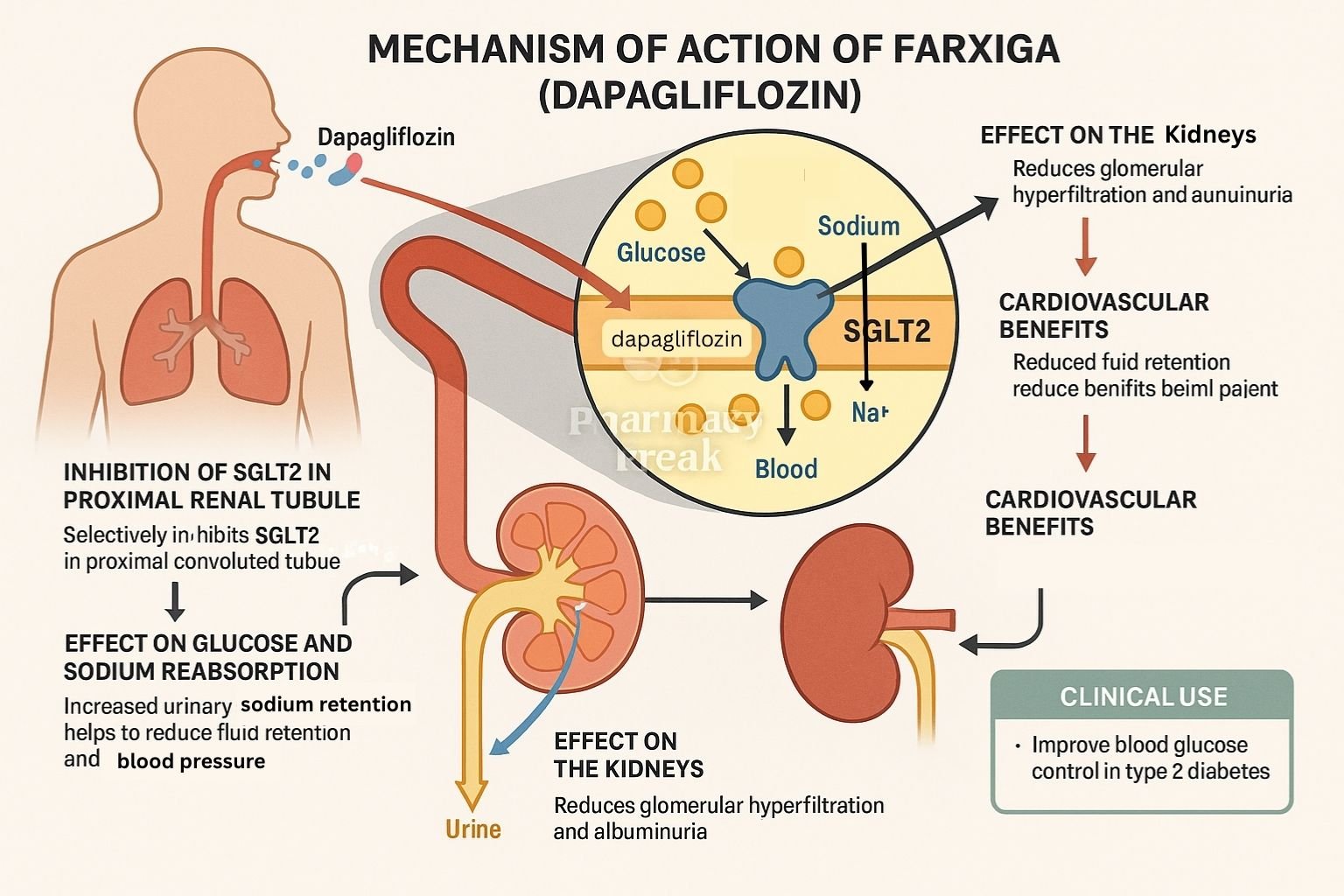
Dapagliflozin (trade name Farxiga) is a sodium–glucose co‑transporter 2 (SGLT2) inhibitor used in type 2 diabetes mellitus (T2DM) and heart failure with reduced ejection fraction (HFrEF). It lowers blood glucose by promoting renal excretion of glucose and also provides cardiovascular and renal benefits beyond glycemic control.
Step-by-Step Mechanism of Action
Selective inhibition of SGLT2 in proximal renal tubule Dapagliflozin blocks the SGLT2 protein in the kidneys, reducing reabsorption of filtered glucose and sodium.
