Table of Contents
Introduction
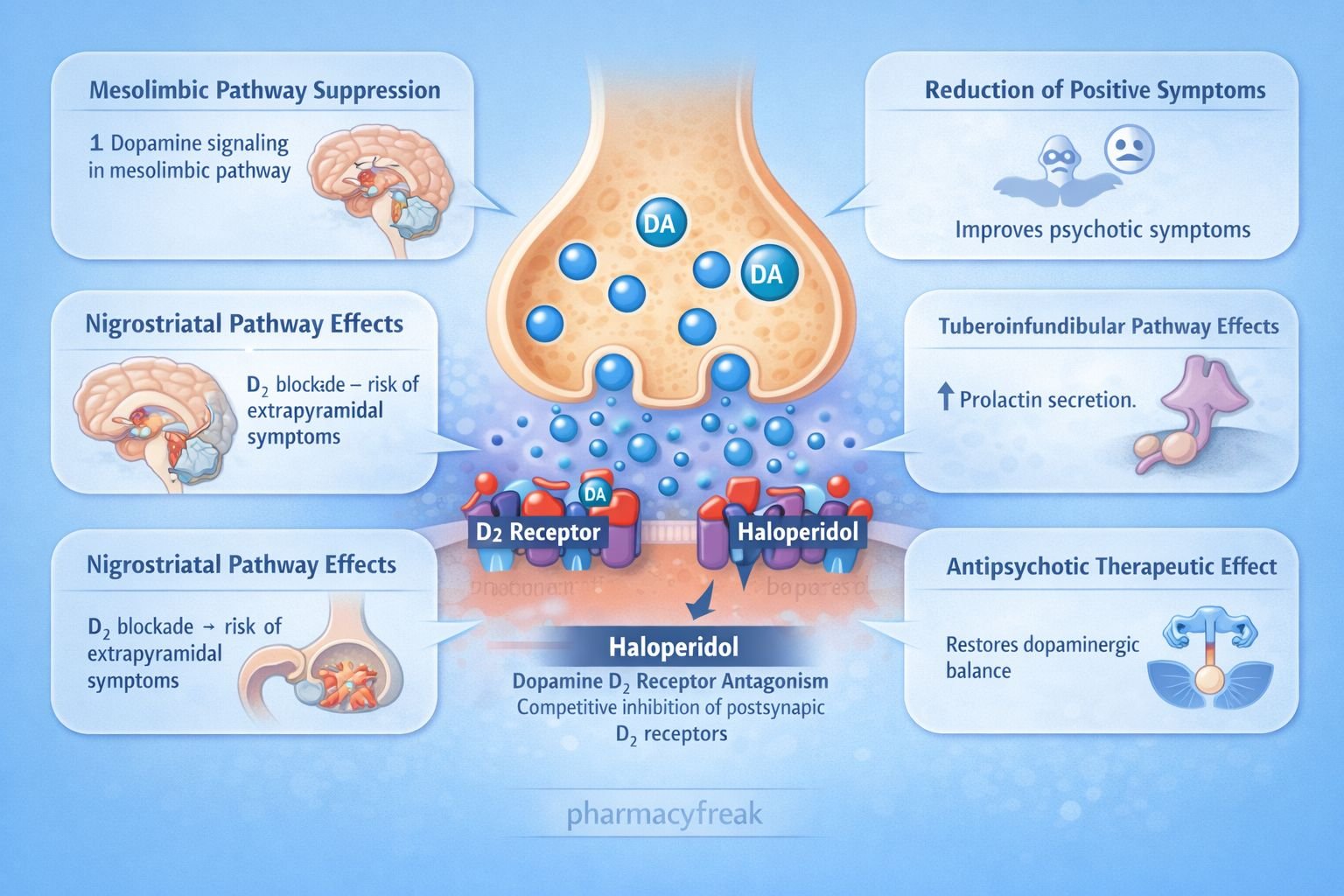
Haloperidol is a first generation (typical) antipsychotic belonging to the butyrophenone class. It is widely used in the treatment of schizophrenia, acute psychosis, delirium, and severe agitation. Haloperidol primarily works by blocking dopamine receptors in the central nervous system, particularly in the mesolimbic pathway.
Because excessive dopamine activity in the mesolimbic pathway is associated with psychotic symptoms such as hallucinations and delusions, dopamine receptor blockade helps control these symptoms. However, dopamine blockade in other pathways leads to adverse effects such as extrapyramidal symptoms.
