Table of Contents
Introduction
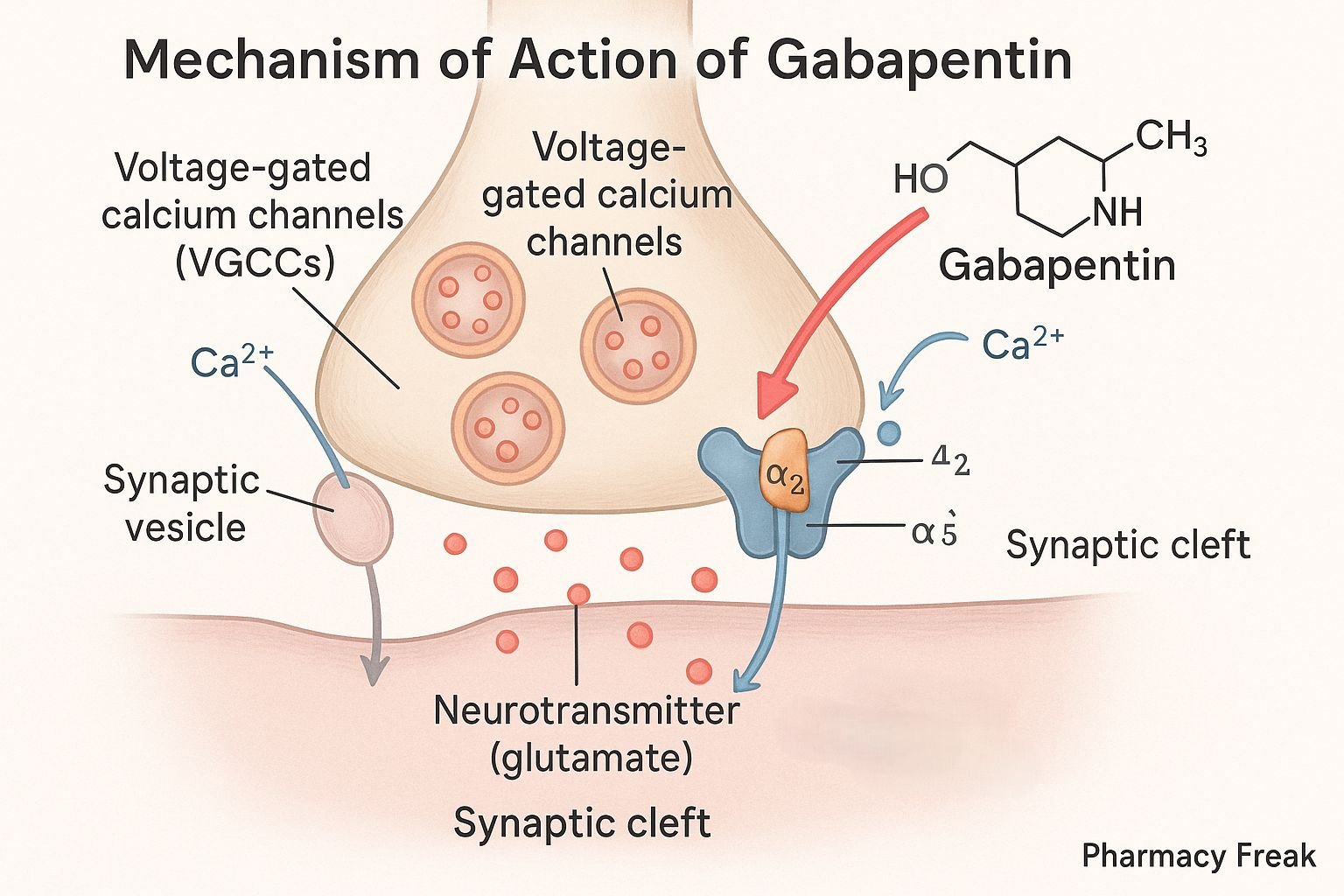
Gabapentin is an anticonvulsant and analgesic drug primarily used in the treatment of epilepsy, neuropathic pain, and restless legs syndrome. Though structurally related to gamma-aminobutyric acid (GABA), gabapentin does not bind to GABA receptors or influence GABA metabolism. Instead, it modulates neuronal excitability by interacting with voltage-gated calcium channels. Its favorable safety profile and broad therapeutic application make it a valuable drug in neurology and pain management.
