
Table of Contents
Introduction
Hydroxychloroquine is an antimalarial drug that also possesses significant immunomodulatory and anti-inflammatory properties. It is widely used in the treatment of malaria as well as autoimmune diseases such as systemic lupus erythematosus (SLE) and rheumatoid arthritis.
Hydroxychloroquine acts primarily by interfering with lysosomal activity and antigen presentation in immune cells. It also affects Toll-like receptor signaling and intracellular parasite metabolism. These actions reduce immune activation and inflammatory responses.
Because of its dual role in infectious diseases and autoimmune disorders, hydroxychloroquine is an important topic in pharmacology examinations such as USMLE, NEET PG, FMGE, PLAB, INICET, NCLEX, and MCCQE.
Mechanism of Action (Step-wise)
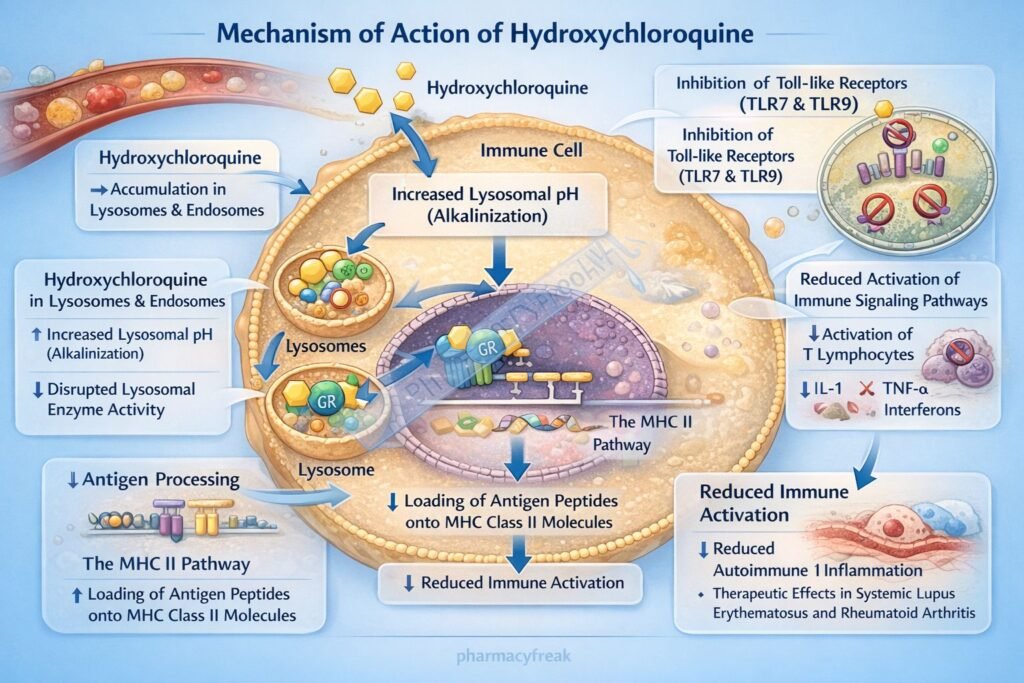
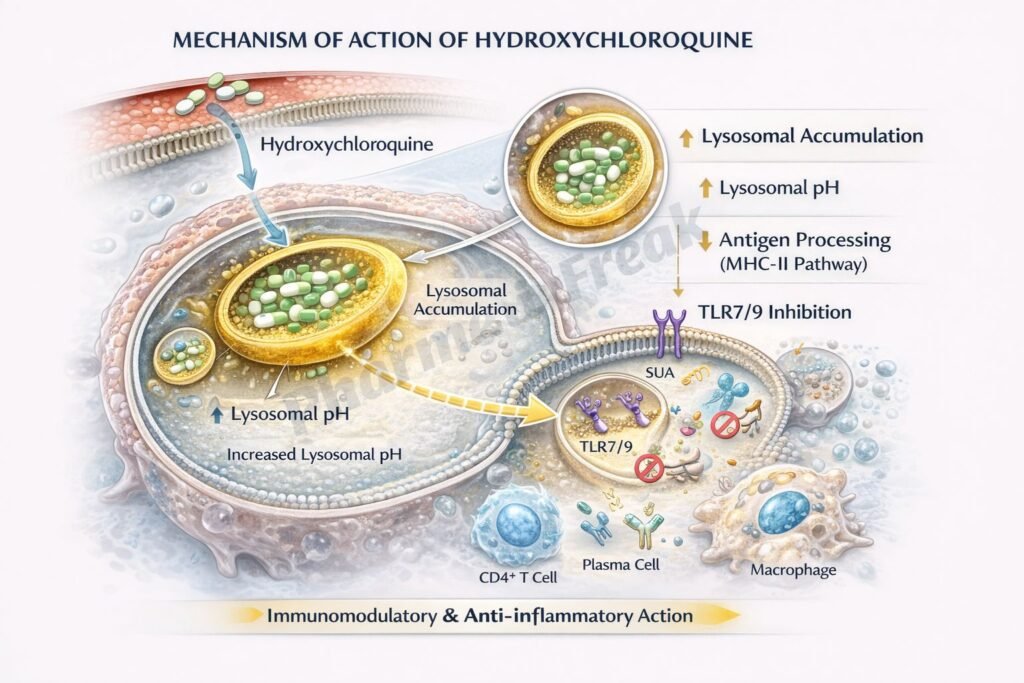
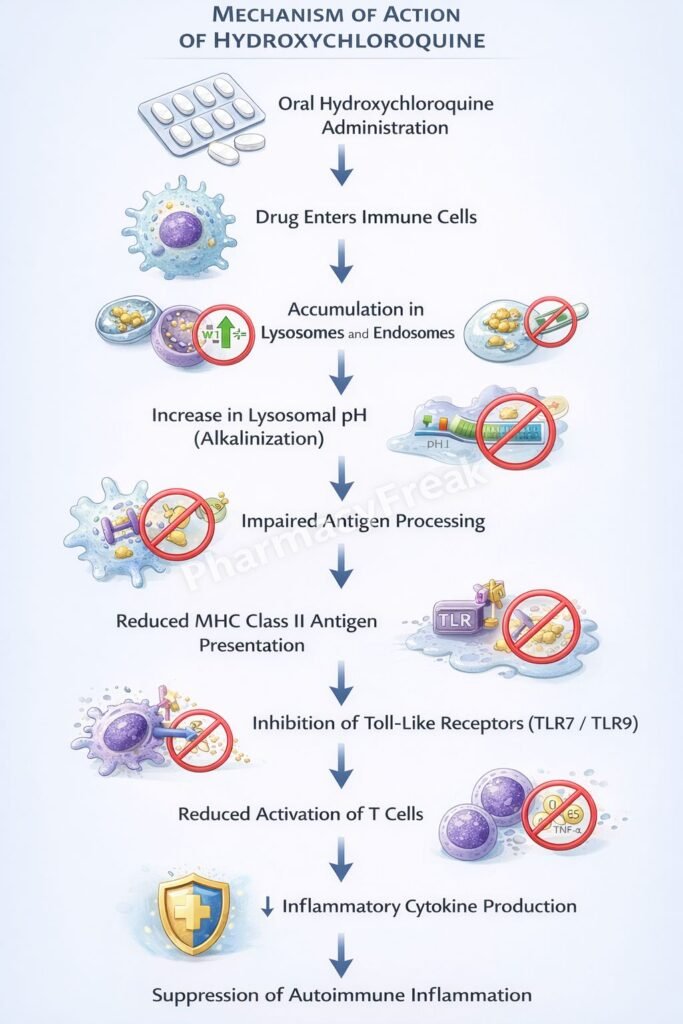
Hydroxychloroquine exerts antimalarial and immunomodulatory effects through multiple intracellular mechanisms.
Step 1: Accumulation in lysosomes
Hydroxychloroquine is a weak base that accumulates in acidic intracellular organelles such as lysosomes.
Step 2: Increase in lysosomal pH
Accumulation of the drug raises lysosomal pH and interferes with lysosomal enzyme activity.
Step 3: Impaired antigen processing
Higher lysosomal pH disrupts antigen processing and presentation by antigen-presenting cells.
Step 4: Inhibition of Toll-like receptor signaling
Hydroxychloroquine inhibits Toll-like receptors (TLR7 and TLR9), reducing activation of dendritic cells and inflammatory cytokine production.
Step 5: Reduced immune activation
Suppression of cytokine production decreases inflammatory responses in autoimmune diseases.
Step 6: Antimalarial activity
In malaria parasites, hydroxychloroquine interferes with heme detoxification within the parasite’s food vacuole, leading to accumulation of toxic heme and parasite death.
Overall effect:
Reduced immune activation and inhibition of parasite survival.
Important pharmacology concept:
Hydroxychloroquine modifies immune cell signaling rather than directly suppressing immune cell proliferation like many immunosuppressants.
Pharmacokinetics
Absorption:
Well absorbed after oral administration.
Distribution:
Extensively distributed in tissues including liver, spleen, lungs, and melanin-containing tissues such as retina.