Haloperidol’s mechanism is an important topic in pharmacology examinations such as USMLE, NEET PG, FMGE, PLAB, INICET, NCLEX, and MCCQE.
Mechanism of Action (Step-wise)
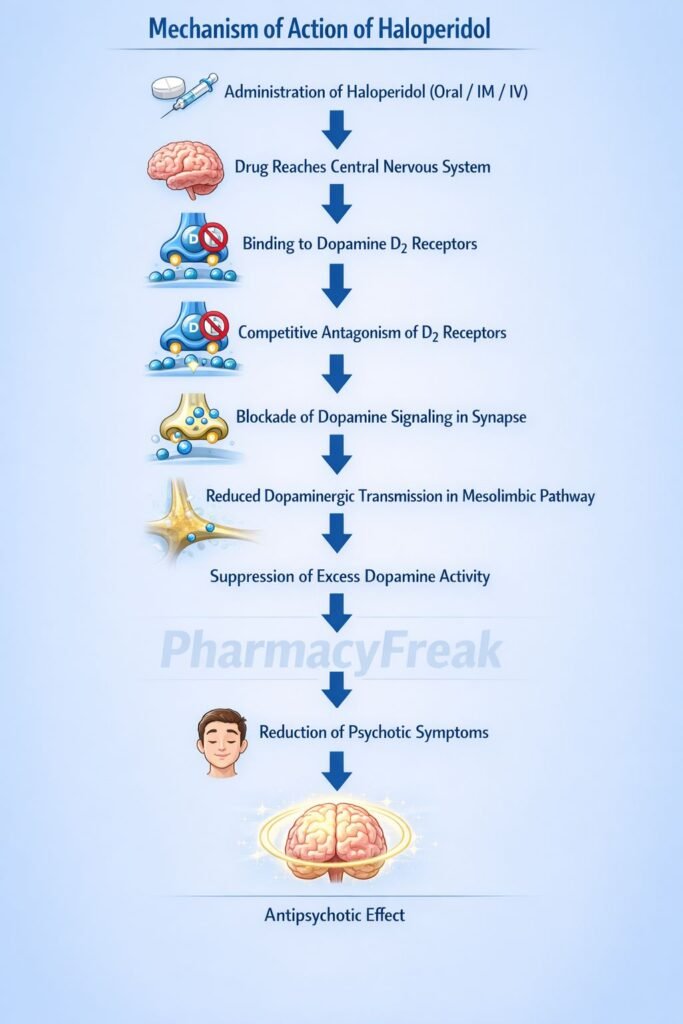
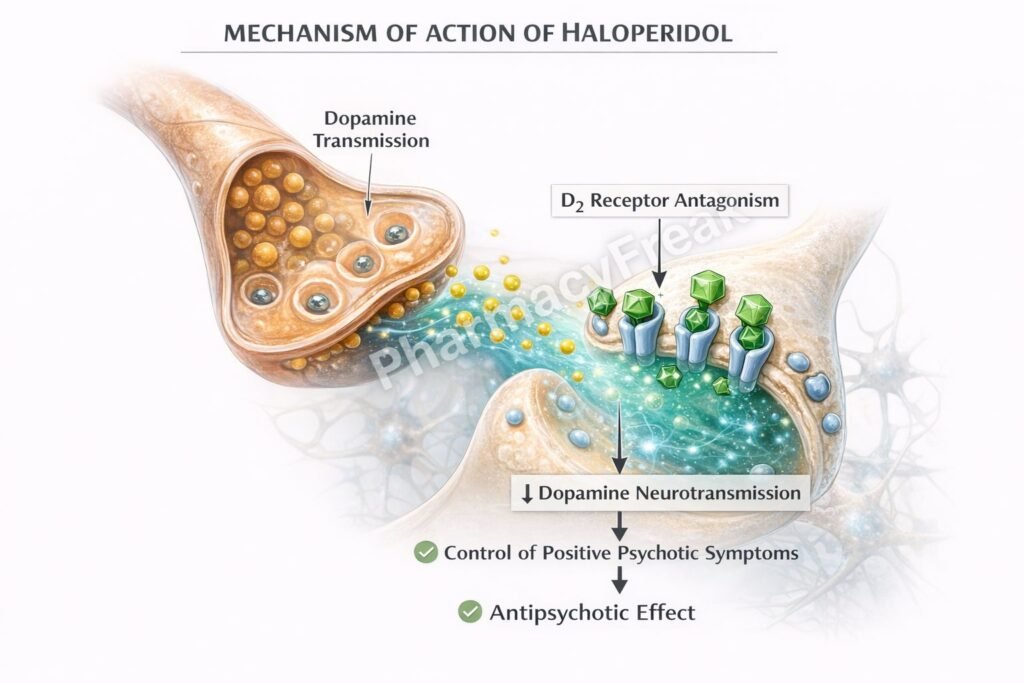
Haloperidol produces antipsychotic effects mainly through dopamine receptor antagonism.