Step-by-Step Mechanism of Action
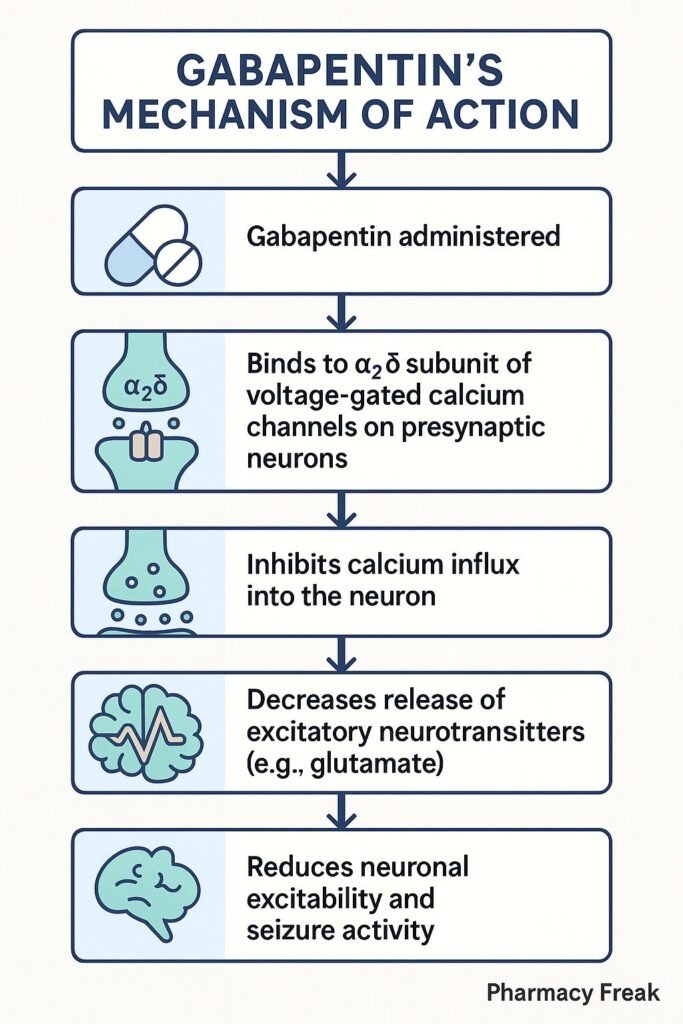
- Binding Site Identification: Gabapentin binds with high affinity to the alpha-2-delta (α2δ) subunit of voltage-gated calcium channels (VGCCs), especially the P/Q-type channels.
- Inhibition of Calcium Influx: By binding to the α2δ subunit, gabapentin reduces the influx of calcium ions into presynaptic neurons upon depolarization.
- Reduction of Neurotransmitter Release: The reduced calcium entry leads to decreased release of excitatory neurotransmitters such as glutamate, norepinephrine, and substance P.
- Attenuation of Neuronal Hyperexcitability: This modulation of neurotransmitter release reduces neuronal excitability, which contributes to its anticonvulsant and analgesic effects.
- Delayed Onset of Action: Gabapentin requires repeated dosing to reach effective concentrations in the CNS, where it accumulates over time.
Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Absorption | Non-linear, saturable |
| Bioavailability | ~60% (300 mg), decreases with dose |
| Tmax | 2 to 3 hours |
| Half-life | 5 to 7 hours |
| Protein binding | <3% |
| Metabolism | Not significantly metabolized |
| Excretion | Renal (unchanged drug) |
Clinical Uses
- Partial seizures (adjunctive therapy)
- Postherpetic neuralgia
- Diabetic neuropathy
- Fibromyalgia
- Restless legs syndrome
- Off-label uses include migraine prophylaxis and anxiety disorders
Adverse Effects
- Somnolence
- Dizziness
- Ataxia
- Peripheral edema
- Fatigue
- Weight gain
- Behavioral changes (rare)
Comparative Analysis
Gabapentin vs Pregabalin:
- Both bind to α2δ subunits of VGCCs.
- Pregabalin has more predictable pharmacokinetics and higher bioavailability.
- Gabapentin is often less expensive and used when cost is a concern.
MCQs
1. What is the primary site of action for gabapentin? a) GABA receptors
b) Sodium channels
c) Alpha-2-delta subunit of VGCCs
d) NMDA receptors
2. Gabapentin reduces the release of which neurotransmitter? a) Dopamine
b) Glutamate
c) Acetylcholine
d) Serotonin
3. Gabapentin is structurally similar to: a) Glycine
b) Serotonin
c) GABA
d) Histamine
4. What is the primary route of excretion for gabapentin? a) Hepatic
b) Fecal
c) Pulmonary
d) Renal
5. Which of the following is an approved indication for gabapentin? a) Generalized seizures
b) Postherpetic neuralgia
c) Schizophrenia
d) Hypertension
6. Which of the following is NOT a side effect of gabapentin? a) Ataxia
b) Somnolence
c) Hepatotoxicity
d) Peripheral edema
7. Gabapentin is best described pharmacokinetically as: a) Highly protein-bound
b) Hepatically metabolized
c) Non-linear absorption
d) Long half-life (>24 hours)
8. Pregabalin differs from gabapentin in that it: a) Binds to sodium channels
b) Is more expensive
c) Is less bioavailable
d) Is not used for neuropathic pain
9. Gabapentin is often used off-label for: a) Hyperlipidemia
b) Asthma
c) Anxiety
d) GERD
10. Gabapentin’s mechanism involves: a) Increasing GABA synthesis
b) Blocking GABA reuptake
c) Modulating VGCC activity
d) Inhibiting monoamine oxidase
FAQs
1. Is gabapentin a GABA agonist?
No, despite its structural similarity, it does not act directly on GABA receptors.
2. Can gabapentin be used for anxiety?
Yes, although off-label, it is sometimes used for anxiety disorders.
3. Is gabapentin safe in renal impairment?
Dose adjustment is required in renal impairment due to its renal excretion.
4. How long does it take for gabapentin to work?
It may take a few days to a few weeks to observe its full therapeutic effect.
5. Can gabapentin cause dependence?
It has a low potential for dependence but should be discontinued gradually.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition.
- KD Tripathi. Essentials of Medical Pharmacology, 8th Edition.
- https://pubmed.ncbi.nlm.nih.gov/11386498/
- https://pubmed.ncbi.nlm.nih.gov/14680413/


