Table of Contents
Introduction
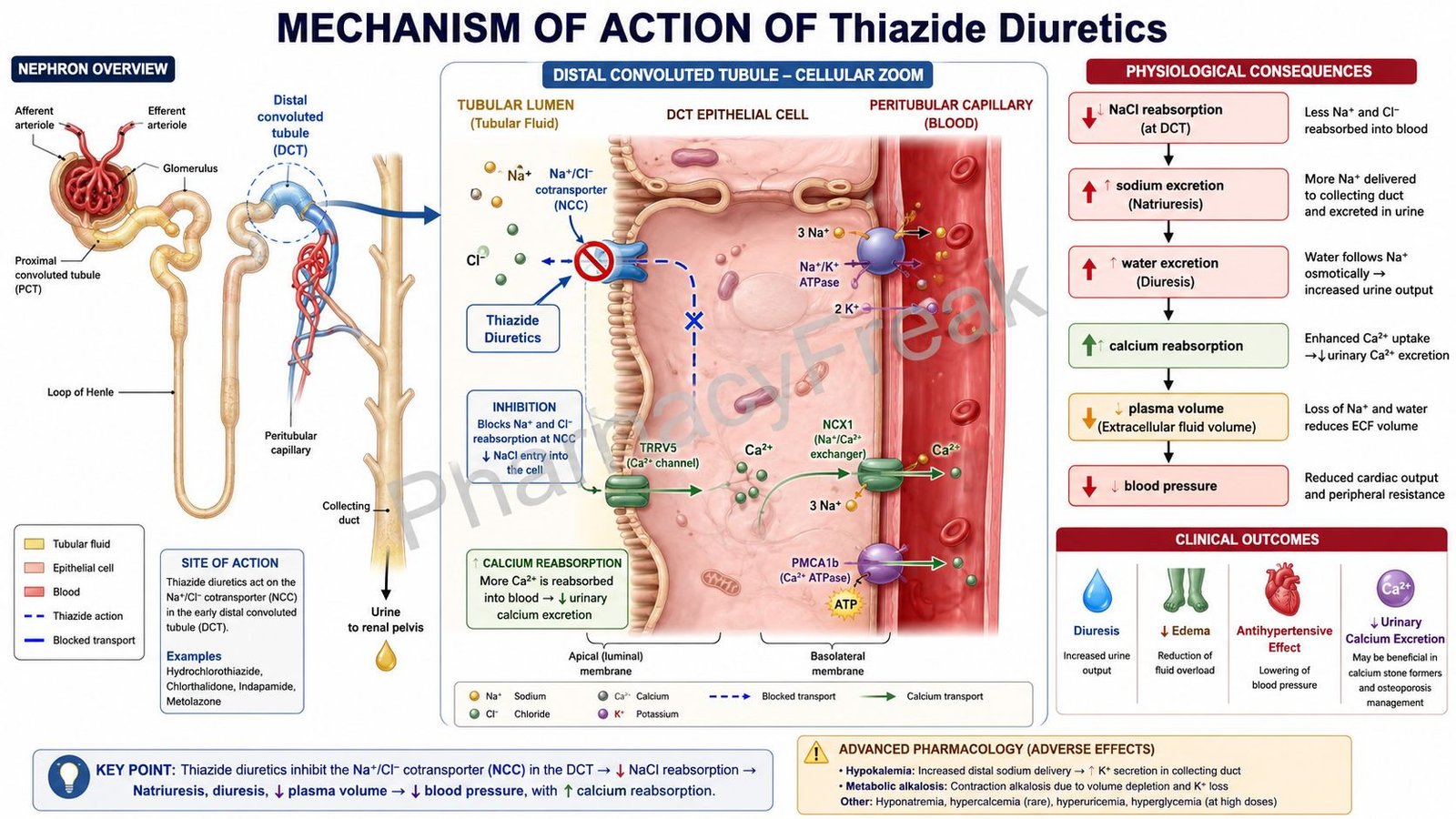
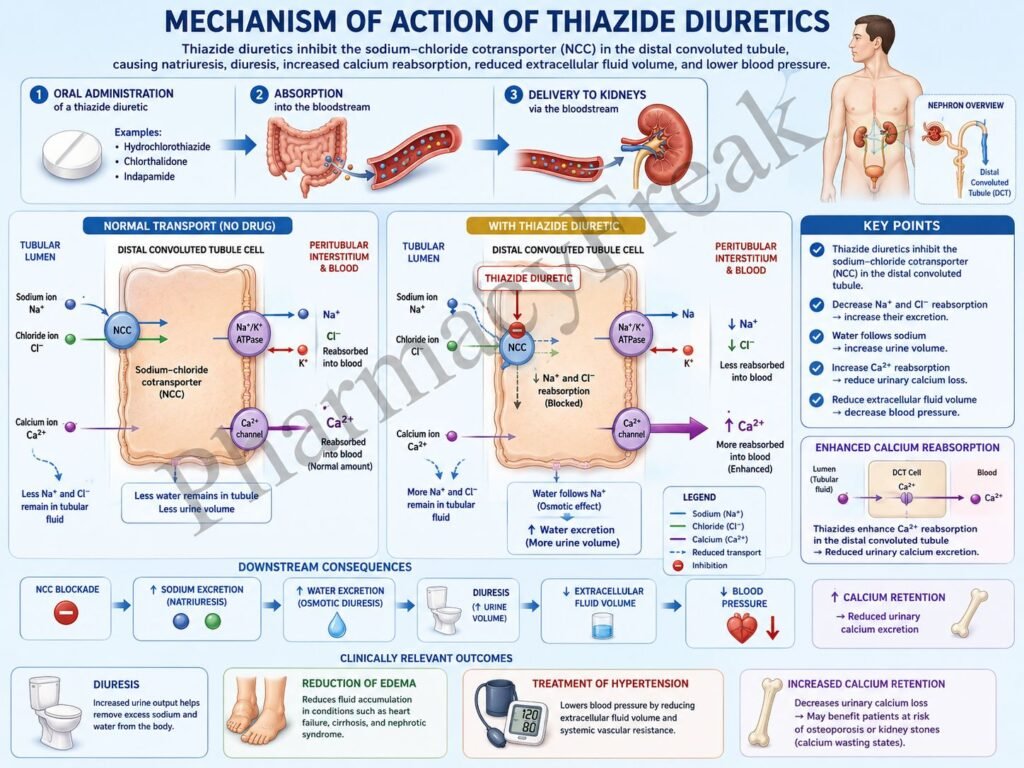
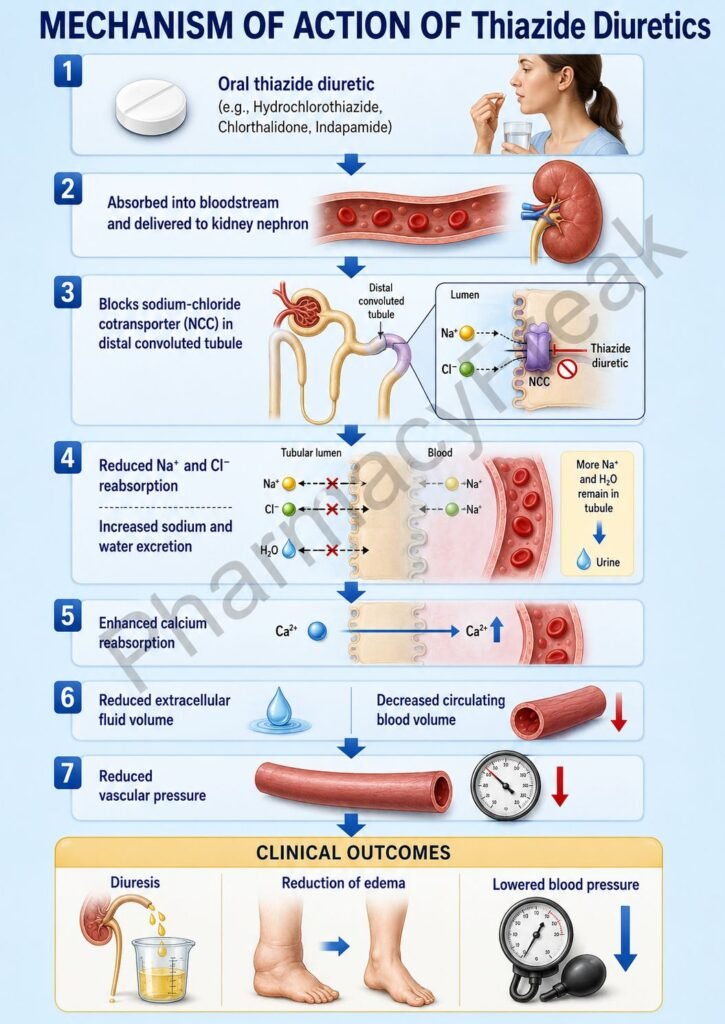
Thiazide diuretics are commonly used antihypertensive and diuretic agents that increase sodium and water excretion by inhibiting sodium reabsorption in the distal convoluted tubule (DCT) of the nephron. Common thiazide diuretics include hydrochlorothiazide, chlorothiazide, and bendroflumethiazide, while thiazide-like diuretics include chlorthalidone, indapamide, and metolazone. These drugs are widely used in hypertension, edema, heart failure, and prevention of calcium-containing kidney stones.
Mechanism of Action (Step-wise)
- Thiazide diuretics reach the kidneys through the bloodstream and are secreted into the renal tubules.
- They act primarily in the early distal convoluted tubule (DCT) of the nephron.
- In the DCT, sodium and chloride are normally reabsorbed through the sodium-chloride cotransporter (NCC).
- Thiazides selectively inhibit the Na⁺/Cl⁻ cotransporter.
- Sodium and chloride reabsorption decreases.
- Increased sodium and chloride remain within the tubular fluid.
