Table of Contents
Introduction
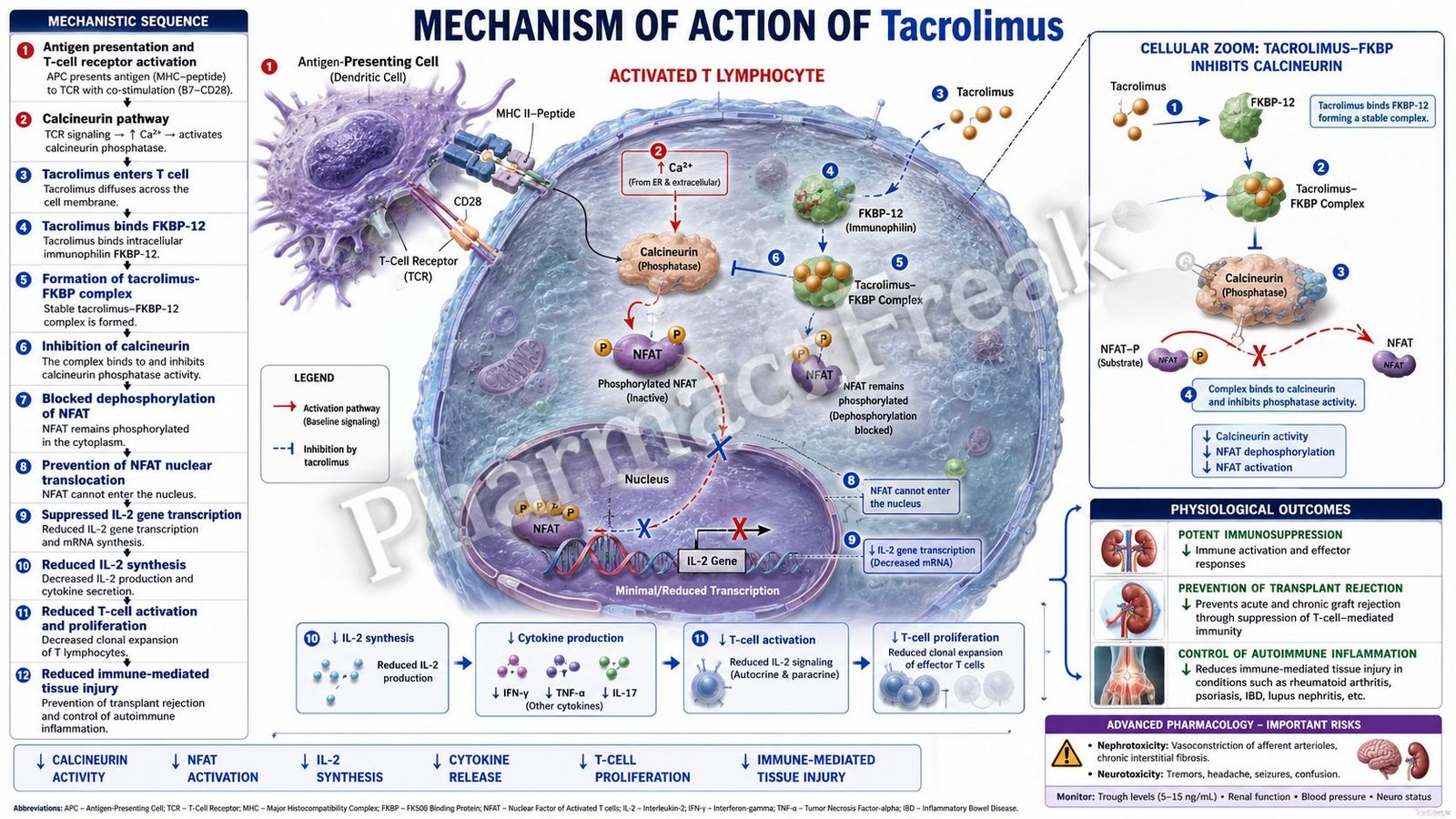
Tacrolimus is a potent immunosuppressive agent widely used in organ transplantation and autoimmune diseases. It belongs to the calcineurin inhibitor class and suppresses T-lymphocyte activation by inhibiting interleukin-2 (IL-2) production. Tacrolimus is more potent than cyclosporine and plays a crucial role in preventing graft rejection after organ transplantation.
