Table of Contents
Introduction
Amlodipine is a commonly prescribed dihydropyridine calcium channel blocker (CCB) used in the treatment of hypertension, angina pectoris, and coronary artery disease. It works by relaxing vascular smooth muscle, leading to vasodilation and reduced blood pressure. With its once-daily dosing, long half-life, and minimal cardiac depression, it is a key drug in cardiovascular therapy.
This drug is high-yield for exams like USMLE, NCLEX, GPAT, NAPLEX, and NEET-PG, especially in cardiovascular pharmacology.
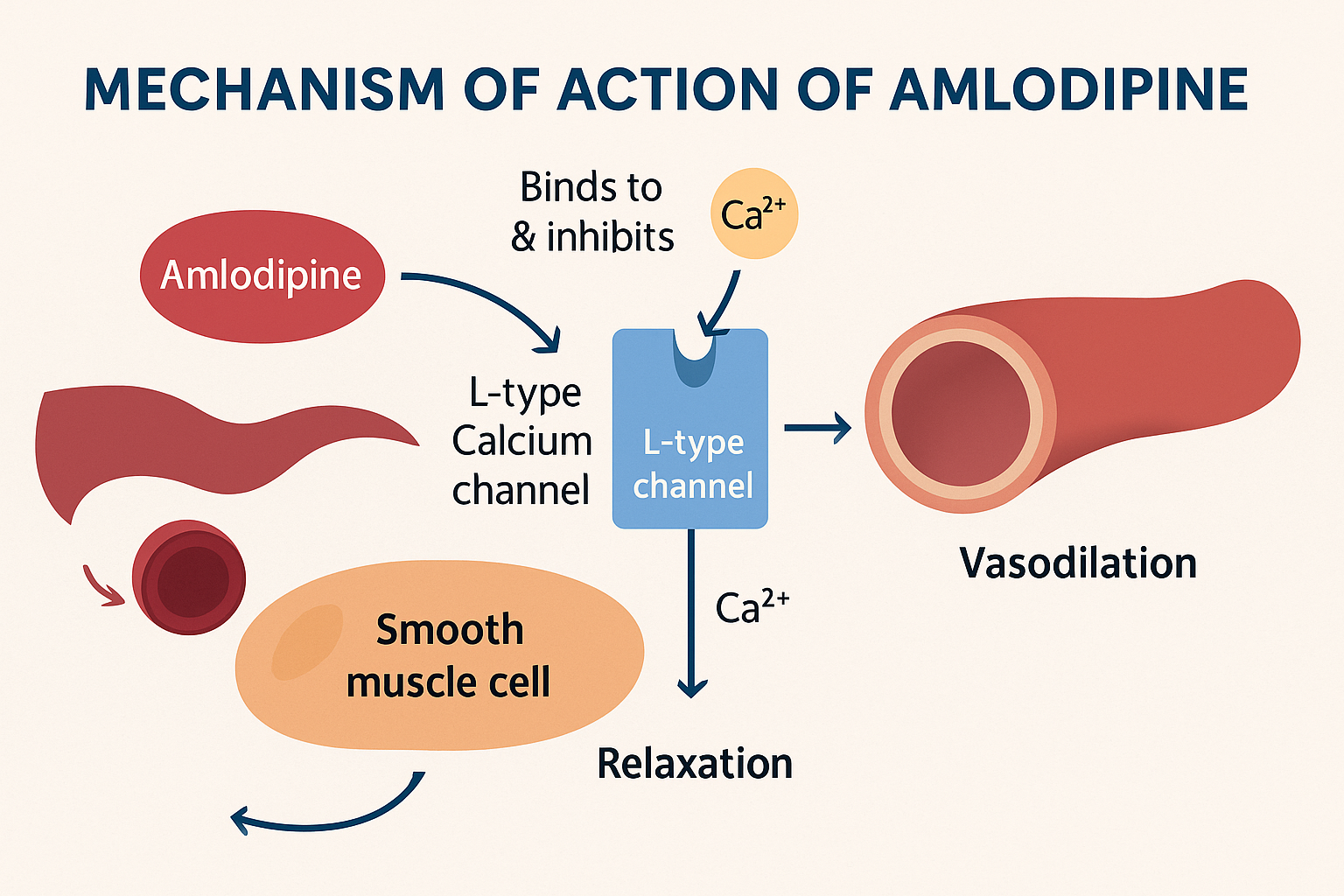
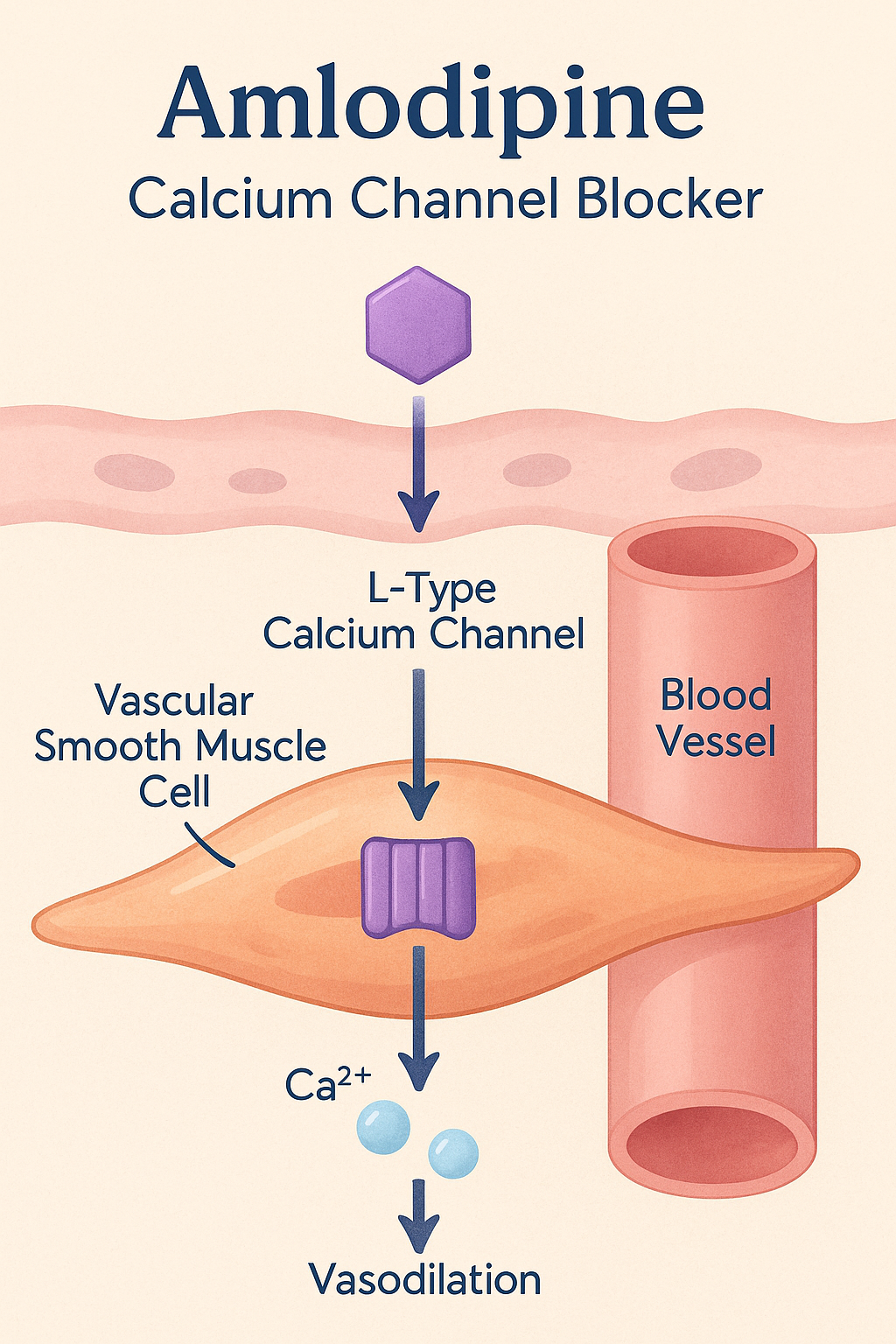
Mechanism of Action of Amlodipine: Step-by-Step
- Selective inhibition of L-type calcium channels
Amlodipine binds to and inhibits L-type voltage-gated calcium channels on vascular smooth muscle cells. - Reduced intracellular Ca²⁺ influx
By blocking these channels, it prevents calcium entry into the cells, which is necessary for muscle contraction. - Vasodilation of arterioles
Reduced intracellular calcium leads to relaxation of vascular smooth muscle, especially in arterioles (not veins), causing peripheral vasodilation. - Decreased peripheral vascular resistance
The vasodilation results in a decrease in systemic vascular resistance, thus lowering blood pressure. - Minimal effect on cardiac conduction
Unlike non-dihydropyridine CCBs (e.g., verapamil), amlodipine has little effect on the SA or AV node, avoiding bradycardia.