- Water follows these electrolytes osmotically, increasing urine output.
- Plasma volume and extracellular fluid volume decrease.
- Cardiac output initially falls because of reduced circulating volume.
- With chronic therapy, peripheral vascular resistance decreases, contributing to long-term blood pressure reduction.
- Increased sodium delivery to the collecting duct promotes potassium and hydrogen ion excretion.
- Calcium reabsorption in the distal tubule increases, reducing urinary calcium excretion.
- The overall effect is diuresis, reduced blood pressure, and decreased edema.
A key exam point is that thiazide diuretics inhibit the Na⁺/Cl⁻ cotransporter in the distal convoluted tubule, increasing sodium and water excretion.
Pharmacokinetics
Thiazide diuretics are administered orally and are generally well absorbed. Most agents have durations ranging from 6 to 24 hours, while chlorthalidone has a longer duration of action. Elimination occurs primarily through renal excretion.
Clinical Uses
Thiazide diuretics are used in:
- Hypertension
- Mild to moderate edema
- Chronic heart failure
- Nephrogenic diabetes insipidus
- Calcium-containing kidney stone prevention
- Osteoporosis risk reduction (due to calcium retention)
Adverse Effects
Common adverse effects include:
- Hypokalemia
- Hyponatremia
- Hyperuricemia
- Hyperglycemia
- Hyperlipidemia
- Dizziness
Serious adverse effects may include:
- Severe electrolyte disturbances
- Cardiac arrhythmias secondary to hypokalemia
- Acute gout attacks
A useful exam mnemonic is “HyperGLUC”:
- HyperGlycemia
- HyperLipidemia
- HyperUricemia
- HyperCalcemia
Comparative Analysis
| Feature | Thiazide Diuretics | Loop Diuretics | Potassium-Sparing Diuretics |
|---|---|---|---|
| Main site of action | Distal convoluted tubule | Thick ascending limb | Collecting duct |
| Main target | Na⁺/Cl⁻ cotransporter | Na⁺/K⁺/2Cl⁻ cotransporter | Aldosterone receptor or ENaC |
| Potassium loss | Yes | Yes | No |
| Calcium excretion | Decreased | Increased | Minimal effect |
| Antihypertensive effect | Excellent | Moderate | Mild |
| Diuretic potency | Moderate | High | Low |
Thiazides differ from loop diuretics because they increase calcium reabsorption rather than calcium excretion. Compared with potassium-sparing diuretics, thiazides have greater antihypertensive efficacy but a higher risk of hypokalemia.