Step 1: Dopamine receptor blockade
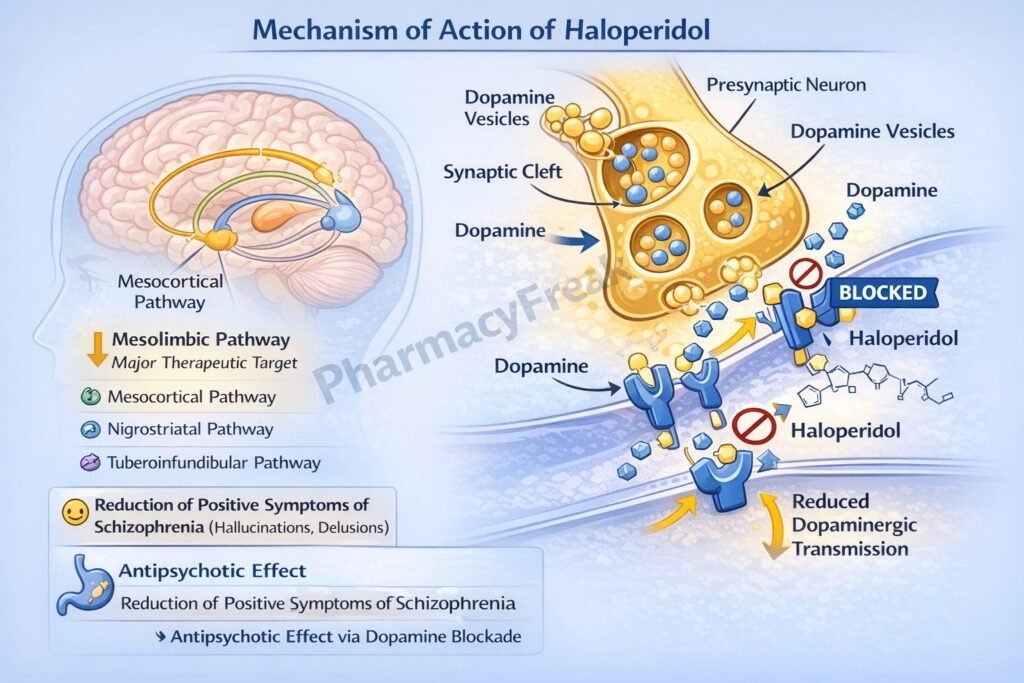
Haloperidol acts as a strong antagonist of dopamine D2 receptors in the central nervous system.
Step 2: Action in mesolimbic pathway
Blocking D2 receptors in the mesolimbic pathway reduces excessive dopamine signaling associated with positive symptoms of schizophrenia.
Step 3: Reduction of psychotic symptoms
Decreased dopamine transmission reduces hallucinations, delusions, and agitation.
Step 4: Effects in other dopaminergic pathways
Nigrostriatal pathway
D2 blockade interferes with dopamine mediated motor control, causing extrapyramidal symptoms.
Tuberoinfundibular pathway
D2 blockade increases prolactin secretion due to loss of dopamine inhibition.
Mesocortical pathway
Dopamine blockade may contribute to worsening of negative symptoms.
Step 5: Additional receptor effects
Haloperidol also has minor activity at alpha adrenergic and muscarinic receptors, although much weaker compared to other antipsychotics.
Overall effect:
Reduction of psychotic symptoms through central dopamine D2 receptor antagonism.
Important pharmacology concept:
Typical antipsychotics like haloperidol strongly block D2 receptors and therefore have a higher risk of extrapyramidal side effects.
Pharmacokinetics
Absorption:
Well absorbed after oral administration.
Distribution:
Highly lipophilic and widely distributed in brain tissues.
Metabolism:
Metabolized primarily in the liver through CYP3A4 and CYP2D6 enzymes.
Excretion:
Eliminated through urine and bile as metabolites.
Half life:
Approximately 12 to 36 hours.
Haloperidol is available in oral, intramuscular, and long acting depot formulations.
