Table of Contents
Introduction
Hydrochlorothiazide (HCTZ) is a thiazide diuretic widely used in the treatment of hypertension, edema, and certain kidney disorders. It acts primarily on the distal convoluted tubule of the nephron to promote sodium and water excretion. By reducing extracellular fluid volume and decreasing peripheral vascular resistance, hydrochlorothiazide effectively lowers blood pressure.
Thiazide diuretics are among the most commonly prescribed antihypertensive medications and are recommended as first-line therapy for uncomplicated hypertension in many clinical guidelines.
Understanding the mechanism of hydrochlorothiazide is important for pharmacology and medical licensing examinations such as USMLE, NEET PG, FMGE, PLAB, INICET, NCLEX, and MCCQE.
Mechanism of Action (Step-wise)
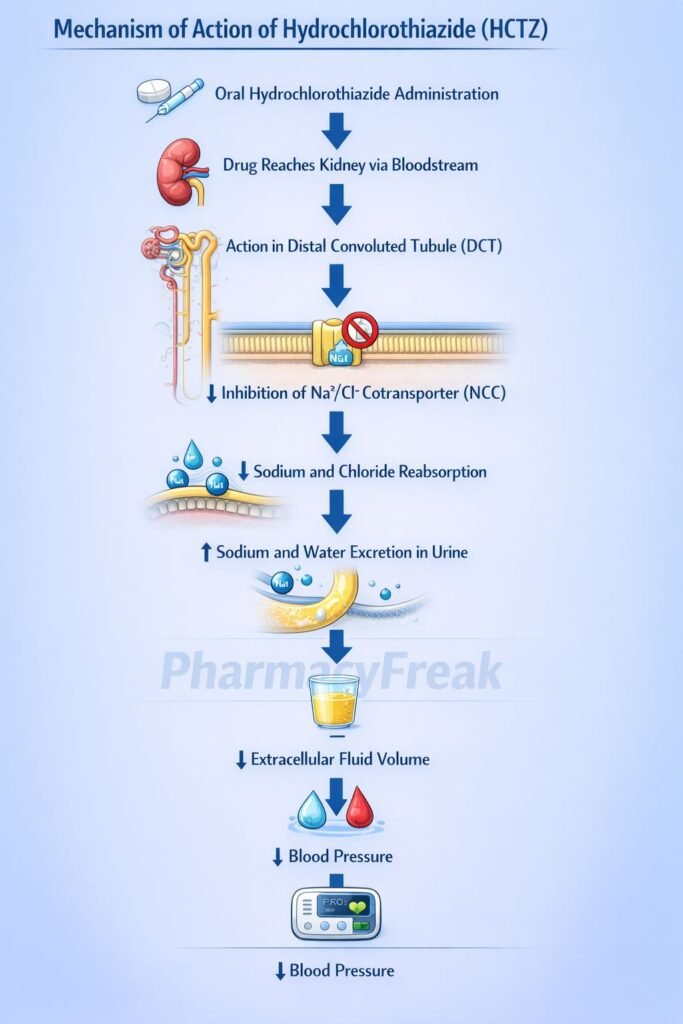
Hydrochlorothiazide acts by inhibiting sodium reabsorption in the distal convoluted tubule of the kidney.