Mechanism of Action (Step-wise)
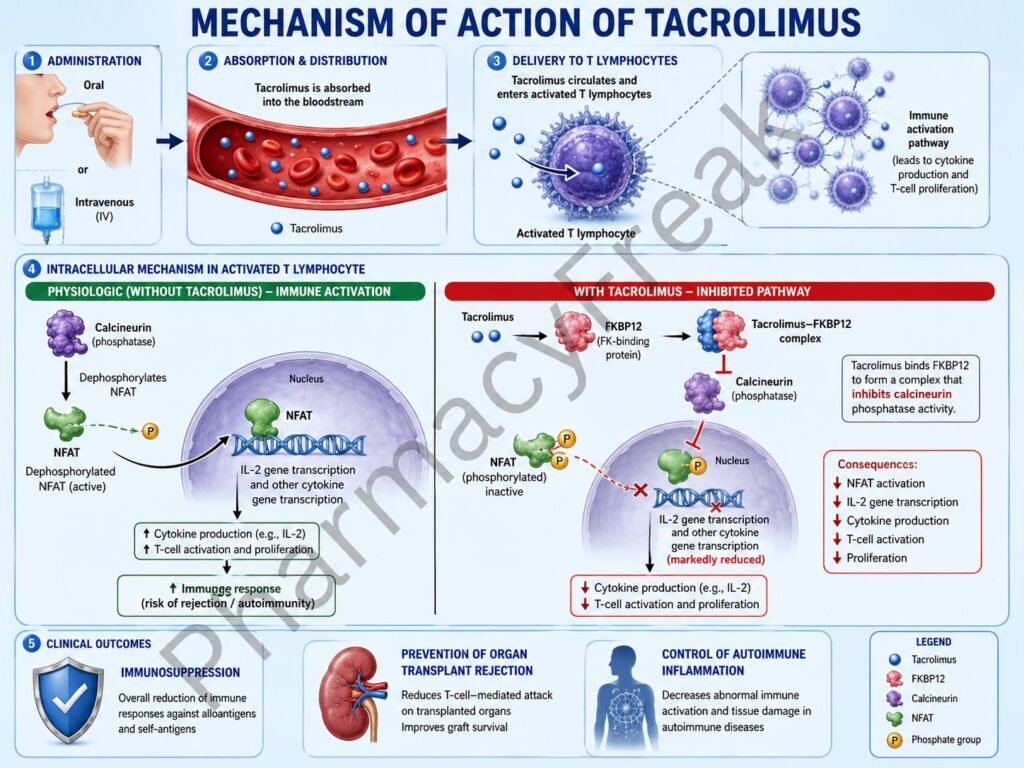
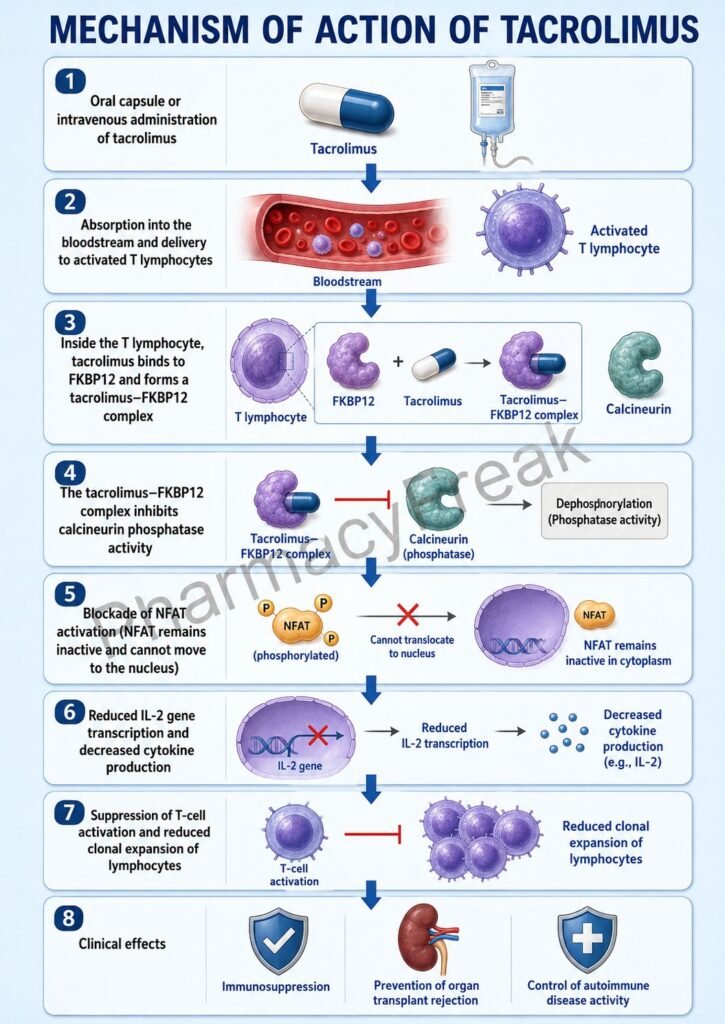
- Tacrolimus enters T lymphocytes after administration.
- Inside the cell, tacrolimus binds to an intracellular immunophilin known as FK-binding protein-12 (FKBP-12).
- The tacrolimus-FKBP12 complex is formed within the cytoplasm.
- This complex inhibits the enzyme calcineurin.
- Calcineurin normally dephosphorylates nuclear factor of activated T cells (NFAT).
- Dephosphorylated NFAT enters the nucleus and stimulates transcription of cytokine genes.
- Inhibition of calcineurin prevents NFAT activation and nuclear translocation.
- Transcription of interleukin-2 (IL-2) decreases significantly.
