
Table of Contents
Introduction
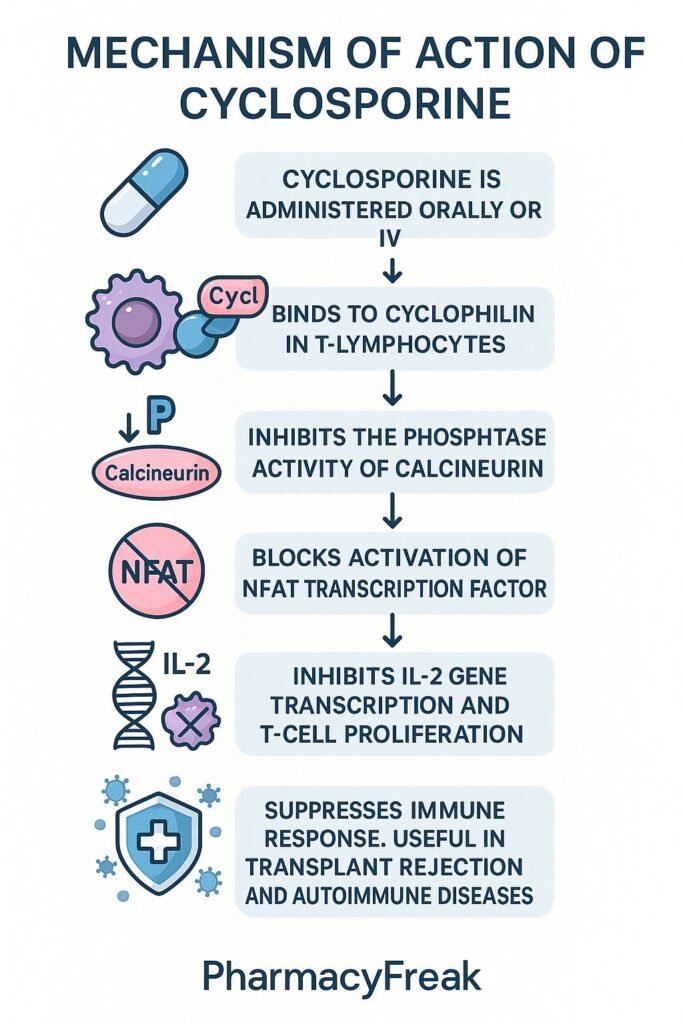
Cyclosporine is a calcineurin inhibitor used primarily to prevent organ transplant rejection and to treat select autoimmune disorders. It binds to cyclophilin, forming a complex that inhibits calcineurin, thereby blocking T‑cell activation and interleukin‑2 (IL‑2) production. This selective immunosuppression reduces T‑lymphocyte–mediated damage.
Step-by-Step Mechanism of Action
- Cyclophilin Binding
Cyclosporine binds intracellular cyclophilin in T‑lymphocytes. - Calcineurin Inhibition
The cyclosporine–cyclophilin complex inhibits calcineurin, a calcium/calmodulin‑dependent phosphatase. - NFAT Dephosphorylation Blockade
Calcineurin inhibition prevents dephosphorylation and nuclear translocation of NFAT (nuclear factor of activated T cells). - Suppression of IL‑2 and Cytokine Gene Transcription
Without active NFAT in the nucleus, IL‑2 and other cytokine genes are not transcribed. - Reduced T‑Cell Proliferation and Activation
Lower IL‑2 levels lead to diminished T‑cell growth, differentiation, and immune response.
Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Bioavailability | ~30% (range 10–90%) |
| Time to Peak (Tₘₐₓ) | ~1–2 hours after oral dose |
| Half-Life | ~6–27 hours (variable) |
| Protein Binding | ~90% bound (plasma proteins) |
| Metabolism | Hepatic via CYP3A4 and P‑gp |
| Excretion | Primarily biliary (fecal), <6% renal |
Clinical Uses
- Prevention of organ transplant rejection (renal, hepatic, cardiac)
- Treatment of graft-versus-host disease
- Management of autoimmune conditions: psoriasis, rheumatoid arthritis, severe nephrotic syndrome, uveitis
Adverse Effects
- Nephrotoxicity (dose-dependent)
- Hypertension
- Hirsutism, gum hypertrophy
- Tremor, headache
- Hyperlipidemia, hyperkalemia
- Increased susceptibility to infections and malignancies
- Rare: neurotoxicity, hepatotoxicity
Comparative Analysis
| Feature | Cyclosporine | Tacrolimus |
|---|---|---|
| Binding Protein | Cyclophilin | FK506‑binding protein (FKBP‑12) |
| Mechanism | Calcineurin inhibition | Calcineurin inhibition |
| Potency | Less potent | More potent |
| Side Effect Profile | Nephrotoxicity, hirsutism, gum growth | Nephrotoxicity, hyperglycemia, neurotoxicity |
| Therapeutic Window | Narrow | Narrow |
| Monitoring Required | Yes (trough levels) | Yes (trough levels) |
MCQs
1. Cyclosporine blocks T-cell activation by:
A. Binding FKBP-12
B. Enhancing IL‑2 production
C. Inhibiting calcineurin via cyclophilin binding
D. Blocking IL‑1 receptors
Answer: C
2. The transcription factor affected is:
A. NF‑κB
B. AP‑1
C. NFAT
D. STAT‑3
Answer: C
3. Major toxicity concern is:
A. Hepatotoxicity
B. Nephrotoxicity
C. Severe infections
D. Thrombocytopenia
Answer: B
4. Cyclosporine is metabolized by:
A. CYP2D6
B. CYP1A2
C. CYP3A4
D. CYP2E1
Answer: C
5. A drug effect not commonly seen with cyclosporine is:
A. Hypertension
B. Hirsutism
C. Hyperglycemia
D. Gum hypertrophy
Answer: C
6. Which drug binds to FKBP instead of cyclophilin?
A. Sirolimus
B. Mycophenolate
C. Tacrolimus
D. Leflunomide
Answer: C
7. Cyclosporine must be monitored due to:
A. Wide therapeutic index
B. Narrow therapeutic window
C. No metabolism
D. No interactions
Answer: B
8. Its effect on IL‑2 is to:
A. Increase production
B. Block receptor
C. Suppress production
D. Degrade mRNA
Answer: C
9. Compared to tacrolimus, cyclosporine is:
A. More potent
B. Less potent
C. Same potency
D. Not immunosuppressive
Answer: B
10. Primary excretion route is:
A. Renal unchanged
B. Biliary fecal
C. Biliary fecal
D. Pulmonary
Answer: C
FAQs
1. Is cyclosporine monitored via blood levels?
Yes—trough levels are routinely checked to maintain therapeutic dosing and avoid toxicity.
2. Why does it cause high blood pressure?
Due to vasoconstriction effects and altered renal sodium handling.
3. How is nephrotoxicity managed?
Through dose adjustment, hydration, and monitoring kidney function.
4. Can cyclosporine be substituted with tacrolimus?
Yes—tacrolimus is often used for its higher potency and different side effect profile.
5. Does cyclosporine increase cancer risk?
Yes—long-term use may elevate risk of lymphomas and skin cancers.
References
- DrugBank – Cyclosporine Profile
- NCBI Bookshelf – Cyclosporine in Transplant Medicine
- FDA Label – Neoral (Cyclosporine Oral Solution)
- Goodman & Gilman’s: The Pharmacological Basis of Therapeutics
- Clinical Pharmacokinetic Review – Cyclosporine