Step 1: Action at distal convoluted tubule
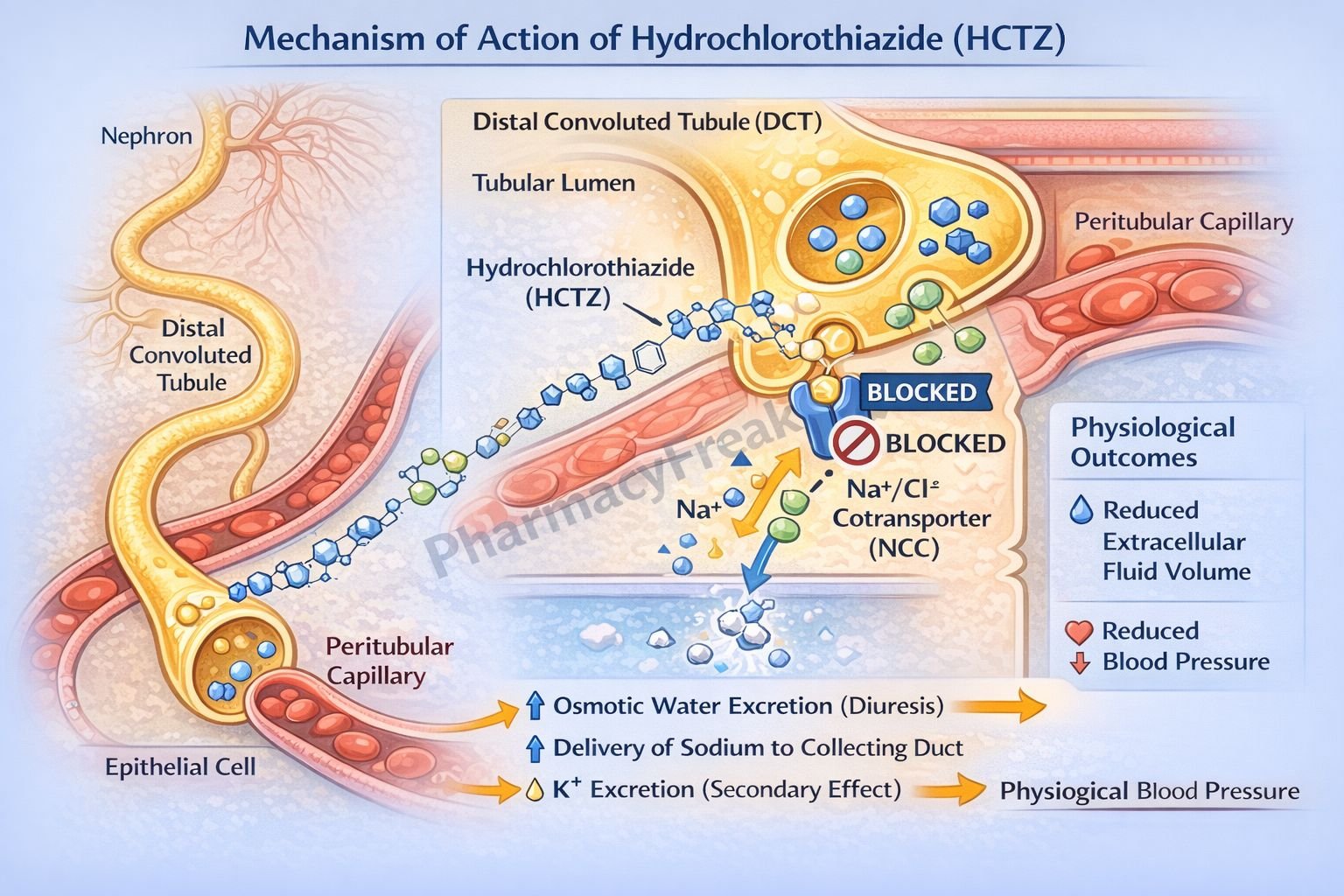
Hydrochlorothiazide reaches the distal convoluted tubule of the nephron via the bloodstream and tubular secretion.
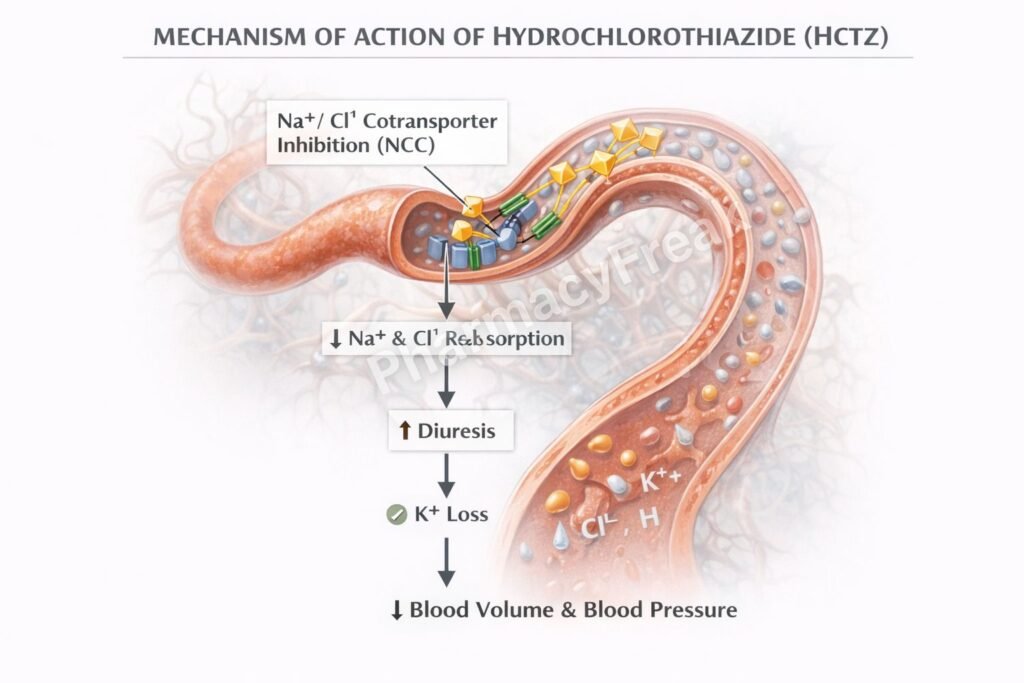
Step 2: Inhibition of Na⁺/Cl⁻ cotransporter
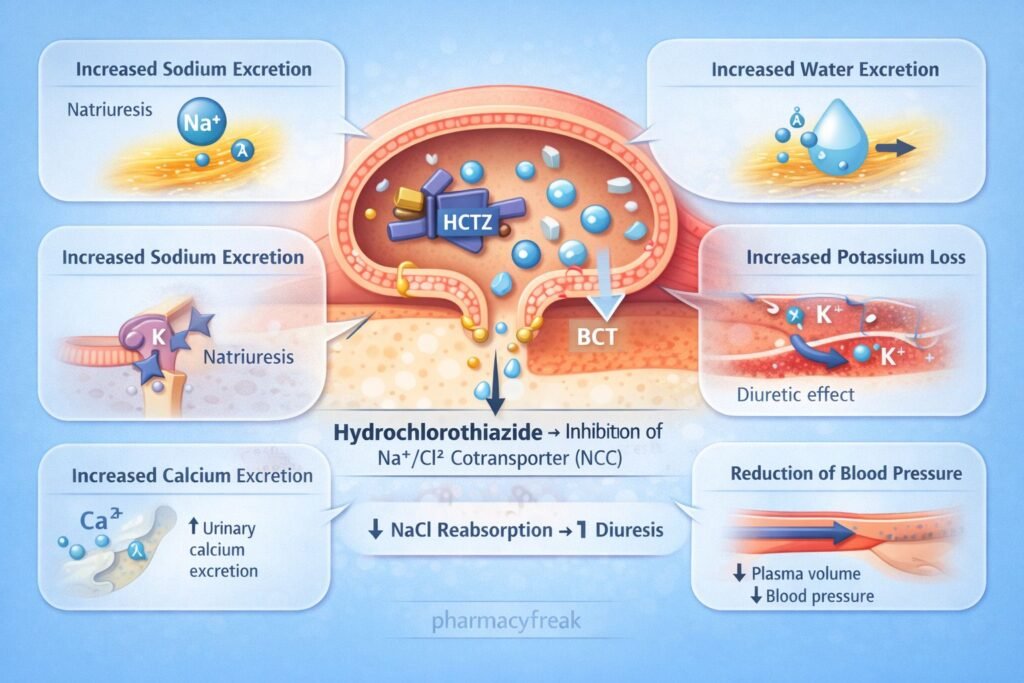
HCTZ inhibits the sodium chloride cotransporter (NCC) located on the luminal membrane of distal tubular cells.
Step 3: Decreased sodium reabsorption
Blocking this transporter prevents reabsorption of sodium and chloride ions.
Step 4: Increased sodium and water excretion
Sodium remains in the tubular fluid, increasing osmotic water excretion.
Step 5: Reduction in plasma volume
Loss of sodium and water decreases extracellular fluid volume and venous return.
Step 6: Long term reduction in peripheral resistance
Chronic therapy leads to reduced peripheral vascular resistance, contributing to sustained blood pressure reduction.
Overall effect:
Increased urinary excretion of sodium, chloride, and water leading to reduced blood volume and decreased blood pressure.
Important pharmacology concept:
Thiazide diuretics increase calcium reabsorption in the distal tubule, which differentiates them from loop diuretics.
Pharmacokinetics
Absorption:
Well absorbed after oral administration.
Distribution:
Distributed widely in body fluids and renal tissues.
Metabolism:
Minimal hepatic metabolism.
Excretion:
Primarily excreted unchanged in urine via renal excretion.
Duration:
Diuretic effect typically lasts 12 to 24 hours.
