Table of Contents
Introduction
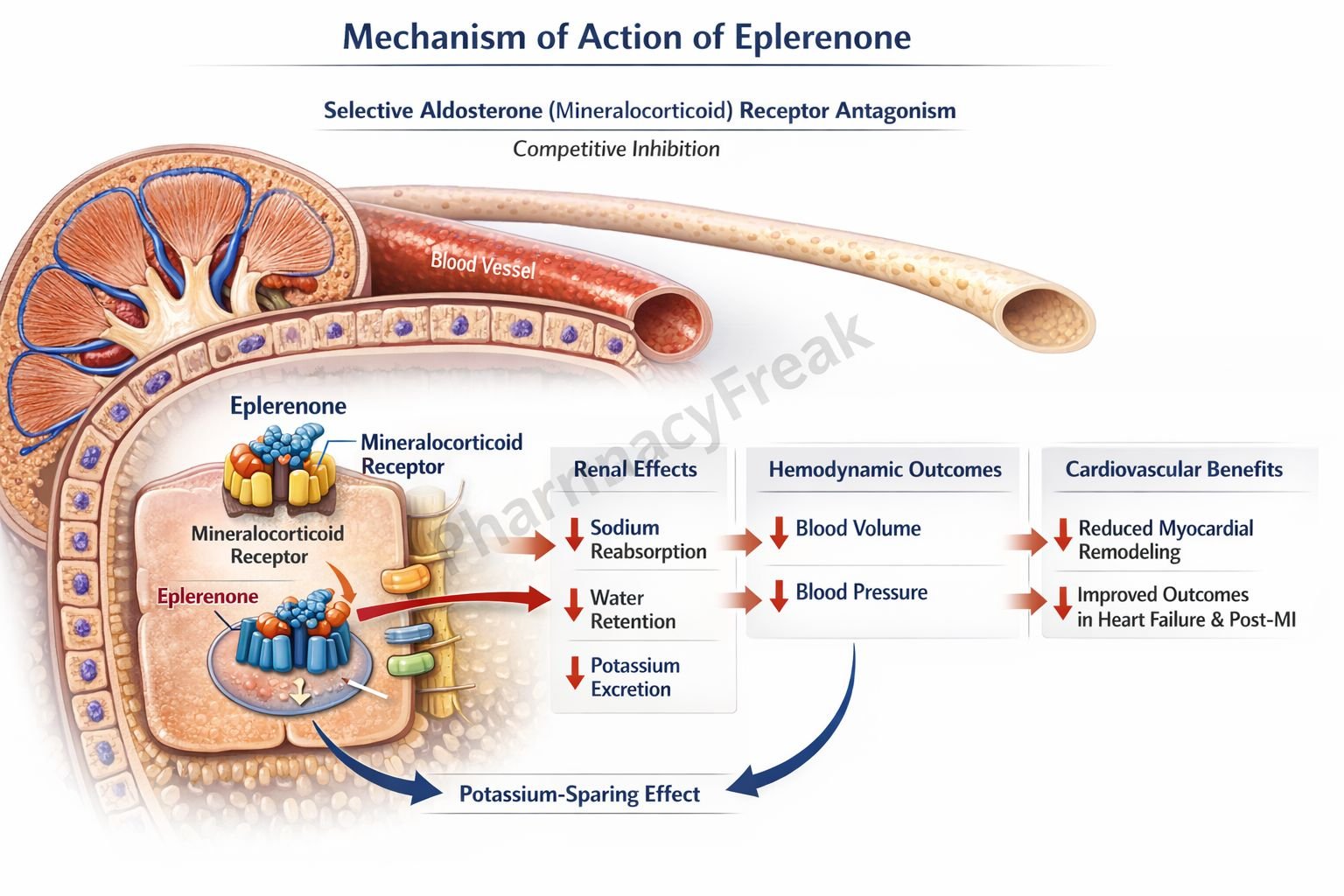
Eplerenone is a selective mineralocorticoid receptor antagonist (MRA) used primarily in cardiovascular disorders such as heart failure and hypertension. It is a steroidal compound structurally related to spironolactone but with greater receptor selectivity, resulting in fewer endocrine adverse effects. From an exam and clinical standpoint, eplerenone is important due to its role in blocking aldosterone-mediated cardiovascular remodeling while maintaining a better safety profile.

Mechanism of Action (Step-wise)
Eplerenone acts by selectively antagonizing aldosterone at mineralocorticoid receptors.