MCQs
1. Thiazide diuretics act primarily in the:
a) Proximal convoluted tubule
b) Loop of Henle
c) Distal convoluted tubule
d) Collecting duct
Answer: c) Distal convoluted tubule
2. Thiazides inhibit which transporter?
a) Na⁺/K⁺/2Cl⁻ cotransporter
b) Na⁺/Cl⁻ cotransporter
c) ENaC channel
d) Sodium-potassium ATPase
Answer: b) Na⁺/Cl⁻ cotransporter
3. The primary effect of thiazides is:
a) Increased sodium excretion
b) Increased glucose absorption
c) Increased potassium retention
d) Increased uric acid excretion
Answer: a) Increased sodium excretion
4. Thiazides are commonly used for:
a) Hypertension
b) Asthma
c) Parkinson disease
d) Peptic ulcer disease
Answer: a) Hypertension
5. A common electrolyte abnormality is:
a) Hyperkalemia
b) Hypokalemia
c) Hypermagnesemia
d) Hypernatremia
Answer: b) Hypokalemia
6. Thiazides affect urinary calcium by:
a) Increasing calcium excretion
b) Decreasing calcium excretion
c) Blocking calcium absorption completely
d) Having no effect
Answer: b) Decreasing calcium excretion
7. Which adverse effect is associated with thiazides?
a) Hyperuricemia
b) Hypoglycemia
c) Hyperkalemia
d) Bradycardia
Answer: a) Hyperuricemia
8. Which drug is a thiazide diuretic?
a) Furosemide
b) Spironolactone
c) Hydrochlorothiazide
d) Mannitol
Answer: c) Hydrochlorothiazide
9. Long-term antihypertensive effects are mainly due to:
a) Reduced peripheral vascular resistance
b) Increased cardiac output
c) Increased aldosterone secretion
d) Increased sympathetic activity
Answer: a) Reduced peripheral vascular resistance
10. Thiazides may worsen:
a) Gout
b) Asthma
c) Hypothyroidism
d) Peptic ulcer disease
Answer: a) Gout
11. Compared with loop diuretics, thiazides:
a) Cause more calcium loss
b) Increase calcium reabsorption
c) Have no calcium effect
d) Cause severe hypercalciuria
Answer: b) Increase calcium reabsorption
12. The antihypertensive action of thiazides results from:
a) Diuresis and reduced vascular resistance
b) β-receptor blockade
c) ACE inhibition
d) Calcium channel blockade
Answer: a) Diuresis and reduced vascular resistance
FAQs
What is the mechanism of action of thiazide diuretics?
Thiazide diuretics inhibit the Na⁺/Cl⁻ cotransporter in the distal convoluted tubule, increasing sodium and water excretion.
Why are thiazides effective in hypertension?
They initially reduce plasma volume and later decrease peripheral vascular resistance.
Do thiazides increase or decrease urinary calcium excretion?
They decrease urinary calcium excretion by increasing calcium reabsorption in the distal tubule.
What is the most common electrolyte abnormality caused by thiazides?
Hypokalemia.
Why can thiazides precipitate gout?
Because they increase serum uric acid levels by reducing urate excretion.
How do thiazides differ from loop diuretics?
Thiazides increase calcium reabsorption, whereas loop diuretics increase calcium excretion.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung’s Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi KD. Essentials of Medical Pharmacology
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com