- Production of other cytokines such as IL-3, IL-4, TNF-α, and interferon-γ is also reduced.
- T-cell activation, proliferation, and differentiation are suppressed.
- Cell-mediated immune responses decrease.
- The overall effect is prevention of transplant rejection and suppression of autoimmune inflammation.
A key exam point is that tacrolimus binds FKBP-12 and inhibits calcineurin, preventing IL-2 transcription and T-cell activation.
Pharmacokinetics
Tacrolimus can be administered orally, intravenously, or topically. It is extensively metabolized by CYP3A4 in the liver and intestine. The drug has a narrow therapeutic index, requiring monitoring of blood concentrations. Elimination occurs mainly through bile.
Clinical Uses
Tacrolimus is used in:
- Kidney transplantation
- Liver transplantation
- Heart transplantation
- Lung transplantation
- Atopic dermatitis (topical formulation)
- Autoimmune disorders
- Graft-versus-host disease prophylaxis
Adverse Effects
Common adverse effects include:
- Nephrotoxicity
- Hypertension
- Tremors
- Headache
- Hyperglycemia
- Hyperkalemia
Serious adverse effects include:
- Neurotoxicity
- Opportunistic infections
- Malignancies due to immunosuppression
- New-onset diabetes after transplantation
Comparative Analysis
| Feature | Tacrolimus | Cyclosporine | Sirolimus |
|---|---|---|---|
| Binding protein | FKBP-12 | Cyclophilin | FKBP-12 |
| Main target | Calcineurin | Calcineurin | mTOR |
| IL-2 production | Decreased | Decreased | Not affected directly |
| T-cell activation | Inhibited | Inhibited | Inhibited indirectly |
| Nephrotoxicity | High | High | Lower |
| Potency | Higher | Lower | Different mechanism |
Tacrolimus differs from cyclosporine by binding FKBP-12 instead of cyclophilin, although both inhibit calcineurin. Compared with sirolimus, tacrolimus suppresses IL-2 production, whereas sirolimus blocks the cellular response to IL-2.
MCQs
1. Tacrolimus belongs to which class of immunosuppressants?
a) mTOR inhibitors
b) Calcineurin inhibitors
c) Antimetabolites
d) Corticosteroids
Answer: b) Calcineurin inhibitors
2. Tacrolimus binds to:
a) Cyclophilin
b) FKBP-12
c) Albumin
d) Calmodulin
Answer: b) FKBP-12
3. Tacrolimus inhibits:
a) mTOR
b) Calcineurin
c) Cyclooxygenase
d) Acetylcholinesterase
Answer: b) Calcineurin
4. Calcineurin normally activates:
a) NFAT
b) NF-κB only
c) STAT proteins only
d) Histamine receptors
Answer: a) NFAT
5. Tacrolimus decreases production of:
a) Insulin
b) IL-2
c) Thyroxine
d) Histamine
Answer: b) IL-2
6. Reduced IL-2 causes:
a) Increased T-cell proliferation
b) Decreased T-cell proliferation
c) Increased antibody synthesis only
d) Hyperglycemia
Answer: b) Decreased T-cell proliferation
7. Tacrolimus is commonly used in:
a) Organ transplantation
b) Asthma
c) Parkinson disease
d) Peptic ulcer disease
Answer: a) Organ transplantation
8. A major adverse effect is:
a) Nephrotoxicity
b) Hypercalcemia
c) Cataracts
d) Polycythemia
Answer: a) Nephrotoxicity
9. Tacrolimus is metabolized mainly by:
a) CYP2D6
b) CYP3A4
c) MAO
d) Xanthine oxidase
Answer: b) CYP3A4
10. Tacrolimus is more potent than:
a) Methotrexate
b) Cyclosporine
c) Azathioprine
d) Prednisone
Answer: b) Cyclosporine
11. Topical tacrolimus is commonly used in:
a) Atopic dermatitis
b) Psoriasis only
c) Acne vulgaris
d) Vitiligo only
Answer: a) Atopic dermatitis
12. The primary immunological effect of tacrolimus is:
a) Suppression of T-cell activation
b) Increased B-cell proliferation
c) Histamine blockade
d) Complement activation
Answer: a) Suppression of T-cell activation
FAQs
What is the mechanism of action of tacrolimus?
Tacrolimus binds FKBP-12 and inhibits calcineurin, preventing IL-2 production and T-cell activation.
Why is tacrolimus used after organ transplantation?
It suppresses immune responses that would otherwise attack the transplanted organ.
How does tacrolimus differ from cyclosporine?
Both inhibit calcineurin, but tacrolimus binds FKBP-12 whereas cyclosporine binds cyclophilin.
What is the major adverse effect of tacrolimus?
Nephrotoxicity.
Why are tacrolimus blood levels monitored?
Because the drug has a narrow therapeutic index and significant toxicity risk.
Can tacrolimus be used topically?
Yes, topical tacrolimus is used for atopic dermatitis and other inflammatory skin disorders.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung’s Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi KD. Essentials of Medical Pharmacology
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com