Pharmacokinetic Parameters of Amlodipine
| Parameter | Value |
|---|---|
| Bioavailability | ~60–65% |
| Half-life | 30–50 hours |
| Time to peak | 6–12 hours |
| Protein binding | ~93% |
| Metabolism | Hepatic (CYP3A4) |
| Excretion | Renal and hepatic |
| Dosing | Once daily |
Clinical Uses of Amlodipine
- Hypertension (first-line agent)
- Stable angina
- Vasospastic (Prinzmetal’s) angina
- Coronary artery disease (CAD)
- Raynaud’s phenomenon (off-label)
Adverse Effects of Amlodipine
- Peripheral edema (most common)
- Headache
- Flushing
- Dizziness
- Reflex tachycardia (mild, dose-dependent)
- Gingival hyperplasia (rare)
- Fatigue
Comparative Analysis: Amlodipine vs Verapamil
| Feature | Amlodipine | Verapamil |
|---|---|---|
| Class | Dihydropyridine CCB | Non-dihydropyridine CCB |
| Main effect | Vasodilation | Cardiac conduction slowing |
| AV nodal blocking | Minimal | Strong |
| Use in heart failure | Safe | Avoid in reduced EF |
| Reflex tachycardia | Possible | No |
| Edema risk | High | Low |
Practice MCQs
Q1. What is the primary mechanism of amlodipine?
a. β-blockade
b. Inhibition of angiotensin II
c. L-type calcium channel blockade ✅
d. Sodium channel blockade
Q2. Amlodipine causes:
a. Vasoconstriction
b. Bradycardia
c. Vasodilation ✅
d. Increased preload
Q3. What is the most common side effect of amlodipine?
a. Hypokalemia
b. Peripheral edema ✅
c. Cough
d. Arrhythmia
Q4. Amlodipine acts mainly on:
a. Cardiac muscle
b. Veins
c. Arterioles ✅
d. Capillaries
Q5. Which calcium channel type is inhibited by amlodipine?
a. T-type
b. N-type
c. P-type
d. L-type ✅
Q6. Compared to verapamil, amlodipine:
a. Causes bradycardia
b. Affects AV node strongly
c. Has minimal cardiac effect ✅
d. Is used only for arrhythmias
Q7. The half-life of amlodipine is approximately:
a. 2–4 hours
b. 6–8 hours
c. 12–24 hours
d. 30–50 hours ✅
Q8. Gingival hyperplasia is a rare side effect of:
a. Amlodipine ✅
b. Atenolol
c. Furosemide
d. Captopril
Q9. Amlodipine is safe in:
a. Pregnancy
b. Bradyarrhythmia
c. Left ventricular failure with reduced EF ✅
d. Acute MI
Q10. Which statement about amlodipine is FALSE?
a. It blocks calcium influx
b. It decreases systemic vascular resistance
c. It increases heart rate significantly ✅
d. It causes dose-dependent edema
FAQs
Q1: Can amlodipine be used in elderly patients?
Yes. It’s commonly used due to once-daily dosing and good tolerability.
Q2: Does amlodipine affect heart rate?
No significant effect. It has minimal action on cardiac nodes.
Q3: Why does amlodipine cause edema?
Due to pre-capillary arteriolar dilation, leading to fluid transudation.
Q4: Is dose adjustment needed in renal impairment?
No. Generally safe without dose adjustment.
Q5: Can amlodipine be combined with β-blockers?
Yes, commonly done to control BP and heart rate synergistically.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Sparsh Gupta – Review of Pharmacology
- NCBI: https://www.ncbi.nlm.nih.gov/books/NBK470557/



Love this, make me understand mechanism amlodipine, thank you. support u