Table of Contents
Introduction
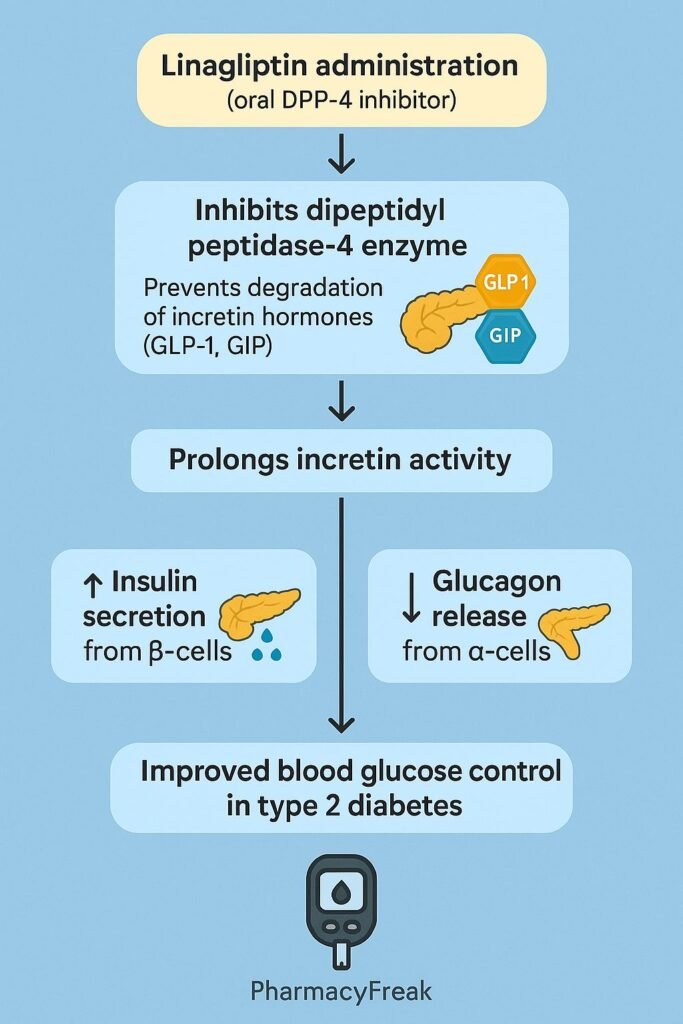
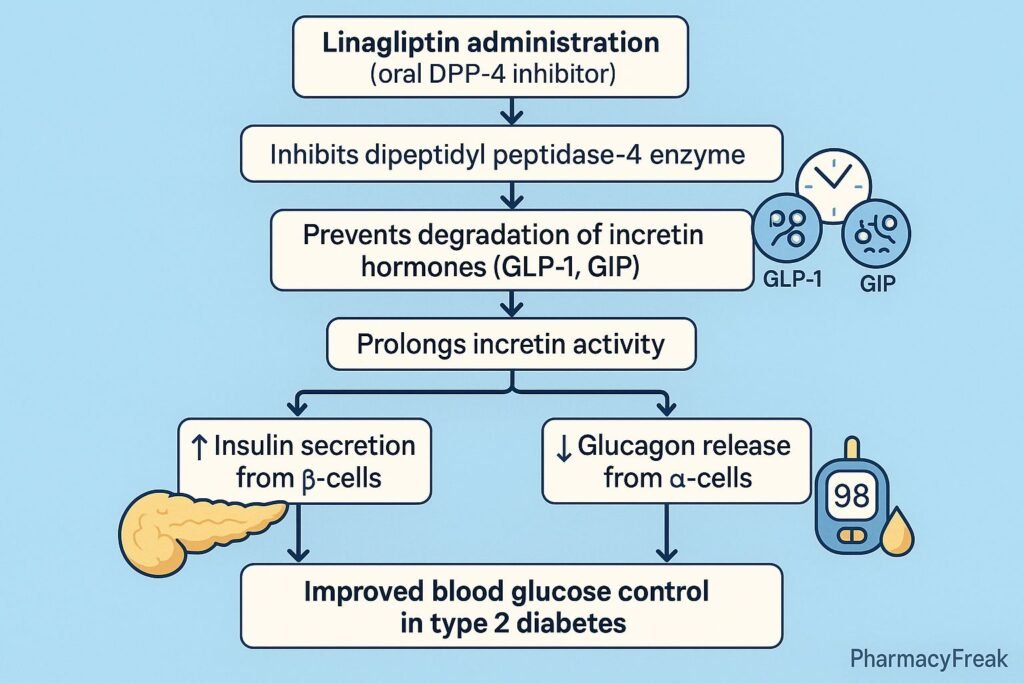
Linagliptin is an oral hypoglycemic drug belonging to the class of dipeptidyl peptidase-4 (DPP-4) inhibitors. It is primarily used in the management of type 2 diabetes mellitus to improve glycemic control. Unlike many other antidiabetic agents, linagliptin has a unique excretion pathway, being mostly eliminated via the enterohepatic system rather than the kidneys, making it safer for patients with renal impairment. Understanding the mechanism of action of linagliptin is essential for clinical decision-making and safe pharmacotherapy.
