b. Renal impairment ✅
c. Hyperlipidemia
d. Hypothyroidism
Q8. Which condition enhances the risk of sulfonylurea-induced hypoglycemia?
a. High protein intake
b. Chronic alcohol use ✅
c. High fiber diet
d. Corticosteroid therapy
Q9. Sulfonylureas are ineffective in:
a. Type 2 diabetes
b. New-onset diabetes
c. Type 1 diabetes ✅
d. Gestational diabetes
Q10. Which drug has similar action but shorter onset than sulfonylureas?
a. Pioglitazone
b. Metformin
c. Repaglinide ✅
d. Acarbose
FAQs
Q1: Can sulfonylureas be used in type 1 diabetes?
No. They require functional beta cells and are ineffective in type 1 diabetes.
Q2: Can sulfonylureas cause weight loss?
No. They are commonly associated with weight gain due to increased insulin levels.
Q3: How should sulfonylureas be administered?
They are taken orally, 30 minutes before meals, to match postprandial glucose peaks.
Q4: Which patients should avoid sulfonylureas?
Patients with frequent hypoglycemia, severe liver/renal dysfunction, or elderly frail individuals.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Review of Pharmacology – Sparsh Gupta
- ADA Guidelines
- NCBI: https://www.ncbi.nlm.nih.gov/books/NBK548227/