Clinical Uses
- Schizophrenia
- Acute psychosis and agitation
- Delirium in hospitalized patients
- Tourette syndrome
- Severe behavioral disturbances
It is also used in emergency settings to control severe agitation.
Adverse Effects
Common adverse effects:
- Extrapyramidal symptoms (EPS)
- Sedation
- Anticholinergic effects
Extrapyramidal symptoms include:
- Acute dystonia
- Parkinsonism
- Akathisia
- Tardive dyskinesia
Serious adverse effects:
- Neuroleptic malignant syndrome
- Hyperprolactinemia
- QT interval prolongation
Comparative Analysis
| Feature | Haloperidol | Clozapine | Risperidone |
|---|---|---|---|
| Drug class | Typical antipsychotic | Atypical antipsychotic | Atypical antipsychotic |
| Primary receptor | D2 antagonist | D4 and 5-HT2A blockade | D2 and 5-HT2A blockade |
| EPS risk | High | Very low | Moderate |
| Prolactin elevation | Common | Rare | Moderate |
| Major use | Acute psychosis | Resistant schizophrenia | Schizophrenia |
Explanation:
Haloperidol is a high potency typical antipsychotic that strongly blocks D2 receptors. Clozapine is an atypical antipsychotic with strong serotonin receptor blockade and minimal extrapyramidal side effects. Risperidone has combined dopamine and serotonin receptor antagonism and is widely used in schizophrenia with fewer motor side effects than typical antipsychotics.
MCQs
- Haloperidol primarily blocks which receptor?
a) Serotonin 5-HT2A
b) Dopamine D2
c) Histamine H1
d) Muscarinic M3
Answer: b) Dopamine D2
- Antipsychotic effects of haloperidol occur mainly in the:
a) Mesolimbic pathway
b) Nigrostriatal pathway
c) Tuberoinfundibular pathway
d) Hypothalamus
Answer: a) Mesolimbic pathway
- Extrapyramidal symptoms occur due to dopamine blockade in:
a) Mesolimbic pathway
b) Mesocortical pathway
c) Nigrostriatal pathway
d) Tuberoinfundibular pathway
Answer: c) Nigrostriatal pathway
- Increased prolactin secretion results from dopamine blockade in:
a) Mesolimbic pathway
b) Tuberoinfundibular pathway
c) Nigrostriatal pathway
d) Cortical pathway
Answer: b) Tuberoinfundibular pathway
- Haloperidol belongs to which drug class?
a) Atypical antipsychotic
b) Typical antipsychotic
c) Antidepressant
d) Mood stabilizer
Answer: b) Typical antipsychotic
- A serious adverse effect associated with antipsychotics is:
a) Neuroleptic malignant syndrome
b) Hypothyroidism
c) Hyperkalemia
d) Renal failure
Answer: a) Neuroleptic malignant syndrome
- Which symptom is considered an extrapyramidal effect?
a) Dystonia
b) Hyperglycemia
c) Hypertension
d) Tachycardia
Answer: a) Dystonia
- Dopamine blockade reduces which symptoms of schizophrenia?
a) Positive symptoms
b) Negative symptoms
c) Cognitive symptoms
d) Metabolic symptoms
Answer: a) Positive symptoms
- Haloperidol metabolism occurs mainly in the:
a) Kidney
b) Liver
c) Lung
d) Intestine
Answer: b) Liver
- Hyperprolactinemia occurs due to inhibition of:
a) Serotonin
b) Dopamine
c) Histamine
d) Acetylcholine
Answer: b) Dopamine
FAQs
- How does haloperidol treat schizophrenia?
By blocking dopamine D2 receptors and reducing excessive dopamine activity in the mesolimbic pathway. - Why does haloperidol cause extrapyramidal symptoms?
Because dopamine blockade in the nigrostriatal pathway interferes with normal motor control. - What is neuroleptic malignant syndrome?
A rare but life threatening reaction characterized by muscle rigidity, hyperthermia, and autonomic instability. - Why does haloperidol increase prolactin levels?
Dopamine normally inhibits prolactin release, so blocking dopamine receptors increases prolactin secretion. - Is haloperidol a typical or atypical antipsychotic?
It is a typical (first generation) antipsychotic. - Can haloperidol be used for acute agitation?
Yes, it is commonly used in emergency settings for severe agitation and psychosis.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookID=2189
Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookID=2249
Tripathi KD. Essentials of Medical Pharmacology
https://jaypeedigital.com/book/9789354651970
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookID=3095


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com