Step 1: Aldosterone receptor targeting
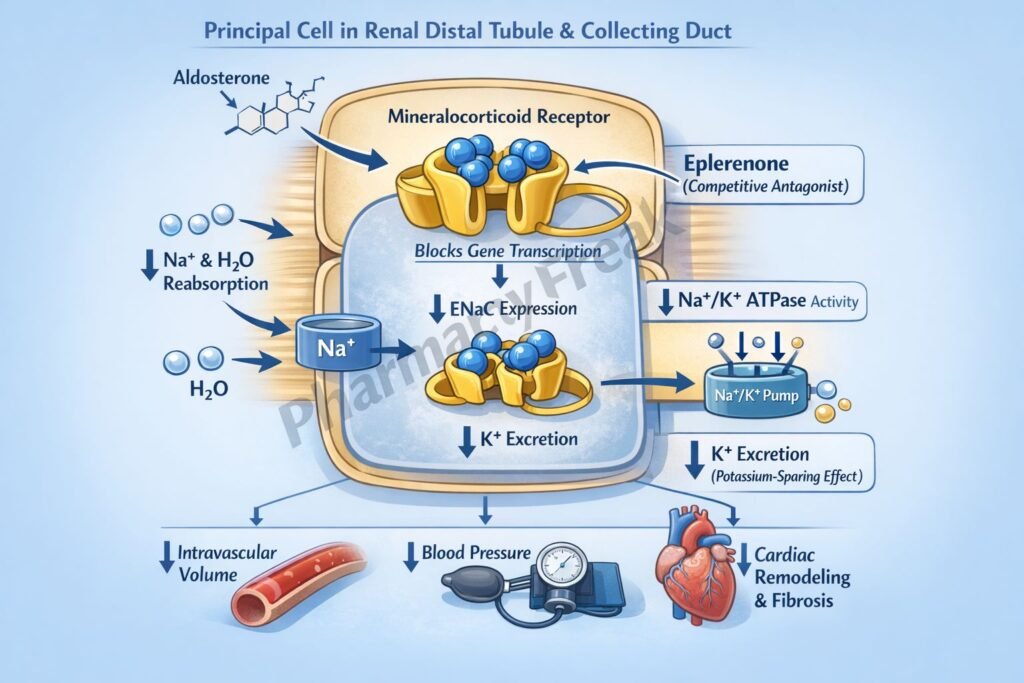
Eplerenone selectively binds to mineralocorticoid receptors (MR) located in the distal convoluted tubule and collecting duct of the nephron, as well as in cardiac and vascular tissues.
Step 2: Competitive antagonism of aldosterone
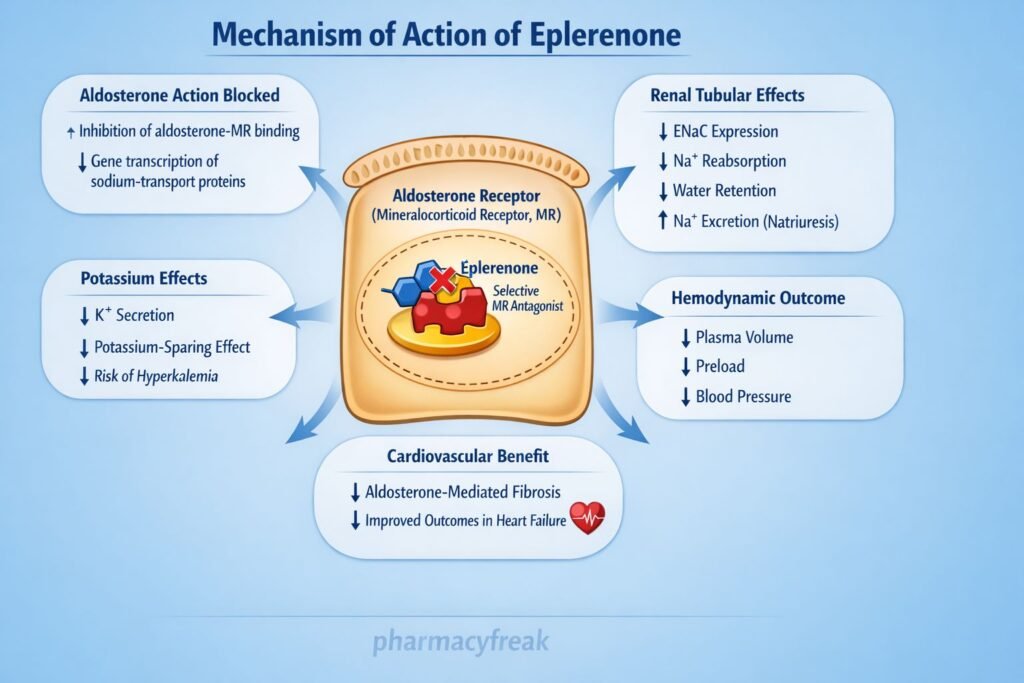
By competitively inhibiting aldosterone binding, eplerenone prevents receptor activation and subsequent gene transcription.
Step 3: Inhibition of sodium reabsorption
Blockade of MR reduces transcription of epithelial sodium channels (ENaC) and Na⁺/K⁺-ATPase pumps, leading to decreased sodium and water reabsorption.