Increased urinary glucose excretion (UGE) Inhibition leads to excretion of 60–80 g of glucose per day, lowering plasma glucose and HbA₁c.
Osmotic diuresis and natriuresis Glucosuria draws water into the urine; concurrent sodium loss lowers plasma volume, blood pressure, and preload.
Weight loss and metabolic effects Caloric loss from glucosuria leads to weight reduction. Improved insulin sensitivity and cardiovascular outcomes follow.
Renoprotective and cardioprotective actions Mechanisms include reduced intraglomerular pressure, decreased albuminuria, and improved heart function via reduced preload, afterload, and energy utilization enhancement.
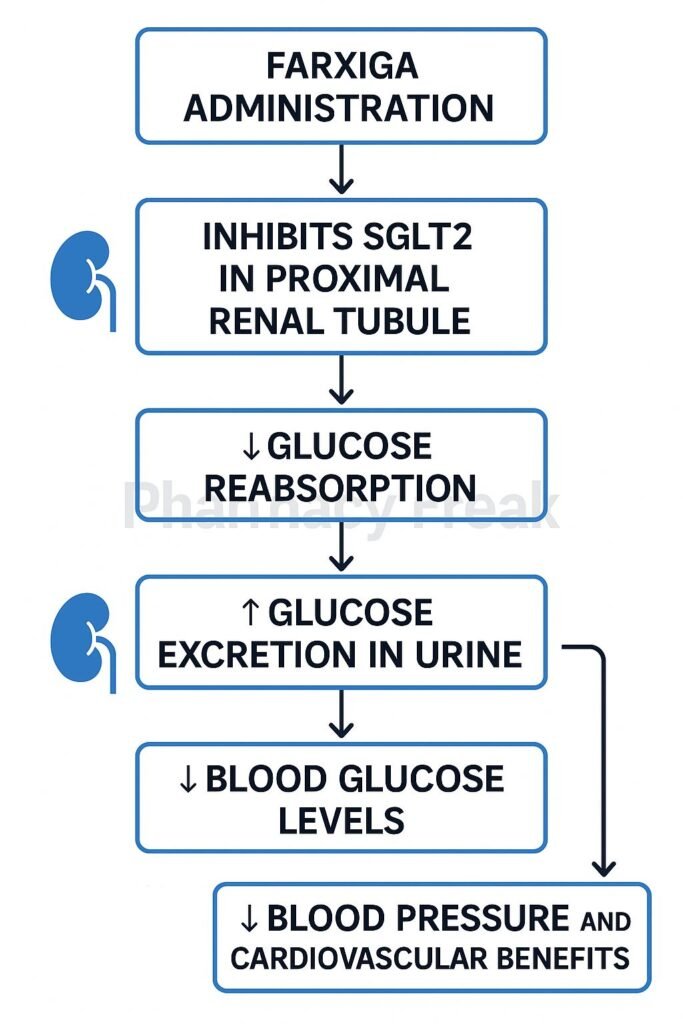
Mechanism of Action of farxiga flowchart
Pharmacokinetic Parameters
Parameter
Value
Route
Oral (tablet)
Bioavailability
~78%
Time to Peak (Tmax)
~2 hours
Protein Binding
~91%
Metabolism
Hepatic via UGT1A9 to inactive glucuronide
Half-life
~12–13 hours
Excretion
~75% renal (mostly unchanged), rest fecal
Clinical Uses
Glycemic control in type 2 diabetes
Reduces risk of cardiovascular death and hospitalization in HFrEF (with or without diabetes)
Slows progression of chronic kidney disease (CKD)
Adverse Effects
Genitourinary infections: mycotic vaginal and urinary tract infections
Volume depletion: hypotension, dizziness, especially in elderly or those on diuretics
Euglycemic diabetic ketoacidosis (rare)
Electrolyte changes: mild increases in LDL cholesterol and magnesium, possible slight potassium changes
Comparative Analysis
Drug
SGLT selectivity
HbA₁c Reduction
Weight Loss
Cardiorenal Benefit
Dapagliflozin
SGLT2 > SGLT1
0.5–1.0%
2–3 kg
Yes
Canagliflozin
SGLT2 ≈ SGLT1
0.8–1.1%
2.5–3.5 kg
Yes
Empagliflozin
High SGLT2
0.7–1.0%
2–3 kg
Yes
MCQs (15)
Dapagliflozin primarily inhibits which transporter? a) SGLT1 b) SGLT2 c) GLUT4 d) Na⁺/K⁺ ATPase Answer: b) SGLT2
Its glucose-lowering effect is due to: a) Enhanced insulin release b) Renal glucose excretion c) Intestinal glucose absorption blockade d) Hepatic gluconeogenesis inhibition Answer: b) Renal glucose excretion
Usual urinary glucose loss per day is around: a) 10 g b) 30 g c) 60–80 g d) 100 g Answer: c) 60–80 g
Common genitourinary side effect is: a) Pharyngitis b) Vaginal yeast infection c) Otitis media d) Dental caries Answer: b) Vaginal yeast infection
Dapagliflozin acts on which part of the nephron? a) Proximal tubule b) Loop of Henle c) Distal tubule d) Collecting duct Answer: a) Proximal tubule
Its effects on blood pressure are due to: a) Beta-blockade b) Natriuresis c) Vasodilation d) Calcium channel blockade Answer: b) Natriuresis
Rare but serious risk is: a) Lactic acidosis b) Euglycemic DKA c) Hyperthyroidism d) Bladder cancer Answer: b) Euglycemic DKA