Metabolism:
Partially metabolized in the liver.
Excretion:
Eliminated mainly through renal excretion.
Half life:
Long half-life, allowing sustained therapeutic effects.
Clinical Uses
- Malaria treatment and prophylaxis
- Systemic lupus erythematosus (SLE)
- Rheumatoid arthritis
- Discoid lupus erythematosus
- Certain dermatologic autoimmune disorders
Hydroxychloroquine is commonly used as a disease-modifying antirheumatic drug (DMARD).
Adverse Effects
Common adverse effects:
- Nausea
- Abdominal discomfort
- Headache
Serious adverse effects:
- Retinal toxicity (retinopathy)
- Visual disturbances
- Myopathy
Important monitoring:
Long-term therapy requires regular ophthalmologic examinations to prevent retinal damage.
Comparative Analysis
| Feature | Hydroxychloroquine | Chloroquine | Methotrexate |
|---|---|---|---|
| Drug class | Antimalarial / Immunomodulator | Antimalarial | Immunosuppressant |
| Mechanism | Lysosomal pH increase and TLR inhibition | Heme detoxification inhibition | Dihydrofolate reductase inhibition |
| Main clinical use | SLE and rheumatoid arthritis | Malaria | Rheumatoid arthritis and cancer |
| Immune modulation | Yes | Minimal | Strong |
| Major toxicity | Retinopathy | Retinopathy | Hepatotoxicity |
Explanation:
Hydroxychloroquine and chloroquine share similar antimalarial mechanisms, interfering with heme detoxification in parasites. However, hydroxychloroquine has better safety and stronger immunomodulatory effects, making it useful in autoimmune diseases. Methotrexate acts through a completely different mechanism by inhibiting folate metabolism and suppressing immune cell proliferation.
MCQs
- Hydroxychloroquine primarily accumulates in:
a) Mitochondria
b) Lysosomes
c) Ribosomes
d) Nucleus
Answer: b) Lysosomes
- Hydroxychloroquine increases the pH of:
a) Cytoplasm
b) Lysosomes
c) Nucleus
d) Golgi apparatus
Answer: b) Lysosomes
- In autoimmune diseases, hydroxychloroquine inhibits:
a) Toll-like receptors
b) Dopamine receptors
c) Beta receptors
d) NMDA receptors
Answer: a) Toll-like receptors
- Hydroxychloroquine interferes with malaria parasite by:
a) Inhibiting DNA replication
b) Blocking heme detoxification
c) Blocking ribosomes
d) Inhibiting glycolysis
Answer: b) Blocking heme detoxification
- Hydroxychloroquine is commonly used to treat:
a) Asthma
b) Systemic lupus erythematosus
c) Tuberculosis
d) Hypertension
Answer: b) Systemic lupus erythematosus
- Long-term toxicity of hydroxychloroquine mainly affects:
a) Kidney
b) Retina
c) Liver
d) Lung
Answer: b) Retina
- Hydroxychloroquine belongs to which drug class?
a) Antimalarial
b) Antibiotic
c) Antiviral
d) Anticoagulant
Answer: a) Antimalarial
- Hydroxychloroquine suppresses inflammatory cytokines by:
a) Increasing lysosomal acidity
b) Raising lysosomal pH
c) Increasing DNA synthesis
d) Activating complement
Answer: b) Raising lysosomal pH
- Regular monitoring during therapy should include:
a) ECG
b) Ophthalmologic examination
c) Thyroid tests
d) Lung function tests
Answer: b) Ophthalmologic examination
- Hydroxychloroquine is classified as a:
a) Disease modifying antirheumatic drug
b) Beta blocker
c) Anticoagulant
d) Antihistamine
Answer: a) Disease modifying antirheumatic drug
FAQs
- How does hydroxychloroquine help in autoimmune diseases?
By suppressing immune activation and reducing inflammatory cytokine production. - Why does hydroxychloroquine accumulate in lysosomes?
Because it is a weak base that becomes trapped in acidic organelles. - What is the most important toxicity of hydroxychloroquine?
Retinal toxicity leading to vision problems. - Why are eye examinations required during treatment?
To detect early retinal damage caused by long-term drug accumulation. - How does hydroxychloroquine kill malaria parasites?
By interfering with heme detoxification in the parasite’s food vacuole. - Is hydroxychloroquine an immunosuppressant?
It is considered an immunomodulatory drug rather than a strong immunosuppressant.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookID=2189
Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookID=2249
Tripathi KD. Essentials of Medical Pharmacology
https://jaypeedigital.com/book/9789354651970
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookID=3095