Mechanism of Action (Step-wise)
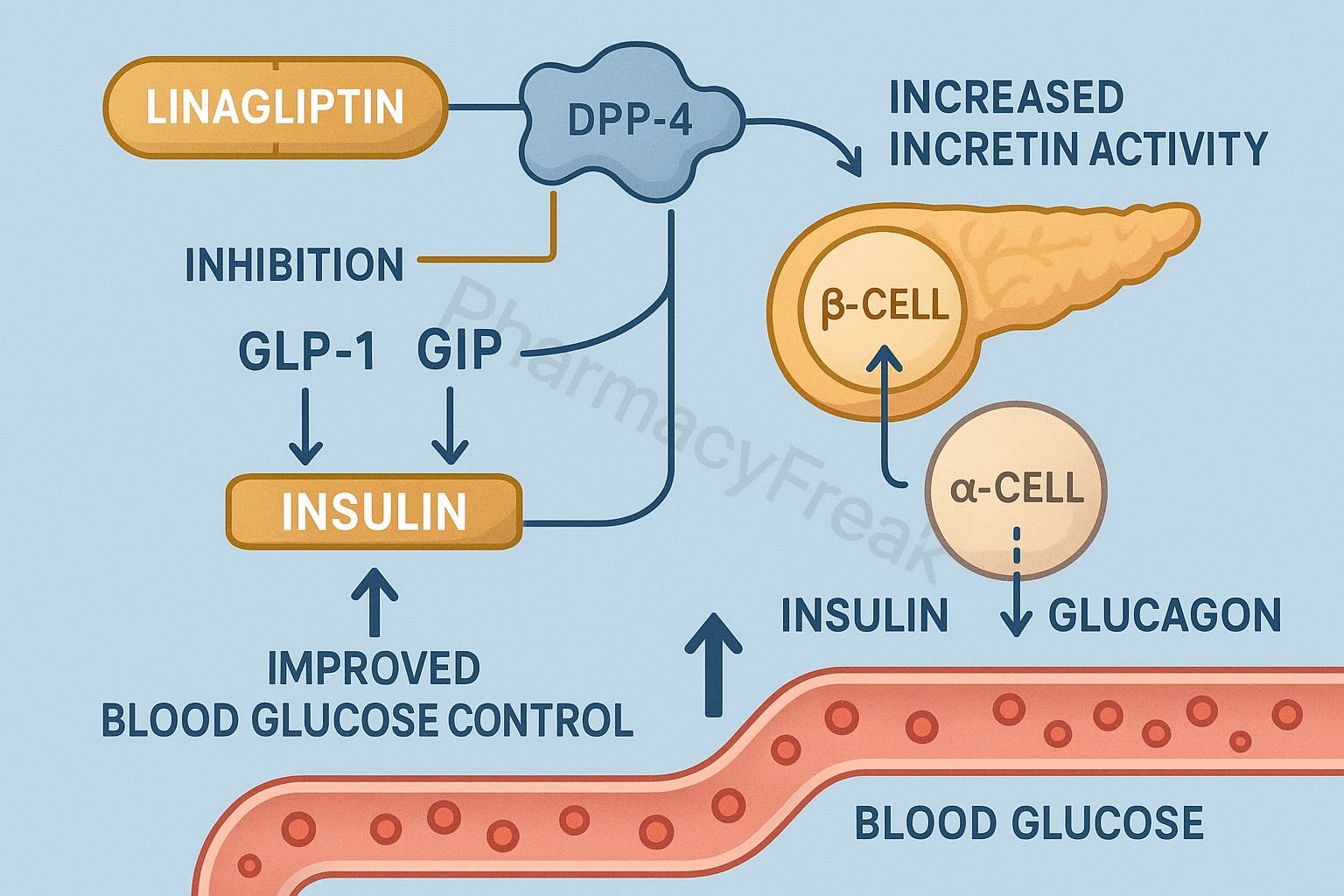
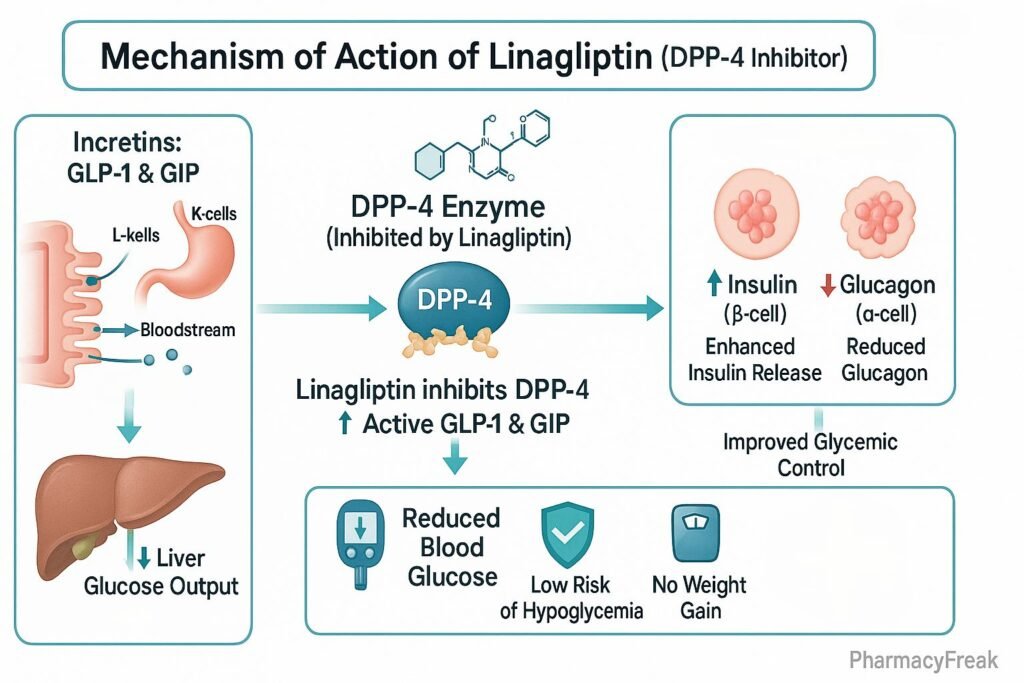
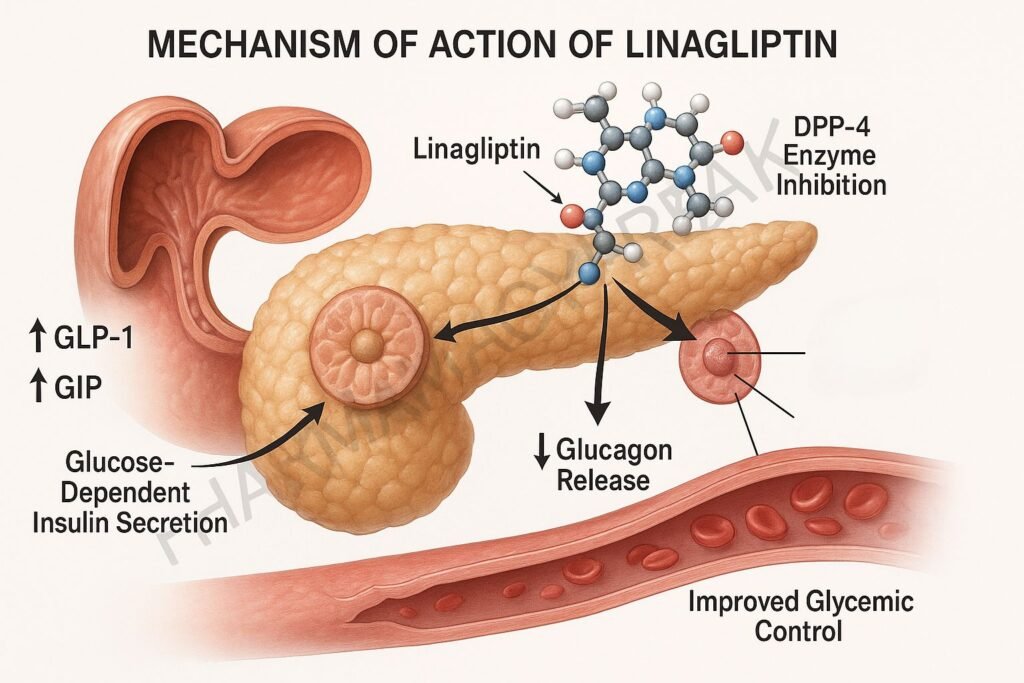
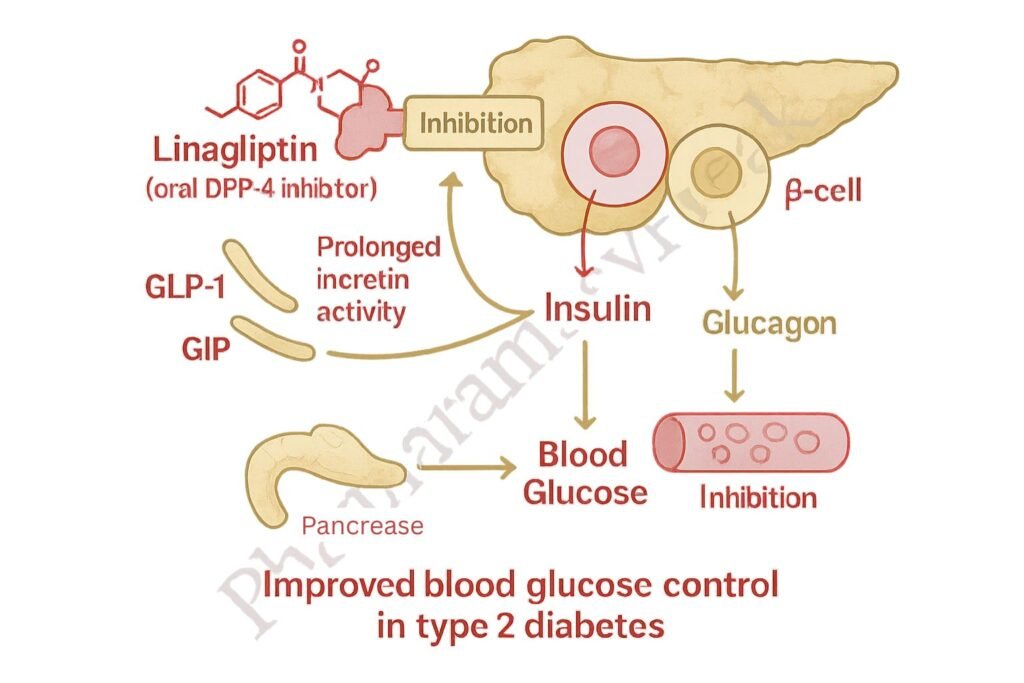
- Inhibition of DPP-4 Enzyme
- Linagliptin selectively inhibits the dipeptidyl peptidase-4 (DPP-4) enzyme.
- DPP-4 normally degrades incretin hormones such as glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP).
- Prolongation of Incretin Activity
- By inhibiting DPP-4, linagliptin increases the half-life of GLP-1 and GIP.
- These incretin hormones remain active longer in the bloodstream.
- Enhanced Insulin Secretion
- Active GLP-1 and GIP stimulate glucose-dependent insulin release from pancreatic β-cells.
- This effect lowers postprandial glucose levels.
- Suppression of Glucagon Secretion
- GLP-1 reduces glucagon secretion from pancreatic α-cells.
- Reduced glucagon lowers hepatic glucose production.
- Overall Effect
- Increased insulin release + decreased glucagon = improved glycemic control.
- Because the mechanism is glucose-dependent, linagliptin has a low risk of hypoglycemia compared to sulfonylureas.
Pharmacokinetics
- Absorption: Rapidly absorbed after oral administration with high bioavailability.
- Distribution: Widely distributed; moderate protein binding.
- Metabolism: Minimal hepatic metabolism; largely unchanged drug circulates.