Dapagliflozin metabolism occurs via: a) CYP3A4 b) UGT1A9 c) CYP2C9 d) Renal CYP enzymes Answer: b) UGT1A9
Protein binding is approximately: a) 50% b) 70% c) 91% d) 100% Answer: c) 91%
Weight loss is mainly due to: a) Appetite suppression b) Glucosuria and caloric loss c) Lipid malabsorption d) Increased exercise tolerance Answer: b) Glucosuria and caloric loss
A comparative SGLT2 inhibitor with similar benefit is: a) Metformin b) Sitagliptin c) Empagliflozin d) Liraglutide Answer: c) Empagliflozin
Primary route of elimination: a) Renal unchanged b) Biliary conjugates c) Fecal d) Pulmonary exhalation Answer: a) Renal unchanged
Dapagliflozin should be used with caution in patients with: a) CKD stage 3‑4 b) Hypothyroidism c) Liver cirrhosis d) Gastroenteritis Answer: a) CKD stage 3‑4
Electrolyte change may include mild: a) Hypomagnesemia b) Hyperkalemia c) Hypernatremia d) Hypocalcemia Answer: a) Hypomagnesemia
Dapagliflozin also reduces: a) LDL cholesterol b) Triglycerides c) Cardiovascular death & HF hospitalization d) Platelet aggregation Answer: c) Cardiovascular death & HF hospitalization
FAQs
Is dapagliflozin effective in non-diabetic heart failure? Yes—it reduces hospitalization for HFrEF even in non-diabetic patients.
How often should renal function be monitored? Monitor eGFR at baseline and periodically, especially in CKD patients.
Can it cause hypotension? Yes, especially in elderly or volume-depleted individuals; monitor blood pressure.
Does it cause hypoglycemia? Unlikely when used alone; risk increases when combined with insulin or sulfonylureas.
Is dapagliflozin safe with ACE inhibitors or ARBs? Yes—often used together for cardiorenal protection.
Pharmacy Freak Editorial Team is the official editorial voice of PharmacyFreak.com, dedicated to creating high-quality educational resources for healthcare learners. Our team publishes and reviews exam preparation content across pharmacy, nursing, coding, social work, and allied health topics, with a focus on practice questions, study guides, concept-based learning, and practical academic support. We combine subject research, structured editorial review, and clear presentation to make difficult topics more accessible, accurate, and useful for learners preparing for exams and professional growth.
Harsh Singh Rajput is a pharmacist currently working at ESIC and holds an MBA in Pharmaceutical Management from NIPER Hyderabad. He has a strong academic record with top ranks in national-level pharmacy exams, including AIR 61 in NIPER 2024 (MS/M.Pharm), AIR 27 in NIPER MBA, AIR 147 in GPAT 2024, AIR 907 in GPAT 2023, and AIR 6 in AIIMS CRE-2025 for Drug Store Keeper. At PharmacyFreak.com, he contributes expert content, exam strategies, and practical guidance for future pharmacists.
Mail- harsh@pharmacyfreak.com