Clinical Uses
- Hypertension (first line therapy)
- Edema associated with heart failure
- Edema due to liver cirrhosis or renal disease
- Prevention of recurrent calcium kidney stones
- Nephrogenic diabetes insipidus
Hydrochlorothiazide is frequently combined with other antihypertensive drugs such as ACE inhibitors or ARBs.
Adverse Effects
Common adverse effects:
- Hypokalemia
- Hyponatremia
- Hyperuricemia
- Hyperglycemia
Other adverse effects:
- Hyperlipidemia
- Photosensitivity
- Dehydration
Important clinical concept:
Thiazide diuretics can increase serum calcium levels due to enhanced calcium reabsorption.
Comparative Analysis
| Feature | Hydrochlorothiazide | Furosemide | Spironolactone |
|---|---|---|---|
| Drug class | Thiazide diuretic | Loop diuretic | Potassium-sparing diuretic |
| Site of action | Distal convoluted tubule | Thick ascending limb | Collecting duct |
| Target transporter | Na⁺/Cl⁻ cotransporter | Na⁺/K⁺/2Cl⁻ transporter | Aldosterone receptor |
| Effect on potassium | Decreases potassium | Decreases potassium | Increases potassium |
| Effect on calcium | Increases calcium reabsorption | Decreases calcium reabsorption | Minimal effect |
Explanation:
Hydrochlorothiazide inhibits the Na⁺/Cl⁻ cotransporter in the distal convoluted tubule, increasing sodium and water excretion while enhancing calcium reabsorption. Furosemide, a loop diuretic, acts earlier in the nephron and produces stronger diuresis but increases calcium excretion. Spironolactone works in the collecting duct by blocking aldosterone receptors and conserving potassium.
MCQs
- Hydrochlorothiazide belongs to which drug class?
a) Loop diuretic
b) Thiazide diuretic
c) Potassium-sparing diuretic
d) Osmotic diuretic
Answer: b) Thiazide diuretic
- HCTZ acts primarily in the:
a) Proximal tubule
b) Loop of Henle
c) Distal convoluted tubule
d) Collecting duct
Answer: c) Distal convoluted tubule
- HCTZ inhibits which transporter?
a) Na⁺/K⁺/2Cl⁻ transporter
b) Na⁺/Cl⁻ cotransporter
c) H⁺ ATPase
d) SGLT2 transporter
Answer: b) Na⁺/Cl⁻ cotransporter
- Thiazide diuretics cause increased excretion of:
a) Sodium and water
b) Glucose
c) Calcium
d) Bicarbonate
Answer: a) Sodium and water
- A common electrolyte abnormality caused by HCTZ is:
a) Hyperkalemia
b) Hypokalemia
c) Hypernatremia
d) Hypermagnesemia
Answer: b) Hypokalemia
- Thiazide diuretics increase reabsorption of:
a) Sodium
b) Calcium
c) Potassium
d) Chloride
Answer: b) Calcium
- Hydrochlorothiazide is commonly used to treat:
a) Hypertension
b) Asthma
c) Diabetes mellitus
d) Tuberculosis
Answer: a) Hypertension
- Compared with loop diuretics, thiazides:
a) Cause stronger diuresis
b) Act in the distal tubule
c) Decrease calcium reabsorption
d) Increase potassium levels
Answer: b) Act in the distal tubule
- Long term antihypertensive effect occurs due to:
a) Increased heart rate
b) Reduced peripheral resistance
c) Increased cardiac output
d) Increased sodium retention
Answer: b) Reduced peripheral resistance
- HCTZ is mainly eliminated through:
a) Liver
b) Kidney
c) Lung
d) Intestine
Answer: b) Kidney
FAQs
- How does hydrochlorothiazide lower blood pressure?
By increasing sodium and water excretion, reducing plasma volume and peripheral vascular resistance. - Where does hydrochlorothiazide act in the nephron?
In the distal convoluted tubule. - Why do thiazide diuretics cause hypokalemia?
Increased sodium delivery to the collecting duct promotes potassium secretion. - Why are thiazides used in kidney stones?
They increase calcium reabsorption, reducing urinary calcium excretion. - What electrolyte imbalance is common with thiazides?
Hypokalemia and hyponatremia. - How do thiazides differ from loop diuretics?
Thiazides act in the distal tubule and increase calcium reabsorption, whereas loop diuretics act in the loop of Henle and increase calcium excretion.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookID=2189
Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookID=2249
Tripathi KD. Essentials of Medical Pharmacology
https://jaypeedigital.com/book/9789354651970
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookID=3095


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com