- Excretion: Predominantly via bile and gut (enterohepatic system); minimal renal excretion.
- Half-life: ~12 hours, allowing once-daily dosing.
Clinical Uses
- Type 2 diabetes mellitus (monotherapy or combination therapy).
- Preferred in patients with renal impairment (no dose adjustment needed).
- Often combined with metformin, sulfonylureas, or insulin when monotherapy is insufficient.
Adverse Effects
- Common: Nasopharyngitis, headache, cough, joint pain.
- Less common: Hypoglycemia (mostly with sulfonylureas or insulin).
- Rare but serious: Pancreatitis, hypersensitivity reactions, bullous pemphigoid.
Comparative Analysis
| Feature | Linagliptin (DPP-4 inhibitor) | Metformin (Biguanide) | Sulfonylureas |
|---|---|---|---|
| Mechanism | Inhibits DPP-4, ↑ incretins | ↓ hepatic glucose output | Stimulates insulin release |
| Hypoglycemia risk | Low | Low | High |
| Effect on weight | Neutral | Neutral/↓ | Weight gain |
| Excretion pathway | Enterohepatic | Renal | Renal/hepatic |
| Use in renal impairment | Safe (no dose adjustment) | Contraindicated (eGFR <30) | Use with caution |
MCQs
1. What is the primary mechanism of action of linagliptin?
a) Inhibition of α-glucosidase
b) Stimulation of insulin release directly
c) Inhibition of DPP-4 enzyme
d) Inhibition of SGLT2 transporter
Answer: c) Inhibition of DPP-4 enzyme
2. Which incretin hormone is preserved by linagliptin?
a) Amylin
b) Ghrelin
c) GLP-1 and GIP
d) Leptin
Answer: c) GLP-1 and GIP
3. Why is linagliptin safe in patients with renal impairment?
a) It is hepatically metabolized
b) It is excreted via enterohepatic system
c) It is dialyzable
d) It reduces kidney glucose reabsorption
Answer: b) It is excreted via enterohepatic system
4. Which adverse effect is most commonly associated with linagliptin?
a) Hypoglycemia
b) Nasopharyngitis
c) Lactic acidosis
d) Weight gain
Answer: b) Nasopharyngitis
5. The risk of hypoglycemia with linagliptin increases when combined with:
a) Metformin
b) Pioglitazone
c) Sulfonylureas
d) GLP-1 agonists
Answer: c) Sulfonylureas
6. Linagliptin primarily works in a:
a) Glucose-dependent manner
b) Glucose-independent manner
c) Insulin-independent manner
d) Ketone-dependent manner
Answer: a) Glucose-dependent manner
7. Which condition is a rare but serious side effect of linagliptin?
a) Hypertension
b) Pancreatitis
c) Renal failure
d) Hepatotoxicity
Answer: b) Pancreatitis
8. Half-life of linagliptin is approximately:
a) 2 hours
b) 6 hours
c) 12 hours
d) 24 hours
Answer: c) 12 hours
9. Which class of drugs does linagliptin belong to?
a) Biguanides
b) Sulfonylureas
c) DPP-4 inhibitors
d) Thiazolidinediones
Answer: c) DPP-4 inhibitors
10. Linagliptin helps in diabetes management by:
a) Directly lowering blood glucose
b) Enhancing incretin action
c) Blocking glucose absorption in intestine
d) Increasing renal glucose excretion
Answer: b) Enhancing incretin action
FAQs
Q1. Is linagliptin used in type 1 diabetes?
No, it is approved only for type 2 diabetes mellitus.
Q2. Does linagliptin cause weight gain?
No, it is considered weight-neutral.
Q3. Can linagliptin be combined with metformin?
Yes, it is often used in combination therapy with metformin for better glycemic control.
Q4. Does linagliptin require dose adjustment in renal impairment?
No, unlike other DPP-4 inhibitors, linagliptin does not require dose modification.
Q5. What is the main advantage of linagliptin over other DPP-4 inhibitors?
Its non-renal excretion pathway makes it safer in patients with kidney dysfunction.
Q6. Can linagliptin cause hypoglycemia when used alone?
No, due to its glucose-dependent mechanism, the risk of hypoglycemia is very low in monotherapy.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
- Katzung Basic and Clinical Pharmacology
- Clinical trials data on linagliptin efficacy and safety