Step 4: Potassium-sparing effect
Reduced sodium reabsorption decreases potassium secretion in the collecting tubules, resulting in potassium retention.
Step 5: Cardiovascular protective effects
In cardiac tissue, MR blockade reduces aldosterone-induced myocardial fibrosis, inflammation, and ventricular remodeling, improving outcomes in heart failure and post–myocardial infarction patients.
Pharmacokinetics
- Route of administration: Oral
- Bioavailability: Approximately 70%
- Protein binding: ~50%
- Metabolism: Extensively metabolized in the liver by CYP3A4
- Half-life: 4–6 hours
- Excretion: Via urine and feces as inactive metabolites
- Onset: Gradual antihypertensive and cardioprotective effects
Clinical Uses
- Heart failure with reduced ejection fraction (HFrEF)
- Post–myocardial infarction left ventricular dysfunction
- Hypertension (especially resistant hypertension)
- Aldosterone-mediated cardiovascular remodeling prevention
Eplerenone is often preferred over spironolactone when antiandrogenic adverse effects must be avoided.
Adverse Effects
Electrolyte disturbances:
- Hyperkalemia (dose-limiting and clinically significant)
Cardiovascular:
- Hypotension (rare)
Endocrine (minimal):
- Gynecomastia (very rare)
- Sexual dysfunction (much less than spironolactone)
Drug interaction–related:
- Increased risk of toxicity with strong CYP3A4 inhibitors
Comparative Analysis
Eplerenone vs Spironolactone
| Feature | Eplerenone | Spironolactone |
|---|---|---|
| Receptor selectivity | High (MR selective) | Low (MR + androgen) |
| Antiandrogen effects | Minimal | Common |
| Gynecomastia | Rare | Frequent |
| CYP metabolism | CYP3A4 | Minimal |
| Use in HF | Preferred | Effective but less selective |
Explanation:
Eplerenone’s higher selectivity for mineralocorticoid receptors explains its reduced endocrine adverse effects compared to spironolactone. However, CYP3A4 metabolism increases the potential for drug–drug interactions, which is clinically relevant in polypharmacy patients.
MCQs
- Eplerenone primarily antagonizes which receptor?
a) Androgen receptor
b) Glucocorticoid receptor
c) Mineralocorticoid receptor
d) Estrogen receptor
Answer: c) Mineralocorticoid receptor
- The potassium-sparing effect of eplerenone is due to inhibition of:
a) Loop of Henle sodium transport
b) ENaC expression
c) Carbonic anhydrase
d) Aldosterone synthesis
Answer: b) ENaC expression
- Major metabolic pathway of eplerenone involves:
a) CYP2D6
b) MAO
c) CYP3A4
d) COMT
Answer: c) CYP3A4
- Compared to spironolactone, eplerenone causes less gynecomastia because it:
a) Is non-steroidal
b) Has higher MR selectivity
c) Has shorter half-life
d) Is renally excreted
Answer: b) Has higher MR selectivity
- Most important adverse effect of eplerenone is:
a) Hypokalemia
b) Hyperkalemia
c) Bradycardia
d) Metabolic acidosis
Answer: b) Hyperkalemia
- Eplerenone is especially useful after myocardial infarction due to:
a) Vasodilator effect
b) Antiarrhythmic action
c) Reduction of ventricular remodeling
d) Increased cardiac contractility
Answer: c) Reduction of ventricular remodeling
- Which drug interaction increases eplerenone toxicity?
a) Rifampicin
b) Ketoconazole
c) Furosemide
d) Digoxin
Answer: b) Ketoconazole
- Eplerenone reduces aldosterone-induced fibrosis mainly in:
a) Liver
b) Kidney cortex
c) Cardiac tissue
d) Skeletal muscle
Answer: c) Cardiac tissue
- Eplerenone differs from potassium supplements because it:
a) Directly provides potassium
b) Prevents potassium excretion
c) Stimulates aldosterone
d) Inhibits Na⁺/K⁺-ATPase
Answer: b) Prevents potassium excretion
- Preferred MRA in patients with endocrine side effects is:
a) Amiloride
b) Triamterene
c) Spironolactone
d) Eplerenone
Answer: d) Eplerenone
FAQs
1. Why is eplerenone more selective than spironolactone?
It has minimal affinity for androgen and progesterone receptors.
2. Does eplerenone cause gynecomastia?
Rarely, due to high mineralocorticoid receptor selectivity.
3. Why is hyperkalemia a concern with eplerenone?
Because it reduces potassium excretion in the collecting duct.
4. Can eplerenone be used in renal impairment?
Use with caution; hyperkalemia risk increases with reduced renal function.
5. Why are CYP3A4 inhibitors contraindicated?
They raise plasma levels of eplerenone, increasing toxicity risk.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accesspharmacy.mhmedical.com - Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com - Tripathi KD. Essentials of Medical Pharmacology
- Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com


